
经阴道超声测量宫颈长度预测无症状双胎早产的诊断效能的Meta分析
2014-03-22 03:45贺瑶谦解丽梅
中国医科大学学报 2014年11期
贺瑶谦,解丽梅
(中国医科大学附属盛京医院超声科,沈阳110004)
经阴道超声测量宫颈长度预测无症状双胎早产的诊断效能的Meta分析
贺瑶谦,解丽梅
(中国医科大学附属盛京医院超声科,沈阳110004)
目的应用Meta分析的方法评价经阴道超声测量的宫颈长度预测无症状双胎早产的诊断效能。方法通过电子文献检索系统检索在中国期刊网,Cochrane library trials register,Medline,Embase,Science Citation Index Expanded上发表的有关应用宫颈长度预测双胎早产诊断效能的中英文文献,应用Meta-disc 1.4软件进行分析,计算加权阳性似然比(pooled LR+)、受试者工作特性曲线(SROC)曲线下面积(AUC)并进行比较。结果有21篇文献符合标准,在20~24周测量宫颈长度,以25 mm为界值时,预测34周前早产及以30 mm为界值时,预测35周前早产SROC曲线下面积均>90%;在20周之前测量宫颈长度,以15 mm为界值时及在20~24周测量宫颈长度,以20 mm为界值时预测34周之前的早产pooled LR+值均>10.0。在20~24周测量,当35 mm、25 mm、15 mm为界值时预测28~37周之前早产的pooled LR+值依次为1.638~2.322、4.175~7.734、12.478~26.433。结论经阴道超声测量宫颈长度,在20~24周测量,以25 mm为界值时,预测34周前早产的准确率较高;以30 mm为界值时,预测35周前早产的准确率较高。宫颈长度与早产的pooled LR+值成反比,即宫颈长度越短,pooled LR+值越大。
宫颈长度;经阴道超声;双胎;早产;Meta分析
早产是造成新生儿死亡和患病的重要原因之一,尤其对双胎而言,对母婴的危害更大,早产率更高[1,2]。因此,预测双胎早产显得尤为重要,有早产危险者有必要进行产前干预降低早产风险,改善新生儿预后[3]。国外的一些研究已经证明经阴道超声测量宫颈长度是预测早产的有效参数之一,但在孕期何时测量宫颈长度及发生早产的医学参考界值的结论不统一[4~8]。本研究采用Meta分析方法评价阴道超声测量宫颈长度预测无早产症状的双胎自发性早产的诊断效能。
1 材料与方法
1.1 文献检索及筛选
通过电子文献检索系统检索1992-2013年在Cochrane library trials register,Medline,Embase,Science citation index expanded和中国期刊网CNKI上发表的有关双胎、宫颈长度、早产的相关中英文文献。英文检索词为(1)twins;(2)cervical OR cervix length OR neck of uterus OR uterine;(3)preterm OR premature OR delivery OR labo(u)r OR birth。中文检索词为“双胎”、“宫颈长度”、“早产”,并通过参考文献检索和手工检索来补充可能遗漏的文献。
1.2 文献纳入及排除标准
纳入标准:(1)可直接或间接获得诊断试验的原始数据,如真阳性数(true positive,TP)、假阳性数(false positive,FP)、真阴性数(true negative,TN)及假阴性数(false negative,FN);(2)病例数≥18例;(3)发表文种仅限于英文以及中文;(4)妊娠期间未经过治疗。
