
The likelihood of having serum level of PSA of‡4.0 ng/mL and‡10.0 ng/mL in non-obese and obese Nigerian men with LUTS
2015-05-16 01:33PatrikTemiAdegunPhilipBaatundeAdeayoSamuelAdeniranAtia
Asian Journal of Urology 2015年3期
Patrik Temi Adegun*,Philip Baatunde Adeayo, Samuel Adeniran Atia
aDepartment of Surgery,College of Medicine,Ekiti State University,Ado-Ekiti,Ekiti State,Nigeria
bDepartment of Medicine,Ladoke Akintola University of Technology,Ogbomoso,Nigeria
cDepartment of Chemical Pathology,College of Medicine,Ekiti State University,Ado-Ekiti,Ekiti State, Nigeria
The likelihood of having serum level of PSA of‡4.0 ng/mL and‡10.0 ng/mL in non-obese and obese Nigerian men with LUTS
Patrick Temi Adeguna,*,Philip Babatunde Adebayob, Samuel Adeniran Atibac
aDepartment of Surgery,College of Medicine,Ekiti State University,Ado-Ekiti,Ekiti State,Nigeria
bDepartment of Medicine,Ladoke Akintola University of Technology,Ogbomoso,Nigeria
cDepartment of Chemical Pathology,College of Medicine,Ekiti State University,Ado-Ekiti,Ekiti State, Nigeria
Objective:This study was undertaken to determine the likelihood of having serum total prostate specif i c antigen(PSA)levels?4.0 ng/mL and?10.0 ng/mL among a cohort of non-obese and obese Nigerian men with lower urinary tract symptoms(LUTS).
Lower urinary tract symptoms;
Men;
Nigeria;
Overweight;
Obesitythe same vein,non-obese men were less likely to have a PSA level of 10.0 ng/mL(OR,0.686; 95%CI,0.318e1.478)in a simultaneous context of age.
Conclusion:Our study demonstrated that,in a sample population of predominantly native African men,there was a non-signif i cantly higher likelihood of overweight/obese patients having a higher serum PSA level than the non-obese.A community based study is needed to further conf i rm this f i nding.
1.Introduction
Prostate speci fi c antigen(PSA)was reported to have been fi rst identi fi ed by researchers attempting to fi nd a substance in seminal fl uid that would aid in the investigation of rape cases[1].It was subsequently found to be able to identify prostate cancer(PCa)in men not known to have the cancer[2].Men with PCa generally have elevated PSA levels in their serum;this tumour marker is now frequently used for PCa screening,diagnosis and monitoring of response to therapy[3e8].
To improve treatment outcome,PSA has been developed which categorized patients into three;viz:(i)low risk disease(LRD),(ii)intermediate risk disease(IRD),and(iii) high risk disease(HRD)especially when combined with Gleason score and American Joint Commission on Cancer clinical tumour category so as to determine the outcome and suitability of various treatment modalities for PCa[9]. In such instances PSA level of<10.0 ng/mL was matched for LRD,PSA level of 10.0e20.0 ng/mL was matched for IRD while PSA of>20.0 ng/mL was matched for HRD[9].The low specif i city of PSA testing and questionable benef i ts of PSA screening on PCa mortality highlight the need for better detection strategies for PCa[10].
Some studies suggested that body weight(BW)and body mass index(BMI)have effect on serum PSA,while some other researchers hold contrary opinion[5e8,11].The variation of PSA levels with obesity in contemporary times poses a great challenge in the utilization of the marker for diagnosis.Establishing the relationship between PSA levels and obesity will detect the inf l uence of BMI in the interpretation and clinical evaluation of PSA results.Moreover, PSA levels differ between various ethnic groups and races [12].It is uncertain whether f i ndings from studies investigating the association between BMI and PSA conducted primarily in Western populations can be applied to other ethnic groups.
