地塞米松对胃肠手术患者术后血清皮质醇浓度的影响
2015-03-21 02:44陈镜伊刘艳红
解放军医学院学报 2015年6期
陈镜伊,刘艳红,张 宏
解放军总医院 麻醉手术中心,北京 100853
地塞米松对胃肠手术患者术后血清皮质醇浓度的影响
陈镜伊,刘艳红,张 宏
解放军总医院 麻醉手术中心,北京 100853
目的观察术前应用地塞米松对胃肠手术患者术后血清皮质醇浓度的影响。方法选择2013年11月- 2014年7月在我院麻醉手术中心行胃肠手术的患者80例,随机分成对照组(C组)和地塞米松组(D组),每组40例。术前1 ~ 2 h,C组静脉注射0.9%氯化钠注射液2 ml,D组静脉注射地塞米松10 mg(2 ml)。分别在术前(T0)、术后第1天(T1)及第7天(T2)抽取外周静脉血测量血清皮质醇浓度。结果术前及术后第7天两组血清皮质醇浓度差异均无统计学意义(P>0.05)。术后第1天D组血清皮质醇浓度为345.8 nmol/L,C组为832.8 nmol/L,D组低于C组(P<0.05)。与术前相比,C组术后第1天血清皮质醇浓度明显升高(P<0.05),D组无明显变化(P>0.05)。结论术前应用10 mg地塞米松可以抑制胃肠手术患者术后皮质醇的过度产生,术后第1天血清皮质醇浓度较术前无明显变化,术后早期血清皮质醇浓度相对稳定。
地塞米松;皮质醇;胃肠手术
大量研究已表明,术前应用地塞米松可以有效减轻患者术后恶心呕吐的发生[1],还可以减缓胃肠手术患者术后疲倦及疼痛,促进术后恢复[2]。地塞米松作为皮质类固醇激素,可以作用于下丘脑-垂体-肾上腺皮质(hypothalamus-pituitary-adrenocortical,HPA)轴,负反馈抑制肾上腺皮质产生皮质醇[3]。目前尚无文献报道临床上常规剂量(10 mg)地塞米松对胃肠手术患者术后皮质醇浓度的影响如何。本研究旨在观察术前1 ~ 2 h静脉注射地塞米松对胃肠手术患者术后血清皮质醇浓度的影响。
资料和方法
1 一般资料 选择2013年11月- 2014年7月在我院麻醉手术中心行胃肠手术的患者80例,美国麻醉医师协会(American Society of Anesthesiologists,ASA)评级为Ⅱ~Ⅲ级。排除标准:有严重的心、肺、肝、肾、脑、内分泌病史,术前长期使用类固醇激素,术前皮质醇浓度超过正常参考值范围(198.7 ~797.5 nmol/L),对地塞米松过敏。采用随机数字表法分为对照组(C组)和地塞米松(D组),每组40例。
2 用药及麻醉 患者入手术室后开通静脉通路,常规监测心率、血压、脉搏氧饱和度及心电图。术前1 ~ 2 h,C组静脉注射0.9%氯化钠注射液2 ml,D组静脉注射地塞米松10 mg(2ml)。全麻诱导:丙泊酚1.0 ~ 1.5 mg/kg,罗库溴铵0.6 ~ 0.8 mg/kg、咪达唑仑0.02 ~ 0.03 mg/kg和芬太尼2 ~ 3 μg/kg。气管插管后连接麻醉机行机械通气,维持PaCO2在35 ~ 45 mmHg(1 mmHg= 0.133 kPa)。连续监测有创动脉血压,使其波动幅度不超过基础值的25%。术中持续泵注异丙酚、瑞芬太尼及吸入七氟醚维持麻醉,控制脑电双频指数(bispectralindex,BIS)值为40 ~ 60。术中根据需要静注罗库溴铵及芬太尼,手术结束停止麻醉用药。
3 血标本采集及检测 分别在术前、术后第1天及第7天从外周静脉抽取血样3 ml,静置1 ~ 2 h后在4 000 r/min下离心15 min,取血清保存在-80℃冰箱中,用化学发光免疫分析法检测血清皮质醇浓度。
4 统计学分析 统计分析采用SPSS15.0软件。计量数据用或中位数(最小值-最大值)表示。组间比较用t检验或Wilcoxon秩和检验,组内比较用方差分析,定性资料比较用χ2检验。P<0.05为差异有统计学意义。
结 果
1 一般情况比较 两组患者年龄、性别、体质量、身高、ASA分级、估计术中出血量、手术时间差异均无统计学意义(P>0.05)。见表1。