排除标准:(1)综述类文献、信件、评论、会议记录及病例报告;(2)样本含量<18例;(3)数据不全,无法获得真假、阳性数及真、假阴性数;(4)数据重复发表;(5)妊娠期间经过治疗。
1.3 数据提取
分别提取每篇纳入文献的特征(作者、发表年份、研究类型、文献质量)、技术参数(样本量、测量时间、界值、早产时间)、诊断试验信息参数(病例数、真阳性数、假阳性数、假阴性数、真阴性数、阳性预测值及阴性预测值)。技术参数信息包括:(1)宫颈长度测量的时间分为3组:20周前、20~24周、24周后;(2)宫颈长度的界值分组:15 mm、20 mm、25 mm、30 mm、35 mm;(3)早产时间<28周、<30周、<32周、<33周、<34周、<35周、<36周、<37周。
1.4 文献质量评估
使用最新的诊断试验质量评价工具——QUADAS-2[9,10]进行文献质量评估。
1.5 统计学分析
1.5.1 异质性检验:用I2评估异质性的大小,I2≤25%则研究结果间异质性较小,25%<I2≤50%为中等度异质性,I2>50%则存在高度异质性。若研究间同质,则采用固定效应模型(fixed-effects model,FEM),若研究间具有异质性,则采用随机效应模型(random-effects model,REM)。
1.5.2 计算合并统计量:采用Meta-disc1.4软件对纳入文献进行统计学处理,P<0.05认为差异有统计学意义。计算加权阳性似然比、受试者工作特性曲线(summary receiver operating characterist,SROC)曲线下面积(area under curve,AUC),所有结果均用95%可信区间表示。
1.5.3 绘制SROC曲线:若SROC曲线下面积AUC≤50%,表明该诊断试验无意义;50%~70%表明诊断的准确率较低;71%~90%表明诊断准确率中等;>90%表明诊断准确率较高。当阳性似然比(pooled LR+)>10或阴性似然比<0.1时,诊断或排除某种疾病的可能性就显著增加。
2 结果
2.1 文献检索结果
共检索到相关英文文献209篇,中文文献44篇,通过阅读标题和摘要排除了英文文献183篇,中文31篇,再由2名研究员独立阅读其余文献(共39篇:英文26篇,中文13篇),应用上述纳入及排除标准对文献进行筛选,排除的文章中有5篇文献原始数据无法提出,4篇文献采取的界值与其他文献不同;3篇文献重复发表;5篇是经腹或经会阴彩超;1篇是Meta分析。最终21篇文献纳入本研究(英文19篇[11~29],中文2篇[30~31])。
2.2 文献特征及质量评估结果
本研究纳入的21篇文献分析结果显示,10篇为前瞻性研究[12,14~16、18~22,29],3篇为回顾性研究[13,23,25],另外8篇文章未明确提出研究类型,发表时间截止2013年12月31日。测量的时间有2篇在20周之前,有14篇在20~24周之间,有7篇在24周之后。所选的宫颈长度界值有4篇是15 mm,10篇是20 mm,14篇是25 mm,7篇是30 mm,10篇是35 mm。早产的时间有6篇为28周之前,7篇为30周之前,10篇为32周之前,3篇为33周之前,8篇为34周之前,5篇为35周之前,1篇为36周之前,6篇为37周之前。样本量18~1 135例。根据诊断试验质量评价工具QUADAS-2评价,3篇评为A级,9篇评为B级,9篇为C级,见表1。
2.3 评价资料异质性及Meta分析结果
Meta-disc1.4软件输出结果SROC平面散点图均呈非典型的“肩臂形”分布,表明不存在阈值效应引起的异质性。对其他来源的异质性进行检验,结果发现:各研究间I2均>50%,即存在中度或高度异质性,需采用随机效应模型进行汇总分析。
