国内创伤救治中应重视“可预防性死亡”的应用
2015-12-23 09:32江利冰马岳峰
创伤外科杂志 2015年6期
江利冰,马岳峰,张 茂
·综述·
国内创伤救治中应重视“可预防性死亡”的应用
江利冰,马岳峰,张茂
【摘要】随着经济的发展,创伤已经严重威胁到人类的生命安全。在国外,很多研究已经证实实施创伤救治质量提高计划(trauma quality improvement program,TQIP),尤其是创伤可预防性死亡在创伤救治中的应用,可以显著降低创伤患者的死亡率。但是到目前为止,创伤可预防性死亡的概念在国内尚未正式提出。本文就创伤可预防性死亡的概念、流行病学资料以及如何在创伤救治质量提高过程中应用创伤可预防性死亡进行综述。
【关键词】创伤;质量提高计划;可预防性死亡;救治
作者单位:310009浙江 杭州,浙江大学医学院附属第二医院急诊医学科
随着世界经济水平的不断提高,创伤已经成为导致人类死亡的主要病因。在美国,创伤是45岁以下青年人群的首位死亡原因,65岁以下人群的第四位死亡原因。2010年全球死于创伤的人数超过500万,占全球死亡人数的9%,占全球伤残调整寿命年的11%[1]。而且创伤给人类带来的不仅仅是死亡,Trunkey[2]在1982年就提到在创伤事件中,每1例创伤患者的死亡,同时伴随着2例创伤患者永久的瘫痪。流行病学资料预测, 2030年之前,创伤对人类生命健康的影响仍将继续加大,将会造成人类伤残调整寿命年的大量损失,同时显著增加医疗费用和伤残率[3]。因此无论是对于患者个体,还是对于整个社会经济的发展,创伤均将造成巨大的损失[4]。在中国,每年各类伤害发生约2亿人次,是继恶性肿瘤、脑血管病、呼吸系统疾病和心脏疾病第五位死亡原因。每年因伤害死亡人数约70万~75万人,占死亡总人数的9%左右,每年因伤害引起的直接医疗费达650亿元,因伤害休工而产生的经济损失高达60多亿元[5]。
1创伤可预防性死亡的概念
创伤可预防死亡在欧美等发达国家的应用已经相当普遍[6-9],但是在国内尚未有文献对此进行正式报道,导致创伤可预防死亡在国内的创伤救治质量控制和提高过程中没有得到充分的利用。不同的创伤救治中心对创伤死亡的可预防性定义可能不同,但是最常使用的判断标准是根据世界卫生组织(WHO)指南推荐,将创伤死亡划分为3个类型:创伤可预防性死亡、创伤潜在可预防性死亡以及创伤不可预防性死亡。其中创伤可预防性死亡应满足以下条件:(1)创伤本身(解剖损伤)是非致命的;(2)如果采取合理的创伤救治流程,死亡是可以避免的;(3)实际操作过程中偏离了相应的创伤救治规范,直接或间接地引起了创伤患者的死亡。创伤潜在可预防性死亡应满足以下条件:(1)创伤严重程度(解剖损伤)是严重的,但是是非致命的;(2)如果采取合理的创伤救治流程,死亡是潜在可以避免的;(3)对于这类死亡患者,处理往往是合理的, 但是仍然存在一些不同程度的偏离创伤救治规范的环节,而这些偏离规范的环节可能直接或间接与患者的死亡有关。创伤不可预防性死亡应满足:(1)创伤本身(解剖损伤)是致命的,即使创伤救治流程达到最佳状态,也不能改变这类患者的死亡结局;(2)根据公认的创伤救治规范/指南判断,这类创伤患者的处理流程是合理规范的;(3)这类患者可能伴发一些共患病或基础疾病,与创伤叠加,导致这类患者发生不可逆转的死亡[10]。
2创伤可预防性死亡的发生率
不同的创伤救治中心对创伤预防性死亡的发生率报道不一,作者认为至少两方面原因可以解释创伤可预防性死亡在不同的创伤救治中心发生率不一致的现象。(1)不同创伤救治中心的创伤救治水平不一。已有研究指出创伤患者的预后与该救治中心的创伤患者数量、是否为大学附属医院等因素有关[11-13]。因此美国外科医师学会规定Ⅰ级创伤中心每年至少应救治1200例不同损伤程度的创伤患者,其中严重创伤患者[损伤严重度评分(ISS)>15分]应在240例以上[14]。(2)不同创伤救治中心对创伤死亡类型的判断使用的标准不同。主要包括两种途径:①通过组建多学科创伤审核团队,对创伤死亡的可预防性进行评判,其中使用最多的就是WHO推荐的判定标准,上文对此已经进行了详细的描述[10];②通过各种创伤评分系统,对创伤患者的死亡风险进行划分,最常用的为TRISS法(revised trauma score and injury severity score)。根据TRISS方法可以计算出创伤患者的生存概率(P),从而对创伤死亡的可预防性进行评判。创伤可预防性死亡:P>0.5,患者死亡;创伤潜在可预防性死亡:0.25 3创伤可预防性死亡在创伤救治质量控制与提高中的应用 损伤严重程度相似的创伤患者在创伤救治能力相似的不同的创伤救治中心进行救治,预后却可能不一样,这在一定程度上是因为不同创伤救治中心实施创伤救治质量控制与提高的力度不同[12]。而有研究指出在创伤救治过程中,实施创伤救治质量提高计划可以显著降低创伤患者的死亡率[24,33]。一项横断面研究调查了加拿大魁北克59家创伤专科医院,发现在创伤救治过程中实施创伤救治质量提高计划是预测创伤患者生存率最强的影响因素。最近,Wong和Dinh等[34-35]也指出在引入创伤救治质量提高计划之后的10年内,创伤患者的粗死亡率下降了3%。创伤可预防性死亡不仅是衡量创伤救治水平的指标,同时也是整个创伤救治流程和创伤救治体系的评估工具。国外已有研究通过多学科创伤审核小组对每一例创伤可预防性死亡患者的整个救治流程,包括院前、院内进行回顾性分析,寻找救治过程中的诊疗失误,并对此提出改进的措施,从而提高创伤患者的救治水平。Teixeira等[9]对美国南加州大学医学中心(Ⅰ级创伤中心)1998年1月~2005年12月连续8年的创伤死亡患者进行回顾性分析,发现导致创伤可预防性死亡(包括可预防性和潜在可预防性死亡)最常见的原因是出血(39.2%)、多器官功能不全(27.5%)以及心跳呼吸骤停(15.6%)。国外已有不少研究证实对创伤死亡原因的分析可以提高创伤患者的救治质量[6]。导致创伤可预防性死亡最常见的失误是治疗延迟(52.9%)、临床判断失误 (21.6%)、诊断遗漏(11.8%)以及技术失误(7.8%)。而且作者还指出导致创伤可预防性死亡的失误主要发生在创伤救治的早期,其中41.2% 的失误发生在复苏阶段[9]。