In our country where healthcare infrastructure is overstretched coupled with a rising prevalence of cardiovascular risk including obesity,knowledge of the inf l uence of concomitant co-morbidities such as obesity on serum PSA concentrations may improve the discriminant value of this test for predicting PCa and reduce the number of unnecessary biopsies and subsequent over-diagnosis of indolent cancers.In this study we examined the likelihood of having a serum PSA of?4.0 ng/mL and?10.0 ng/mL in obese and non-obese Nigerian men presenting with lower urinary tract symptoms(LUTS).
2.Patients and methods
2.1.Study site
This was a prospective hospital based cross-sectional observational study conducted at the urology clinic of Ekiti State University Teaching Hospital(EKSUTH),Ado-Ekiti,South-Western Nigeria.The study covered a period between 1st January and 31st December,2014.
2.2.Subject’s selection
One hundred and forty consecutive patients aged 40 years and above,who presented to urology clinic with LUTS within the study period were recruited.
However,the following categories of patients were excluded:
(i)those who have had digital rectal examination(DRE);
(ii)those who have had sexual intercourse within 24 h of examination;
(iii)those who have had recent catheterization or any other form of urologic manipulations;
(iv)those on 5-a-reductase inhibitor;
(v)those with a diagnosis of PCa;
(vi)those who have had prostate surgery or prostatitis;
(vii)those who did not give their consent;
(viii)All patients who had suspicious DRE or had PSA of ?10.0 ng/mL were subjected to prostate biopsy and were excluded if positive for cancer.
2.3.Ethical consideration
This study was approved by the Health Research and Ethics CommitteeofEKSUTH.Alltheparticipantswere adequately informed through written notice before the data were collected.
2.4.Data collection
2.4.1.Anthropometric variable
Height without shoes was measured to the nearest centimetre with a stadiometer(seca,Birmingham,UK)and weight in light clothing was measured to the nearest 0.1 kg, with a bathroom scale(Zhongshan Camry Electronic, Guangdong,China).BMI was calculated as a ratio of weight(kg)to height squared(m2).All anthropometric measurements were made by trained observers.The subjects were then classif i ed as non-obese(BMI<25 kg/m2)or obese[BMI ?25 kg/m2]according to Asian-Pacif i c classif i cation more suited for African community[13].
2.4.2.PSA assay
Normal laboratory procedures were complied with in carrying out PSA analysis.About 5 mL of blood sample was taken into the screwed cap plain specimen bottle for the laboratory analysis of PSA.The blood sample was left to retract for about 30 min.Each set of sample was centrifuged at 2500 g for 5 min after which serum was separated into another screwed cap plain specimen bottle.The serum was later kept frozen till analysis of that batch.Serum PSA was determined using ready-to-use enzyme immunoassay commercially manufactured kit(Teco Diagnostic Laboratory,USA).This was based on the principle that PSA molecule was sandwiched between solid phase(rabbit anti-PSA antibody)and enzyme linked antibodies(monoclonal anti-PSA conjugated to Horse raddish peroxidise)[14].
2.5.Statistical analysis
The mean and standard deviation were used as appropriate to describe normally distributed continuous data.Median and inter-quartile(IQ)ranges and ManneWhitney U-test were employed in analysing between group differences for skewed variables.A p-value was calculated using the independent t-test for continuous variables and the Pearson Chi-square test for categorical variables.Two separate PSA thresholds,?4.0 and?10.0 ng/mL,were used to categorize PSA values as“normal”or“abnormal”for the analyses.To describe the association between age,obesity and the likelihood of a certain serum total PSA level,multivariate analysis was used after dichotomising men as having a PSA level?4.0 or?10.0 ng/mL,respectively.The odds ratio (OR)of having an‘abnormal’PSA level for each threshold was then calculated,using overweight/obese men as the reference.The OR of having normal or abnormal PSA was also dichotomised between ages?65 years and<65 years with?65 years as the reference.The SPSS 17.0 software (SPSS Inc.,Chicago,IL,USA)was used for the statistical analyses and p<0.05 was considered statistically signif icant for all analyses.