在20~24周测量宫颈长度,以25 mm为界值时,预测28周、30周、32周、34周之前早产的SROC曲线下面积分别为0.964 2、0.928 4、0.904 1、0.920 2,以30 mm为界值时,预测35周之前早产的SROC曲线下面积为0.957 3,均>90%,表明诊断早产的准确率较高;在20~24周测量宫颈长度,以30 mm为界值时,预测32周、34周之前早产及在24周之后测量宫颈长度,以20 mm、25 mm为界值时,预测35周早产的SROC曲线下面积在71%~90%之间;在20~24周测量宫颈长度,以20 mm、35 mm为界值时,预测32周、34周早产的SROC曲线下面积在50%~70%之间(表2、3)。

表1 文献的特征Tab.1 Characteristics of documents
在20~24周测量宫颈长度,以15 mm为界值时预测28周、30周、32周、33周、34周之前早产的pooled LR+值分别为20.404、26.433、24.415、14.04、12.47,均>10.0,表明早产的可能性较大;在20周之前测量宫颈长度,以20 mm为界值时,预测28周、30周、32周、34周之前早产的pooled LR+值分别为20.976、32.926、28.267、30.943,也均>10.0,表明早产的可能性较大。
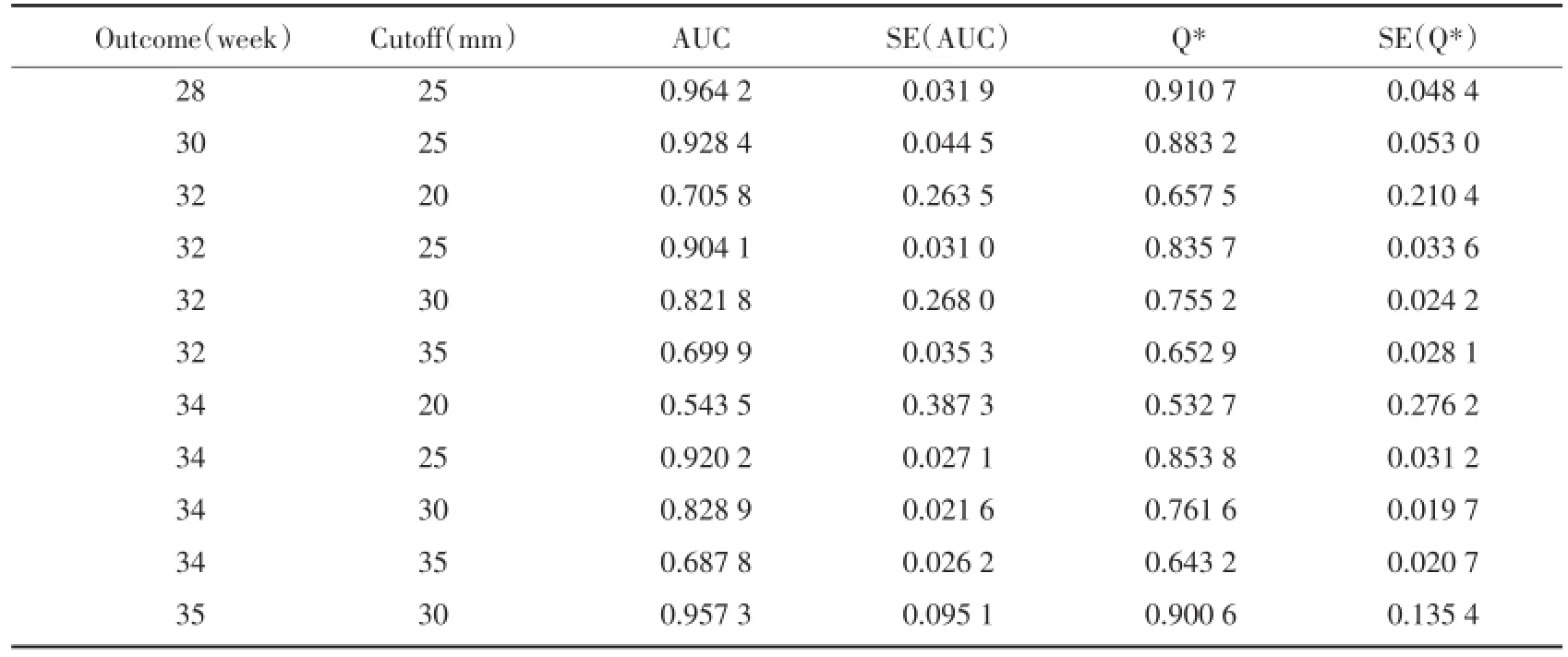
表2 20~24周时测量宫颈长度的结果Tab.2 Results of CL testing at 20⁃24 weeks′gestation

表3 24周后测量宫颈长度的结果Tab.3 Result of CL testing after 24 weeks′gestation
在20~24周测量宫颈长度的研究较多,故以此测量时间为例,当35 mm为界值时预测28~37周之前早产的pooled LR+值为1.638~2.322,当25 mm为界值时预测早产的pooled LR+值为4.175~7.734,当15 mm为界值时(除36周的pooled LR+值是4.063外),预测早产的pooled LR+值为12.478~26.433,从总体上来看,随着宫颈长度的缩短,pooled LR+值越大,即宫颈长度与早产的pooled LR+值成反比。
3 讨论
本研究的Meta分析表明应用经阴道超声测量宫颈长度是预测无症状双胎早产很好的方法。在20~24周测量,当宫颈长度界值是25 mm时,预测34周之前早产及当宫颈长度界值是30 mm时,预测35周之前早产的SROC曲线下面积均>90%,表明诊断准确率较高;当宫颈长度界值是20 mm、30 mm、35 mm时预测34周之前早产及在24周后测量,当宫颈长度界值是20 mm、25 mm时预测35周之前早产的SROC曲线下面积在50%~90%之间,表明诊断准确率中等或较低。因纳入研究的各个文献中,测量时间多是在20~24周,界值也多在20~35mm之间,对于测量时间在20周之前与24周之后的文献较少,一部分未形成有效的SROC曲线。在20~24周测量宫颈长度,当界值是15 mm时预测34周之前早产及在20周之前测量,界值是20 mm时预测34周前早产的pooled LR+值均>10.0,表明早产的可能性较大,但界值为15 mm、20 mm的研究较少,多少于3篇,有的仅有1篇,但因其LR+值>10.0,虽入选分析的文献较少,但也应引起临床医师足够的重视,必要时给予适当的早期干预治疗。