以上事实说明对创伤可预防性死亡的研究可以识别创伤救治流程中的缺陷,从而启动相应的应对和改进措施,最终改善创伤患者的预后。典型的例子就是在美国奥兰治县曾经因为无规范和流程的救治导致创伤可预防性死亡的发生率很高,这一现象最终导致了奥兰治县对整个创伤救治系统进行改进和提高,包括院前组织救治、现场分流标准的实施以及对院内创伤救治能力的提高等。而这些改进和提高措施使得创伤可预防性死亡的发生率从34%下降至15%[19]。类似的结果也在美国蒙大拿州进行了报道,通过对可预防性死亡的回顾性分析,不断地改进创伤救治流程,在5年内,该地区的创伤可预防性死亡从13%下降至8%[36]。 以上分析均需要所有的创伤救治单位具有相应的创伤审核指标(如院前时间、入急诊室至首次头颅CT的时间、受伤至手术的时间等)以及相应的创伤救治规范和指南,以便将创伤可预防性死亡患者的创伤救治流程与其进行比对,从而发现该类患者救治流程中的不足之处。笔者建议可以参考WHO推荐的创伤救治核查单、美国外科协会(ACS)制定的创伤救治审核指标、东部创伤外科学会以及西部创伤协会制定的各种创伤救治规范和指南,结合本地区的实际情况制定最适合本地区的创伤救治流程以及审核指标。而整个创伤救治质量的提高过程需要反复循环实践,因此需要良好的监测系统即创伤数据库,只有具备了良好的创伤登记制度,才能将整个创伤救治质量的提高过程形成一个闭合的环路,不断地提高创伤患者的救治质量(图1)。 图1 创伤审核 我国作为世界人口最多、交通事故和意外伤害高发的国家,创伤救治水平与国外发达国家还存在很大的差距,尤其是在创伤救治质量控制和提高方面。笔者在此强调了创伤性可预防性死亡的重要性,以期可以为我国的创伤救治质量控制和提高增砖添瓦。 参考文献: [1]Ozano R,Naghavi M,Foreman K,et al.Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010:a systematic analysis for the Global Burden of Disease Study 2010[J].Lancet, 2012,380(9859):2095-2128. [2]Trunkey DD.On the nature of things that go bang in the night[J].Surgery,1982,92(2):123-132. [3]Mathers CD,Loncar D.Projections of global mortality and burden of disease from 2002 to 2030[J].PLoS Med,2006,3(11):e442. [4]Jayaraman S,Sethi D.Advanced trauma life support training for hospital staff[J].Cochrane Database Syst Rev,2009,15(2):CD004173. [5]徐少文,赵小纲,张茂.严重创伤救治若干新进展[J].中华急诊医学杂志,2011,20(5):456-458. [6]Tien HC,Spencer F,Tremblay LN,et al.Preventable deaths from hemorrhage at a level I Canadian trauma center[J].J Trauma Acute Care Surg,2007,62(1):142-146. [7]Kleber C,Giesecke MT,Lindner T,et al.Requirement for a structured algorithm in cardiac arrest following major trauma: epidemiology, management errors, and preventability of traumatic deaths in Berlin[J].Resuscitation,2014,85(3):405-410. [8]Saltzherr TP,Wendt KW,Nieboer P,et al.Preventability of trauma deaths in a Dutch Level-1 trauma centre[J].Injury,2011,42(9):870-873. [9]Teixeira PG,Inaba K,Hadjizacharia P,et al.Preventable or potentially preventable mortality at a mature trauma center[J].J Trauma Acute Care Surg,2007,63(6):1338-1347. [10]Mock C,Juillard C,Brundage S,et al.Guidelines for trauma quality improvement programmes.World Health Organization,2009. [11]Caputo LM,Salottolo KM,Slone DS,et al.The relationship between patient volume and mortality in American trauma centres: a systematic review of the evidence[J].Injury,2014,45(3):478-486. [12]Chaubey VP,Roberts DJ,Ferri MB,et al.Quality improvement practices used by teaching versus non-teaching trauma centres: analysis of a multinational survey of adult trauma centres in the United States,Canada,Australia,and New Zealand[J].BMC Surg,2014,14(1):112. [13]Todd