2 血清皮质醇浓度比较 术前、术后第7天两组血清皮质醇浓度差异均无统计学意义(P>0.05)。术后第1天,D组血清皮质醇浓度较C组低(345.8 nmol/L vs 832.8 nmol/L)(P<0.05)。C组术后第1天血清皮质醇浓度较术前显著升高(P<0.05),术后第7天和术前比较差异无统计学意义(P>0.05)。D组术后第1天、第7天与术前比较,差异均无统计学意义(P>0.05)。见表2。
表1 80例患者基本资料Tab. 1 Clinical data about 80 patients included in this study ()
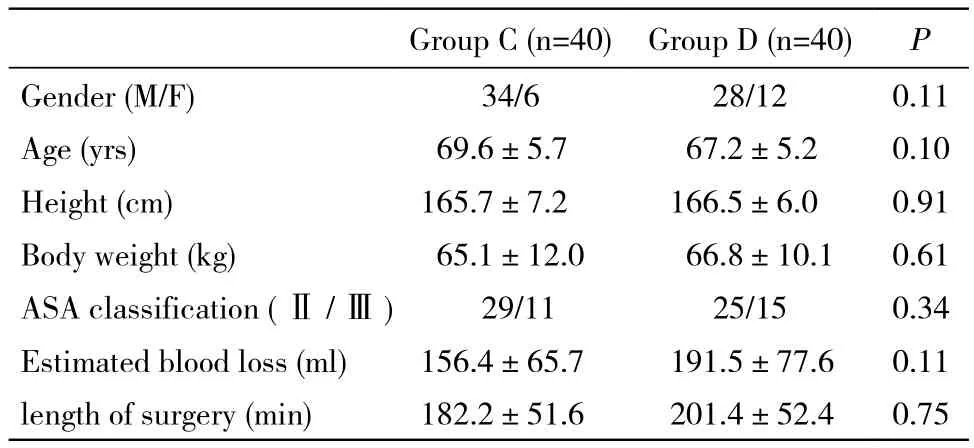
表1 80例患者基本资料Tab. 1 Clinical data about 80 patients included in this study ()
Group C (n=40)Group D (n=40)P Gender (M/F)34/628/120.11 Age (yrs)69.6±5.767.2±5.20.10 Height (cm)165.7±7.2166.5±6.00.91 Body weight (kg)65.1±12.066.8±10.10.61 ASA classification (Ⅱ/Ⅲ)29/1125/150.34 Estimated blood loss (ml)156.4±65.7191.5±77.60.11 length of surgery (min)182.2±51.6201.4±52.40.75
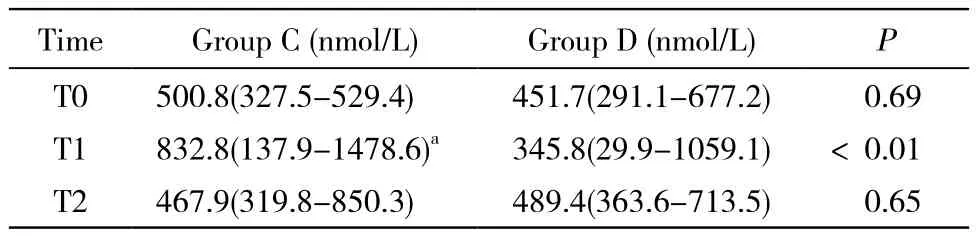
表2 两组患者血清皮质醇浓度比较Tab. 2 Comparison of serum levels of cortisol between the two groups (median)
讨 论
本研究表明,在接受胃肠手术患者中,术前给予临床常用剂量(10 mg)地塞米松可以降低术后第1天血清皮质醇浓度,但与术前无明显差异,血清皮质醇浓度较平稳。
糖皮质激素具有抗炎及免疫调节作用,地塞米松是人工合成的糖皮质激素,抗炎作用强,作用时间长,被广泛应用于临床[4]。手术会引起以炎症反应及内分泌改变为主的一系列应激反应,过度应激会使机体代谢增强,各器官营养需求增加,这也许会导致术后患病率增加[5-6]。多数研究表明,术前单剂量(8 ~ 10 mg)地塞米松可以有效降低患者循环中炎症因子浓度,减轻术后恶心呕吐、疼痛,减缓术后疲倦,促进术后肺功能恢复等[2,7-10]。因此现在临床上术前应用地塞米松非常普遍。
手术创伤引起HPA轴活动增强,患者循环皮质醇浓度增高[11],可引起骨骼肌萎缩、骨质疏松、皮肤变薄、淋巴组织萎缩、海马退化、血管并发症等不良反应[12-13]。Crema等[14]研究发现,在胆囊切除术的患者中,术后第1天血清皮质醇浓度显著高于术前。本研究发现,对照组患者术后第1天时血清皮质醇浓度显著高于术前水平,这和之前Crema等得出的结果相似。有文献报道,成年人在非应激状态下每天产生的皮质醇含量为10 ~20 mg,但在手术创伤应激状态下产生的皮质醇量急剧增加,为10 ~ 15 mg/h[15]。地塞米松生物效能为皮质醇的25倍[7],那么术前应用10mg地塞米松对患者循环皮质醇浓度影响如何?目前为止研究甚少。Elston等[16]发现,健康成年人在非应激状态下(非手术创伤刺激),静脉注射8 mg地塞米松后第1天循环皮质醇浓度被抑制到基础水平(应用地塞米松之前)的5%左右。本研究发现,术前应用10 mg地塞米松的患者术后第1天血清皮质醇浓度虽低于术前,但差异无统计学意义,然而术前未注射地塞米松的患者术后第1天血清皮质醇浓度较术前显著升高(P<0.05)。这与手术本身引起的应激反应导致皮质醇增多有关,地塞米松的抑制作用一定程度上抵消了手术应激引起的皮质醇浓度升高部分,使得循环皮质醇浓度相对平稳。两组患者术后第7天血清皮质醇浓度和术前相比,均无明显差异,这说明术后第7天患者HPA轴功能基本恢复至术前水平,并且地塞米松的抑制作用也已消失。
地塞米松通过和细胞内受体结合影响细胞转录而发挥生物效应,起效时间较慢,为1 ~ 2 h[17],为充分获得其治疗效益,选择在手术开始切皮刺激前1 ~ 2 h静脉注射。