Conde-Agudelo[6]2010年发表文章对16篇文献中的3 213例无症状双胎早产进行Meta分析,其研究结果是在20~24周测量,当界值是20 mm时,预测32周及34周前早产的LR+是10.1和9.0;当界值是25 mm时,预测28周前早产的LR+是9.6;当界值是25 mm时,预测28周前早产的ROC曲线下面积是0.86,当界值是20 mm及25 mm时,预测32周前早产的均是0.80,当界值是20 mm及35 mm时,预测34周前早产的均是0.77,但是该研究将35周早产归入到34周,36周早产归入到37周分析。而本次Meta分析将早产的时间细分为28周、30周、32周、33周、34周、35周、36周、37周,最大程度上忠实于原研究,并未将相近时间做归类处理,得出的结论较为真实,但也造成了部分组中的文章篇数较少,不能形成有效的SROC曲线,故需要更多的临床研究。
本研究应用Meta分析的方法分析经阴道超声测量宫颈长度来预测双胎早产,国外有少量相关报道外,在国内尚属首次,原因也在于对于经阴式孕检的检查方法的抵触,误认为易造成早产,但鉴于阴式彩超的宫颈显示率高,图像不受胎儿影响,较腹式测量更准确,更优越,该方法应给予重视并进行推广。
本研究使用最新的诊断试验质量评价工具——QUADAS-2进行文献质量评估,和其他Meta文章一样,也有局限性,受入选文章质量的制约,主要是大部分研究不是在盲法下进行的,另外由于检索语种只限于中文与英文、未获取未发表的文献且获得阳性结果的文章较阴性结果的文章更容易发表,因而不能排除发表偏倚;各文献提供的信息及样本量有限,未能进行更深入亚组分析。本研究对敏感度和特异度的合并均存在一定程度的统计学异质性,由于系统综述是将临床和方法学上相似的研究进行合并,受诊断技术、文献质量及纳入标准的影响,异质性是不可避免的。
[1]Branum AM,Schoendorf KC.Changing patterns of low birth weight and preterm birth in the United States[J].Paediatr Perinat Epidemiol,2002,16(1):8-15.
[2]Mac Dorman MF,Hoyert DL,Mathews TJ.Recentdeclines in infant mortality in the United States,2005-2011[J].NCHS Data Brief,2013,4(120):1-8.
[3]Goldenberg RL,Culhane JF,Iams JD,et al.Epidemiology and causes of preterm birth[J].Lancet,2008,371(9606):75-84.
[4]Lim AC,Hegeman MA,Huis In′T Veld MA,et al.Cervical length measurement for the prediction of preterm birth in multiple pregnancies:a systematic review and bivariate Meta-analysis[J].Ultrasound Obstet Gynecol,2011,38(1):10-17.
[5]Aboulghar MM,Aboulghar MA,Mourad L,et al.Trasound cervical measurement and prediction of spontaneous preterm birth in ICSI pregnancies:a prospective controlled study[J].Reprod Biomed Online,2009,18(2):296-300.