SR,Arthur M,Newgard C,et al.Hospital factors associated with splenectomy for splenic injury: a national perspective[J].J Trauma Acute Care Surg,2004,57(5):1065-1071. [14]Minei JP,Fabian TC,Guffey DM,et al.Increased trauma center volume is associated with improved survival after severe injury: results of a resuscitation outcomes consortium study[J].Ann Surg,2014,260(3):456-465. [15]Moon JH,Seo BR,Jang JW,et al.Evaluation of probability of survival using trauma and injury severity score method in severe neurotrauma patients[J].J Korean Neurosurg Soc,2013,54(1):42-46. [16]MacKenzie EJ,Steinwachs DM,Bone LR,et al.Inter-rater reliability of preventable death judgments[J].J Trauma Acute Care Surg,1992,33(2):292-303. [17]Wilson DS,McElligott J,Fielding LP.Identification of preventable trauma deaths: confounded inquiries[J].J Trauma Acute Care Surg,1992,32(1):45-51. [18]Goldman RL.The reliability of peer assessments a meta-analysis[J].Eval Health Prof,1994,17(1):3-21. [19]Cales RH.Trauma mortality in Orange County: the effect of implementation of a regional trauma system[J].Ann Emerg Med,1984,13(1):1-10. [20]Esposito TJ,Sanddal TL,Reynolds SA,et al.Effect of a voluntary trauma system on preventable death and inappropriate care in a rural state[J].J Trauma Acute Care Surg,2003,54(4):663-670. [21]Cales RH,Trunkey DD.Preventable trauma deaths: a review of trauma care systems development[J].JAMA,1985,254(8):1059-1063. [22]Chiara O,Scott JD,Cimbanassi S,et al.Trauma deaths in an Italian urban area: an audit of pre-hospital and in-hospital trauma care[J].Injury,2002,33(7):553-562. [23]Esposito TJ,Sanddal ND,Dean JM,et al.Analysis of preventable pediatric trauma deaths and inappropriate trauma care in Montana[J].J Trauma Acute Care Surg,1999,47(2):243-253. [24]Yeboah D,Mock C,Karikari P,et al.Minimizing preventable trauma deaths in a limited-resource setting: a test-case of a multidisciplinary panel review approach at the Komfo Anokye Teaching Hospital in Ghana[J]. World J Surg,2014,38(7):1707-1712. [25]Maio RF,Burney RE,Gregor MA,et al.A study of preventable trauma mortality in rural Michigan[J].J Trauma Acute Care Surg,1996,41(1):83-90. [26]Saltzherr TP,Wendt KW,Nieboer P,et al.Preventability of trauma deaths in a Dutch Level-1 trauma centre[J].Injury,2011,42(9): 870-873. [27]Sanddal TL,Esposito TJ,Whitney JR,et al.Analysis of preventable trauma deaths and opportunities for trauma care improvement in Utah[J].J Trauma Acute Care Surg,2011,70(4):970-977. [28]West JG,Cales RH,Gazzaniga AB.Impact of regionalization: the Orange County experience[J].Arch Surg,1983,118(6):740-744. [29]Zafarghandi MR,Modaghegh