3.Results
Table 1 shows the demographic characteristics of patients with LUTS.The mean ages of overweight/obese and nonobesemenwithLUTSwere64.00?11.26and 64.80?10.88 years respectively.There was no statistical difference between the mean ages(p>0.05).The median (IQ range)of the PSA level was 13.2(160.2)ng/mL for nonobese patients and 14.8(145.1)ng/mL for overweight/ obese group.The number of overweight/obese patients with PSA level?10 ng/mL was 64(61.5%)while 19(52.8%) non-obese patients had PSA?10.0 ng/mL.This was not statistically signif i cant even though greater proportion of obese patients had PSA?10 ng/mL.
Table 2 shows the multivariate logistic regression analysis of the relationship between age and BMI on serum PSA threshold of?4.0 ng/mL and?10.0 ng/mL.
Although there was no statistically signif i cant difference, non-obese patients were less likely to have PSA level of ?4.0 ng/mL(0.701)as shown in Model 1.Also,Model 1 shows that patients aged<65 years were 1.395 times likely to have a PSA?4.0 ng/mL compared to older patients.This f i nding was also not statistically signif i cant.Model 2 shows that patients aged<65 years were less likely to have a PSA value of?10.0 ng/mL compared with older patients,while nonobese patients were less likely to have a PSA?10.0 ng/mL.
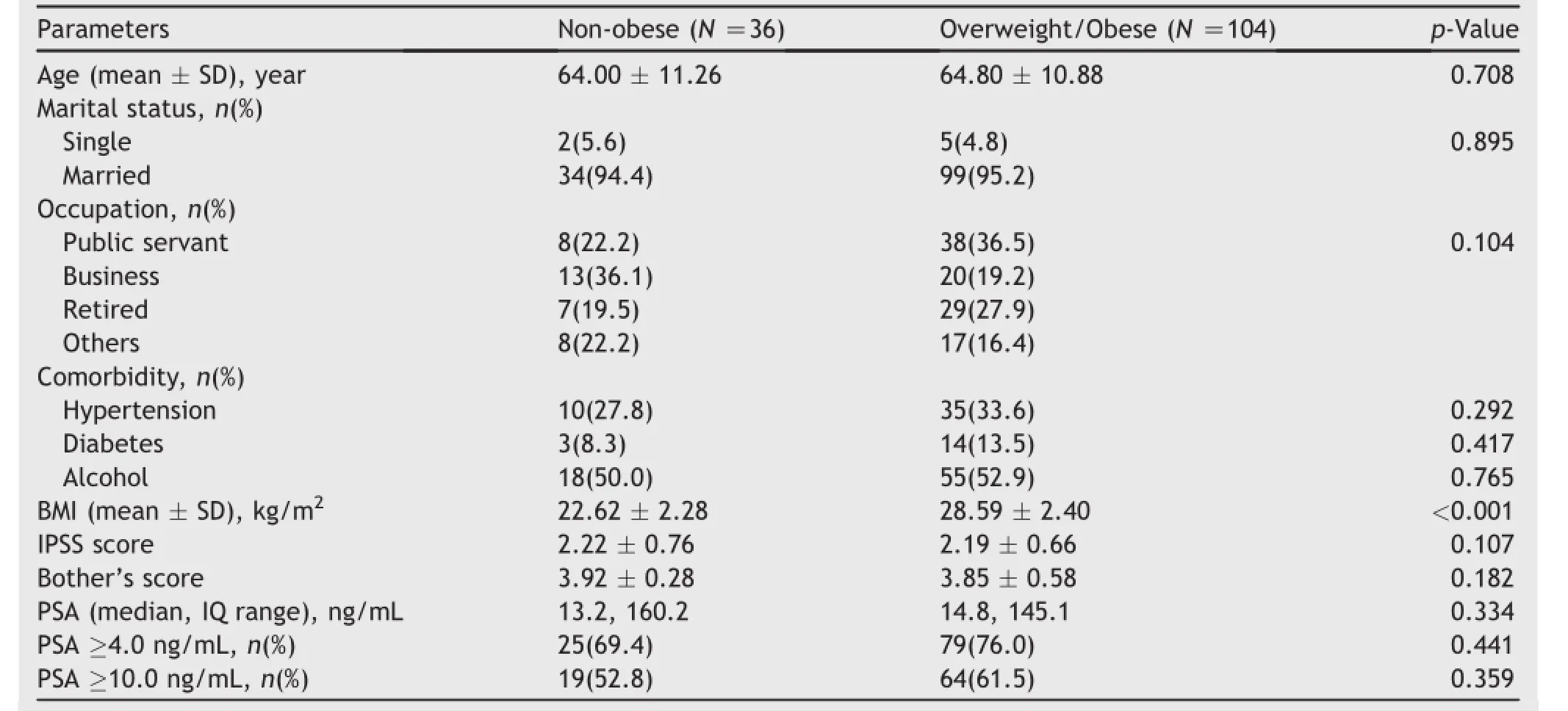
Table 1 The demographic and clinical characteristics of patients with LUTS.