[6]Conde-Agudelo A,Romero R,Hassan SS,et al.Transvaginal sonographic cervical length for the prediction of spontaneous preterm birth in twin pregnancies:a systematic review and Metaanalysis[J]. Am J Obstet Gynecol,2010,203(2):128.e1-12.
[7]Honest H,Bachmann LM,Coomarasamy A,et al.Accuracy of cervical transvaginal sonography in predicting preterm birth:a systematic review[J].Ultrasound Obstet Gynecol,2003,22(3):305-322.
[8]Makrydimas G,Sotiriadis A.Prediction of preterm birth in twins[J]. Best Pract Res Clin Obstet Gynaecol,2014,28(2):265-272.
[9]邬兰,张永,曾宪涛.QUADAS-2在诊断准确性研究的质量评价工具中的应用[J].湖北医药学院学报,2013,32(3):201-208.
[10]Whiting PF,Rutjes AWS,Westwood ME,et al.QUADAS-2:A revised tool for the quality assessment of diagnostic accuracy studies[J].Ann Intern Med,2011,155(8):529-536.
[11]Ong S,Smith A,Smith N,et al.Cervical length assessment in twin pregnancies using transvaginal ultrasound[J].Acta Obstet Gynecol Scand,2000,79(10):851-853.
[12]Souka AP,Heath V,Flint S,et al.Cervical length at 23 weeks in twins in predicting spontaneous preterm delivery[J].Obstet Gynecol,1999,94(3):450-454.
[13]Fait G,Har-Toov J,Gull I,et al.Cervical length,multifetal pregnancy reduction,and prediction of preterm birth[J].J Clin Ultrasound,2005,33(7):329-332.
[14]Vayssière C,Favre R,Audibert F,et al.Cervical length and funneling at 22 and 27 weeks to predict spontaneous birth before 32 weeks in twin pregnancies:A French prospective multicenter study[J].Am J Obstet Gynecol,2002,187(6):1596-1604.
[15]Arabin B,Roos C,Kollen B,et al.Comparison of transvaginal sonography in recumbent and standing maternal positions to predict spontaneous preterm birth in singleton and twin pregnancies[J]. Ultrasound Obstet Gynecol,2006,27(4):377-386.
[16]Sperling L,Kiil C,Larsen LU,et al.How to identify twins at low risk of spontaneous preterm delivery[J].Ultrasound Obstet Gynecol,2005,26(2):138-144.
[17]Imseis HM,Albert TA,Iams JD.Identifying twin gestations at low risk for preterm birth with a transvaginal sonographic cervical measurement at 24 to 26 weeks′gestation[J].Am J Obstet Gynecol,1997,177(5):1149-1155.
[18]To MS,Fonseca EB,Molina FS,et al.Maternal characteristics and cervical length in the prediction of spontaneous early preterm delivery in twins[J].Am J Obstet Gynecol,2006,194(5):1360-1365.
[19]Yang JH,Kuhlman K,Daly S,et al.Prediction of preterm birth by second trimester cervical sonography in twin pregnancies[J].Ultrasound Obstet Gynecol,2000,15(4):288-291.
[20]Skentou C,Souka AP,To MS,et al.Prediction of preterm delivery in twins by cervical assessment at 23 weeks[J].Ultrasound Obstet Gynecol,2001,17(1):7-10.
[21]Gibson JL,Macara LM,Owen P,et al.Prediction of preterm delivery in twin pregnancy:a prospective,observational study of cervical length and fetal fibronectin testing[J].Ultrasound Obstet Gynecol,2004,23(6):561-566.
[22]Fox NS,Rebarber A,Klauser CK,et al.Prediction of spontaneous preterm birth in asymptomatic twin pregnancies using the change in cervical length over time[J].Am J Obstet Gynecol,2010,202(2):155.e1-4.
[23]Fox NS,Saltzman DH,Klauser CK,et al.Prediction of spontaneous preterm birth in asymptomatic twin pregnancies with the use of combined fetal fibronectin and cervical length[J].Am J Obstet Gynecol,2009,201(3):313.e1-5.
[24]Klein K,Gregor H,Hirtenlehner-Ferber K,et al.Prediction of spontaneous preterm delivery in twin pregnancies by cervical length at mid-gestation[J].Twin Res Hum Genet,2008,11(5):552-557.