MHS,Roudsari BS.Preventable trauma death in Tehran: an estimate of trauma care quality in teaching hospitals[J].J Trauma Acute Care Surg,2003,55(3):459-465. [30]Afuwape OO,Okolo CA,Akinyemi OA.Preventable trauma deaths in Ibadan: a comparison of revised trauma score and panel review[J].West Afr J Med,2011,30(1):19-23. [31]Jat AA,Khan MR,Zafar H,et al.Peer review audit of trauma deaths in a developing country[J].Asian J Surg,2004,27(1): 58-64. [32]Navarro S, Montmany S, Rebasa P, et al. Impact of ATLS training on preventable and potentially preventable deaths[J].World J Surg,2014,38(9):2273-2278. [33]Juillard CJ,Mock C,Goosen J,et al.Establishing the evidence base for trauma quality improvement: a collaborative WHO-IATSIC review[J].World J Surg,2009,33(5):1075-1086. [34]Wong TH,Lumsdaine W,Hardy BM,et al.The impact of specialist trauma service on major trauma mortality[J].J Trauma Acute Care Surg,2013,74(3):780-784. [35]Dinh MM,Bein KJ,Gabbe BJ,et al.A trauma quality improvement programme associated with improved patient outcomes: 21 years of experience at an Australian Major Trauma Centre[J].Injury,2014,45(5):830-834. [36]Esposito TJ,Sanddal TL,Reynolds SA,et al. Effect of a voluntary trauma system on preventable death and inappropriate care in a rural state[J].J Trauma Acute Care Surg,2003,54(4):663-670. (本文编辑:黄小英) Trauma care in China should attach importance to the application of preventable death JIANGLi-bing,MAYue-feng,ZHANGMao (Department of Emergency,Second Affiliated Hospital,School of Medicine,Zhejiang University, Hangzhou310009,China) 【Abstract】With the development of economy,trauma has seriously threatened peoples’ health and lives.A lot of researches in foreign counties has reported that a trauma quality improvement program(TQIP),particularly the application of preventable trauma death,is associated with lower mortality of trauma patients.Up to now,however,the definition of preventable trauma death in China has not been put forward formally.In this paper,we reviewed the definition and epidemiology of preventable trauma death and discussed how to apply preventable trauma death in the trauma quality improvement protocol. 【Key words】trauma;quality improvement;preventable death (收稿日期:2015-02-26;修回日期:2015-04-14) 【中图分类号】R 641 【文献标识码】A【DOI】10.3969/j.issn.1009-4237.2015.06.033 文章编号:1009-4237(2015)06-0570-04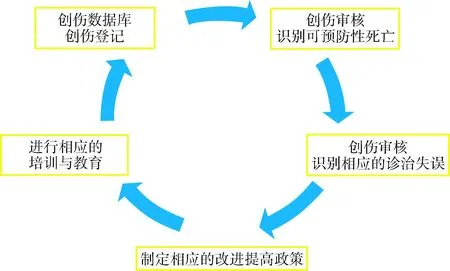
猜你喜欢
中国医学创新(2016年34期)2017-02-28
中外医学研究(2017年1期)2017-02-23
中国医药科学(2016年10期)2017-02-05
现代养生·下半月(2016年5期)2017-01-09
电子技术与软件工程(2016年20期)2016-12-21
上海医药(2016年22期)2016-12-13
北方文学·中旬(2016年9期)2016-12-08
戏剧之家(2016年22期)2016-11-30
中外医学研究(2016年28期)2016-11-28