Table2 Multivariate logistic regression showing predictors of PSA values of?4.0 ng/mL and?10.0 ng/mL.
4.Discussion
Having a serum PSA level of above 10.0 ng/mL has been associated with increasing risk of PCa and this has driven the increase in the use of PSA as screening marker for PCa [10].We sought to establish the effect of obesity on the likelihood of having serum PSA of 4.0 ng/mL(normal 0e4.0ng/mLandindicativeofPCa?10.0ng/mL) among Nigerian men with LUTS.When PSA thresholds of 4.0 ng/mL and 10.0 ng/mL were compared between non-obese and overweight/obese,we found that PSA threshold of 4.0 ng/mL and 10.0 ng/mL were prevalent among overweight/obese patients.Although this difference did not reach statistical signif i cance.
Ourmultivariatelogisticanalysisshowedanonstatistically signif i cant trend towards a higher likelihood of overweight/obese men having a total serum PSA level ?4.0 ng/mL and?10.0 ng/mL.When this threshold was considered,a trend of increasing PSA level with increasing BMI was noted.This is similar to the f i ndings of Loeb et al. [15]who found that total PSA increased with an increasing BMI in a cohort of nearly 600 men who underwent radical prostatectomy(RP)by a single surgeon[15].
Besides,when our threshold was considered,a trend of decreasing PSA level with increasing BMI could not be established.This f i nding is contrary to that of Curp and Porter[16]and some researchers who found a decreasing level of point estimates of abnormal PSA level with increasing BMI although the authors’studies were better powered.However,most of these studies were amongst men of cross-cultural origins,ranging from Hispanics to Koreans[17e19].In spite of this,Naito et al.[20]found that there was an increased serum PSA with Japanese men with higher normal BMI even though they also reported a lower PSA among the overweight/obese.Although the exact mechanism for lower PSA has not been fully elucidated,their f i ndings were based on the theory of hormonal hypothesis that suggested a possible interaction between body adiposity and steroid hormone metabolism[19].Other contributory postulation is that,men with a higher BMI could have larger plasma volumes,which could decrease serum concentrations of soluble tumour markers[21].All the above postulations are still subject of debate.
Moreover,it should be noted that PSA levels are inf l uenced by a number of demographic,lifestyle,and health characteristics,all of which deserve careful attention in the interpretation of test results[22].The association between BMI and PSA may vary according to population characteristics[12,23],and this may explain why this study is different from those conducted outside Africa.Therefore,the explanation for the f i nding in this study may be due to racial differences as a result of larger prostate size and higher mean PSA typical of the African race compared to others[24].However,our study is hospital based and less powered.Therefore,additional studies are needed to further clarify the relationships between BMI and PSA and determinewhetherweightreductioncouldleadto improved outcomes.
Our f i ndings imply that overweight/obesity could create a false positive screening cut-off level of PSA as a screening test for PCa.We suggest interpretation of PSA levels with clinical f i ndings and other diagnostic methods such as histopathology,DRE and imaging studies.