本研究中,术后第1天地塞米松组患者与对照组相比,血清皮质醇浓度明显降低,说明肾上腺皮质功能在一定程度上被抑制,但与术前相比却无明显差异。然而我们仅仅观察了血清指标的变化,并未观察这种变化对患者的恢复影响如何,所以并不能说明临床上这种地塞米松对皮质醇反应的抑制作用对患者是有利还是有害。Henzi等[18]通过对一系列文献进行总结后发现,抗吐剂量的地塞米松对手术患者并未产生任何明显的不良反应,若从过度应激(皮质醇浓度过高)影响患者恢复的理论来看,可以大胆的提出术前10 mg地塞米松对肾上腺皮质功能的抑制是一种保护作用。本研究观察的术后时间点较少,并未记录皮质醇浓度的连续变化,以后我们会做更多关于术前应用地塞米松对患者预后影响及相关机制的研究,为临床应用提供参考意见。
1 王亮.3种药物联合对腹腔镜子宫肌瘤剔除术后自控镇痛患者恶心呕吐的疗效观察[J].当代医学,2014,20(15):132-132.
2 Zargar-Shoshtari K, Sammour T, Kahokehr A, et al. Randomized clinical trial of the effect of glucocorticoids on peritoneal inflammation and postoperative recovery after colectomy[J]. Br J Surg, 2009, 96(11):1253-1261.
3 Martin NM, Dhillo WS, Banerjee A, et al. Comparison of the dexamethasone-suppressed corticotropin-releasing hormone test and low-dose dexamethasone suppression test in the diagnosis of Cushing’s syndrome[J]. J Clin Endocrinol Metab, 2006, 91(7):2582-2586.
4 张冠中,焦顺昌,杨纪华.培美曲塞单药或联合铂类治疗非小细胞肺癌86例分析[J].解放军医学院学报,2013,34(4):319-321.
5 Desborough JP. The stress response to trauma and surgery[J]. Br J Anaesth, 2000, 85(1): 109-117.
6 薛霞,薛红,李卫东,等.高正加速度应激对人体唾液睾酮及皮质醇的影响[J].解放军医学院学报,2013,34(11):1189-1191.
7 Holte K, Kehler H. Perioperative single-dose glucocorticoid administration: Pathophysiologic effects and clinical implications [J]. J Am Coll Surg, 2002, 195(5): 694-712.
8 De Oliveira GS Jr, Almeida MD, Benzon HT, et al. Perioperative single dose systemic dexamethasone for postoperative pain: a metaanalysis of randomized controlled trials[J]. Anesthesiology, 2011,115(3):575-588.
9 Sistla S, Rajesh R, Sadasivan J, et al. Does single-dose preoperative dexamethasone minimize stress response and improve recovery after laparoscopic cholecystectomy?[J]. Surg Laparosc Endosc Percutan Tech, 2009, 19(6):506-510.