[25]Schwartz R,Prieto J.Shortened cervical length as a predictor of preterm delivery in twin gestations[J].J Reprod Med,2010,55(3-4):147-150.
[26]Goldenberg RL,Iams JD,Miodovnik M,et al.The preterm prediction study:risk factors in twin gestations.National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network[J].Am J Obstet Gynecol,1996,175(4):1047-1053.
[27]Soriano D,Weisz B,Seidman DS,et al.The role of sonographic assessment of cervical length in the prediction of preterm birth in primigravidae with twin gestation conceived after infertility treatment[J].Acta Obstet Gynecol Scand,2002,81(1):39-43.
[28]Crane JM,Van den Hof M,Armson BA,et al.Transvaginal ultrasound in the prediction of preterm delivery:singleton and twin gestations[J].Obstet Gynecol,1997,90(3):357-363.
[29]Guzman ER,Walters C,O′reilly-Green C,et al.Use of cervical ultrasonography in prediction of spontaneous preterm birth in twin gestations[J].Am J Obstet Gynecol,2000,183(5):1103-1107.
[30]温岩,孙晓艳,贾君容.胎儿纤连蛋白与宫颈长度联合测定预测双胎妊娠自发早产的价值[J].中国实验诊断学,2011,15(8):1392-1393.
[31]易清华,凌晟荣,黄晓燕.胎儿纤维连接蛋白联合宫颈长度检测对双胎妊娠早产的预测价值[J].中国妇幼保健,2011,26(24):3807-3809.
(编辑 武玉欣)
Meta Analysisof Predicting Preterm Birth in Asymptomatic Twin Pregnancy with Transvaginal Sonographic MeasurementofCervicalLength
HEYao-qian,XIE Li-mei
(DepartmentofUltrasound,Shengjing Hospital,China MedicalUniversity,Shenyang 110004,China)
ObjectiveTo assess the accuracy of transvaginal sonographic cervical length(CL)in predicting preterm birth in asymptomatic women with twin pregnancies.MethodsA comprehensive literature search was performed in CNKI,The Cochrane Library trials register,Medline,Embase,Science Citation Index Expanded and the references were listed.The diagnostic accuracy ofCL to predictpreterm birth in asymptomatic women with twin pregnancieswere investigated.Pooled LR+and the area underthe SROCcurve were calculated by Meta-disc 1.4 software.ResultsTwentyone studies metthe inclusion criteria.Atthe time of20-24 weeks′gestation,a CL≤25 mm in predicting preterm birth<34 weeks′gestation and a CL≤30 mm in predicting preterm birth<35 weeks′gestation,the area under the SROC curve were more than 90%.A CL≤15 mm before 20 weeks′gestation and a CL≤20 mm at 20-24 weeks′gestation in predicting preterm birth<34 weeks′gestation,the pooled LR+were more than 10.0.At 20-24 weeks′gestation,a CL≤35 mm,25 mm,15 mm in predicting preterm birth between 28 and 34 weeks′gestation,the pooled LR+were 1.638-2.322,4.175-7.734,12.478-26.433,respectively.ConclusionTransvaginal sonographic CL at 20-24 weeks′gestation,a CL≤25 mm was more accurate in predicting preterm birth<34 weeks′gestation,and a CL≤30 mm was more accurate in predicting preterm birth<35 weeks′gestation.CLwas inversely related to pooled LR+ofpreterm birth,which means the shorterofCL,the largernumericalofpooled LR+.
cervical length;transvaginal sonographic;twins;prediction;metaanalysis
R445.1;R714.2
A
0258-4646(2014)11-1023-05
贺瑶谦(1981-),女,主治医师,硕士研究生.
解丽梅,E-mail:xielm72@sohu.com
2014-06-23
网络出版时间:
猜你喜欢
今日农业(2021年10期)2021-11-27
中国生殖健康(2020年5期)2021-01-18
宝藏(2020年4期)2020-11-05
中国生殖健康(2020年6期)2020-02-01
中国生殖健康(2019年2期)2019-08-23
中国生殖健康(2019年2期)2019-08-23
幸福(2019年12期)2019-05-16
中国老年保健医学(2018年6期)2019-01-14
中国生殖健康(2018年6期)2018-11-06
中国妇幼健康研究(2017年12期)2018-01-31