5.Conclusion
Our study demonstrated that in a sample population of predominantly native African men,there was a higher likelihood of overweight/obese patients of having higher PSA level;however,this association was washed off in a logistic regression analysis.Additional studies are needed to further clarify the links between BMI and PSA and to determinewhetherweightreductioncouldleadto improved level of serum PSA.
Conf l icts of interest
The authors declare no conf l ict of interest.
[1]Chia SE,Lau WK,Chin CM,Tan J,Ho SH,Lee J,et al.Effect of ageing and body mass index on prostate-specif i c antigen levels among Chinese men in Singapore from a community-based study.BJU Int 2009;103:1487e91.
[2]Catalona WJ,Smith DS,Ratliff TL,Dodds KM,Coplen DE, Yuan JJ,et al.Measurement of prostate-specif i c antigen in serum as a screening test for prostate cancer.N Engl J Med 1991;324:1156e61.
[3]Oesterling JE.Prostate specif i c antigen:a critical assessment of the most useful tumor marker for adenocarcinoma of the prostate.J Urol 1991;145:907e23.
[4]Consedine NS,Morgenstern AH,Kudadjie-Gyamf iE,Magai C. Neugut AI.Prostate cancer screening behavior in men from seven ethnic groups:the fear factor.Cancer Epidemiol Biomarkers Prev 2006;15:228e37.
[5]Banez LL,Hamilton RJ,Partin AW.Obesity-related plasma hemodilution and PSA concentration among men with prostate cancer.JAMA 2007;298:2275e80.
[6]Kubota Y,Seike K,Maeda S.Relationship between prostatespecif i c antigen and obesity in prostate cancer screening: analysis of a large cohort in Japan.Int J Urol 2011;18:72e5.
[7]Grubb III RL,Balck A,Izmirlian G.Serum prostate-specif i c antigen hemodilution among obese men undergoing screening in the prostate,lung,colorectal,and ovarian cancer screening trial.Cancer Epidemiol Biomarkers Prev 2009;18:748e51.
[8]Wright JL,Lin DW,Stanford JL.The effect demographic and clinical factors on the relationship between BMI and PSA levels. Prostate 2011;71:1631e7.
[9]D’Amico AV,Whittington R,Malkowicz SB,Schultz D,Blank K, Broderick GA,et al.Biochemical outcome after radical prostatectomy,external beam radiation therapy,or interstitial radiation therapy for clinically localized prostate cancer.JAMA 1998;280:969e74.
[10]Schroder FH,Hugosson J,Roobol MJ,Tammela TL,Ciatto S, Nelen V,et al.Screening and prostate-cancer mortality in a randomized European study.N Engl J Med 2009;360:1320e8.
[11]BaillargeonJ,PollockBH,KristalAR,BradshawP, Hermandez J,Basler J,et al.The association of body mass index and prostate specif i c antigen in a population-based study.Cancer 2005;103:1092e5.
[12]Ekman P.Genetic and environmental factors in prostate cancer genesis:identifying high-risk cohorts.Eur Urol 1999; 35:362e9.
[13]Kanazawa M,Yoshiike N,Osaka T,Numba Y,Zimmet P,Shuji I. Criteria and classif i cation of obesity in Japan and Asia-Oceania.World Rev Nutr Diet 2005;94:1e12.
[14]Stowell L,Sherman I,Hamel K.An enzyme-linked immunosorbent assay[ELISA]for prostate specif i c antigen.Forensic Sci Interm 1991;50:125e38.
[15]Loeb S,Yu X,Nadler RB,Roehl KA,Han M,Hawkins SA,et al. Does body mass index affect preoperative prostate specif i c antigen velocity or pathological outcomes after radical prostatectomy?J Urol 2007;177:102e6.
[16]Culp S,Porter M.The effect of obesity and lower prostatespecif i c antigen levels on prostate cancer screening results in American men.BJU Int 2009;104:1457e61.
[17]BaillargeonJ,PollockBH,KristalAR,BradshawP, Hernandez J,Basler J,et al.The association of body mass index and prostate-specif i c antigen in a population-based study.Cancer 2005;103:1092e5.