10 Karanicolas PJ, Smith SE, Kanbur B, et al. The impact of prophylactic dexamethasone on nausea and vomiting after laparoscopic cholecystectomy a systematic review and Meta-Analysis[J]. Ann Surg, 2008, 248(5): 751-762.
11 Karaman K, Bostanci EB, Aksoy E, et al. Effects of dexamethasone and pheniramine hydrogen maleate on stress response in patients undergoing elective laparoscopic cholecystectomy[J]. Am J Surg,2013, 205(2):213-219.
12 Takagi S, Tanabe A, Tsuiki M, et al. Hypokalemia, diabetes mellitus, and hypercortisolemia are the major contributing factors to cardiac dysfunction in adrenal Cushing's syndrome[J]. Endocr J,2009, 56(8):1009-1018.
13 唐志清,朱笑笑,王先令,等.正常血钾和伴低血钾库欣病患者心脑血管并发症和临床特点的比较[J] .解放军医学院学报,2013,34(7):693-695.
14 Crema E, Ribeiro EN, Hial AM, et al. Evaluation of the response of cortisol, corticotropin and blood platelets kinetics after laparoscopic and open cholecystectomy[J]. Acta Cir Bras, 2005, 20(5):364-367.
15 Kraan GP, Dullaart RP, Pratt JJ, et al. The daily cortisol production reinvestigated in healthy men. The serum and urinary cortisol production rates are not significantly different[J]. J Clin Endocrinol Metab, 1998, 83(4):1247-1252.
16 Elston MS, Conaglen HM, Hughes C, et al. Duration of cortisol suppression following a single dose of dexamethasone in healthy volunteers: a randomised double-blind placebo-controlled trial[J]. Anaesth Intensive Care, 2013, 41(5):596-601.
17 Barnes PJ. Anti-inflammatory actions of glucocorticoids: molecular mechanisms[J]. Clin Sci, 1998, 94(6): 557-572.
18 Henzi I, Walder B, Tramer MR. Dexamethasone for the prevention of postoperative nausea and vomiting: A quantitative systematic review[J]. Anesth Analg, 2000, 90(1): 186-194.
Effects of dexamethasone on serum cortisol levels in patients undergoing gastrointestinal surgery
CHEN Jingyi, LIU Yanhong, ZHANG Hong
Anesthesiology and Operation Center, Chinese PLA General Hospital, Beijing 100853, China
ZHANG Hong. Email: mazuimao301@163.com
ObjectiveTo investigate the effects of preoperative administration of dexamethasone on serum levels of cortisol in patients undergoing gastrointestinal surgery.MethodsEighty patients scheduled for elective gastrointestinal surgery were included in this study, and they were randomly divided into control group (Group C) and dexamethasone group (Group D). Patients in Group C received 2 ml of normal saline 1-2 hour before surgery while patients in Group D received 10 mg of dexamethasone. Serum levels of cortisol were determined on the day before surgery (T0), post-operative day 1 (T1) and day 7 (T2).ResultsThere were no significant differences in serum cortisol levels on T0 and T1 between the two groups (P>0.05). Compared with Group C, Group D had significantly lower serum level of cortisol (345.8 nmol/L vs. 832.8 nmol/L, P<0.05) on T1. Compared with T0, patients in group C had significantly higher levels of cortisol on T1(P<0.05), while there were no differences between T0 and T1 in Group D (P>0.05).ConclusionPreoperative administration of 10 mg of dexamethasone can decrease the serum levels of cortisol on postoperative day 1, and shrink the fluctuation of serum levels of cortisol.
dexamethasone; cortisol; gastrointestinal surgery
R 614
A
2095-5227(2015)06-0580-03
10.3969/j.issn.2095-5227.2015.06.016
时间:2015-03-12 08:42
http://www.cnki.net/kcms/detail/11.3275.R.20150312.0842.002.html
2015-01-14
总后勤部卫生部保健专项课题(13BJZ38)
Supported by the Health Care Project of Health Ministy of General Logistic Department of PLA(13BJZ38)
陈镜伊,女,硕士。Email: cjy823957912@163.com
张宏,女,博士,主任医师,教授,博士生导师。Email: mazuimao301@163.com
猜你喜欢
中国急救医学(2022年2期)2022-11-15
中国药学药品知识仓库(2022年2期)2022-03-23
麻醉安全与质控(2021年4期)2021-06-29
云南医药(2020年5期)2020-10-27
基层中医药(2020年4期)2020-09-11
疯狂英语·新读写(2020年3期)2020-06-06
基层中医药(2018年9期)2018-11-09
中国体育教练员(2017年2期)2017-07-31
西南军医(2016年3期)2016-01-23
中国卫生标准管理(2015年2期)2016-01-14