[18]Kim YJ,Han BK,Hong SK,Byun SS,Kim WJ,Lee SE.Body mass index inf l uences prostate-specif i c antigen in men younger than 60 years of age.Int J Urol.2007;14:1009e12.
[19]Yang WJ.The likelihood of having a serum PSA level of?2.5 or ?4.0 ng/mL according to obesity in a screened Korean population.Asian J Androl 2013;15:770e2.
[20]Naito M,Asai Y,Mori A,Fukada Y,Kuwabara M,Katase S,et al. Association of obesity and diabetes with serum prostatespecif i c antigen levels in Japanese males.Nagoya J Med Sci 2012;74:285e92.
[21]Banez LL,Hamilton RJ,Partin AW,Vollmer RT,Sun L, Rodriguez C,et al.Obesity-related plasma hemodilution and PSA concentration among men with prostate cancer.JAMA 2007;298:2275e80.
[22]Muller H,Raum E,Rothenbacher D,Stegmaier C,Brenner H. Association of diabetes and body mass index with levels of prostate-specif i cantigen:implicationsforcorrectionof prostate-specif i c antigen cutoff values?Cancer Epidemiol Biomarkers Prev 2009;18:1350e6.
[23]Thompson IM,Leach R,Troyer D,Pollock B,Naylor S,Higgins B. Relationshipofbodymassindexandprostatespecif i cantigenin a population-based study.Urol Oncol 2004;22:127e31.
[24]Kang JS,Maygarden SJ,Mohler JL,Pruthi RS.Comparison of clinical and pathological features in African-American and Caucasian patients with localized prostate cancer.BJU Int 2004;93:1207e10.
Received 12 February 2015;received in revised form 4 May 2015;accepted 10 June 2015 Available online 24 June 2015
*Corresponding author.
E-mail address:patrickikelomo@yahoo.com(P.T.Adegun).
Peer review under responsibility of Shanghai Medical Association and SMMU.
http://dx.doi.org/10.1016/j.ajur.2015.06.004
2214-3882/ª2015 Editorial Off i ce of Asian Journal of Urology.Production and hosting by Elsevier(Singapore)Pte Ltd.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Methods:This was a prospective cross-sectional survey among men who presented with benign prostatic hypertrophy to the urology clinic of the Ekiti State University Teaching Hospital,Ado -Ekiti with LUTS between January 1 and December 31,2014.One hundred and forty men who presented in the urologic clinic with LUTS were recruited.PSA was analyzed using standard method while other clinical variables were collected using a clinical case form.Multivariate logistic regression was used to estimate the odds of an abnormal PSA of?4.0 ng/mL or ?10.0 ng/mL in these men.
Results:The mean ages of obese and non-obese men were 64.8 and 64.0 years respectively. The mean total serum PSA were 14.8 and 13.2 ng/mL for obese and non-obese men respectively.Univariate analysis showed no difference(p>0.05)in the proportion of obese and non-obese men with LUTS who had a PSA threshold of at least 4.0 ng/mL.Multivariate logistic regression showed that,at a PSA threshold of 10.0 ng/mL,obese men had a statistically significant proportion(p<0.05).Although not signif i cant,non-obese patients were less likely to have PSA level of?4.0 ng/mL(OR 0.701;95%CI 0.301e1.630)compared to obese men.In
 Asian Journal of Urology2015年3期
Asian Journal of Urology2015年3期
- Asian Journal of Urology的其它文章
- Evaluation of kidney allograft status using novel ultrasonic technologies
- Pygopus 2 promotes kidney cancer OS-RC-2 cells proliferation and invasion in vitro and in vivo
- Does varicocele grade predict the postoperative changes of semen parameters following left inguinal micro-varicocelectomy?
- Serum cystatin C can be used as a marker of renal function even in patients with intestinal urinary diversion
- Isolated penile urethral injury:A rare case following male coital trauma
- Extensive prostatic calculi in alkaptonuria: An unusual manifestation of rare disease