
替格瑞洛用于老年急性ST段抬高型心肌梗死急诊PCI治疗患者的临床研究
2016-04-21 03:01郭金成朱芙丽蔡宜婷陈文明柳子静郝明辉
中华老年多器官疾病杂志 2016年10期
郭金成,朱芙丽,蔡宜婷,陈文明,柳子静,郝明辉
(首都医科大学附属北京潞河医院心血管内科,北京 101149)
急性ST段抬高型心肌梗死(ST segment elevation myocardial infarction,STEMI)患者急诊经皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)术前、术后给予双联抗血小板治疗(dual anti-platelet therapy,DAPT)已经成为标准治疗。新的P2Y12(血小板ADP受体)受体拮抗剂替格瑞洛(ticagrelor)是2014年和2015年欧洲心脏病学会(European Society of Cardiology,ESC)和美国心脏病学学会(American College of Cardiology,ACC)、美国心脏协会(American Heart Association,AHA)指南推荐急诊PCI 优先选用的抗血小板药物[1-3],但替格瑞洛在我国患者中的使用处于起步阶段,用于老年STEMI急诊PCI患者的临床经验不足。本研究旨在评估替格瑞洛在老年STEMI急诊PCI患者中应用的临床疗效。
1 对象与方法
1.1 研究对象
连续入选2012年11月至2014年12月北京潞河医院心血管内科急性STEMI接受急诊PCI手术患者240例,其中男性147例,女性93例,年龄60~91(71.93±6.87)岁。入选标准:(1)符合STEMI的诊断标准[4];(2)年龄≥60岁,发病时间≤12 h;(3)签署PCI知情同意书。排除标准:(1)心源性休克;(2)既往出血性脑卒中或中重度肝病;(3)大出血活动期;(4)替格瑞洛或氯吡格雷过敏;(5)6个月内有重大手术或外伤、脑血管疾病;(6)凝血疾病和血小板减少症。
1.2 方法
根据应用P2Y12受体拮抗剂不同,分为替格瑞洛组和氯吡格雷(clopidogrel)组,所有患者术前均嚼服阿司匹林300 mg,维持量每天100 mg。替格瑞洛组(倍林达,阿斯利康制药有限公司),术前顿服180 mg,术后90 mg,2次/d,服用至少1 年;氯吡格雷组(波立维,赛诺菲制药公司)术前顿服600 mg,术后75 mg,1次/d,服用至少1 年。使用更换药物前需接受负荷剂量(如替格瑞洛更换为氯吡格雷,需服用300 mg的氯吡格雷)。
两组患者术前给予肝素100 U/kg,静脉注射,如给予血小板糖蛋白(glycoprotein,GP) Ⅱb/Ⅲa受体拮抗剂,剂量为50~70 U/kg。PCI按标准方法进行。
1.3 观察指标
PCI手术前后心肌梗死溶栓治疗(thrombolysis in myocardial infarction,TIMI)血流分级以及术后心电图ST段回落(ST segment resolution,STR)情况。ST段抬高回落分为完全回落(STR >70%)、部分回落(STR 31%~69%)、无回落(STR≤30%)。主要心脏不良事件(major adverse cardiac events,MACE)包括死亡、脑卒中、再次心肌梗死、靶血管再次血运重建、支架内血栓形成。出血分级采用出血学术研究联合会(bleeding academic research consortium,BARC)定义[5]:1级为无需治疗的非活动性出血;2级为需要处理的活动性出血,但不满足3~5级出血标准;3a级为血红蛋白降低3~5 g/dl且需要输血的出血;3b级为血红蛋白降低≥5 g/dl,或心包压塞,或需要外科止血,或需要使用血管活性药物辅助治疗的出血;3c级为脑出血或眼底出血;4级为与冠状动脉旁路移植术(coronary artery bypass graft,CABG)相关的出血;5级为致死性出血。替格瑞洛或氯吡格雷相关的呼吸困难[6]。需置入永久起搏器的缓慢心律失常。记录随访12个月时停用替格瑞洛/氯吡格雷的时间、原因以及换药情况。
1.4 统计学处理

2 结 果
2.1 两组患者基线资料、冠状动脉造影和介入特点
两组患者基线资料差异无统计学意义(P>0.05;表1)。两组患者操作通路从桡动脉更换到股动脉的比例、术前TIMI血流分级、梗死相关动脉、置入支架、主动脉内气囊反搏、GPⅡb/Ⅲa受体拮抗剂及造影剂使用等方面差异无统计学意义(P>0.05),替格瑞洛组介入术后TIMI 3级血流患者比例明显高于氯吡格雷组(91.5%vs80.8%,P=0.024;表2)。

表1 两组间基线资料的比较
SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; LVEF: left ventricular ejection fraction; CK: creatine kinase; ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin receptor blocker.1 mmHg=0.133 kPa

表2 两组患者造影和介入特点比较
LAD: left anterior descending artery; LCX: left circumflex; RCA: right coronary artery; PCI: percutaneous coronary intervention; IABP: intra-aortic balloon pump; GPⅡb/Ⅲa: glycoprotein Ⅱb/Ⅲa; STR: ST segment resolution
2.2 两组患者出血并发症和不良反应
两组患者BARC 1~3级出血发生率分别为28.7%和24.0%,差异无统计学意义(P>0.05)。BARC 3型出血患者4例均发生在住院期间,术前、术后均应用低分子肝素。替格瑞洛组消化道出血患者2例,BARC 3a出血患者1例,女性,75岁,有尿毒症病史,住院期间死亡。BARC 3b出血患者1例,男性,82岁,肾功能不全4期,术后3天黑便,经处理好转出院。氯吡格雷组BARC 3a出血患者1例,男性,77岁,消化道出血经治疗好转。BARC 3c型出血患者1例,女性,66岁,既往高血压,3年前脑梗死并有后遗症,急诊处理前降支,第7天择期处理右冠状动脉时出现无复流,应用GPⅡb/Ⅲa受体拮抗剂并置入主动脉球囊反搏(intra-aortic balloon pump,IABP),第2天脑出血后死亡。两组患者呼吸困难差异无统计学意义(12.8%vs6.8%,P=0.121)。两组患者均无药物相关心动过缓而需置入起搏器。
2.3 两组患者坚持服药情况及停换药原因
替格瑞洛组院内停药患者1例(1.1%),该患者服用后2 h即出现严重的呼吸困难,因此停药,换用氯吡格雷。出院时、出院后30 d、6个月和12个月内坚持服药情况见表3,两组患者坚持服药方面差异有统计学意义(P<0.001)。相比氯吡格雷组,替格瑞洛组12个月内易停药或更改抗栓方案,差异有统计学意义(P<0.001),主要原因是医师更改抗栓方案、经济原因和呼吸困难。具体停药原因见表4。替格瑞洛组患者12个月内坚持双联抗血小板治疗(dual anti-platelet therapy,DAPT)者占85.1%(80/94),氯吡格雷组占88.4%(129/146),两组差异无统计学意义(P>0.05)。

表3 两组患者坚持服药情况
2.4 院内、术后12个月MACE
两组患者院内和术后12个月MACE发生率相似,差异无统计学意义(5.3%vs5.5%,8.5%vs8.9%,P>0.05;表5)。
表412个月内停换药原因
Table 4 Reasons for drug withdrawal or discontinuation within 12 months [n(%)]
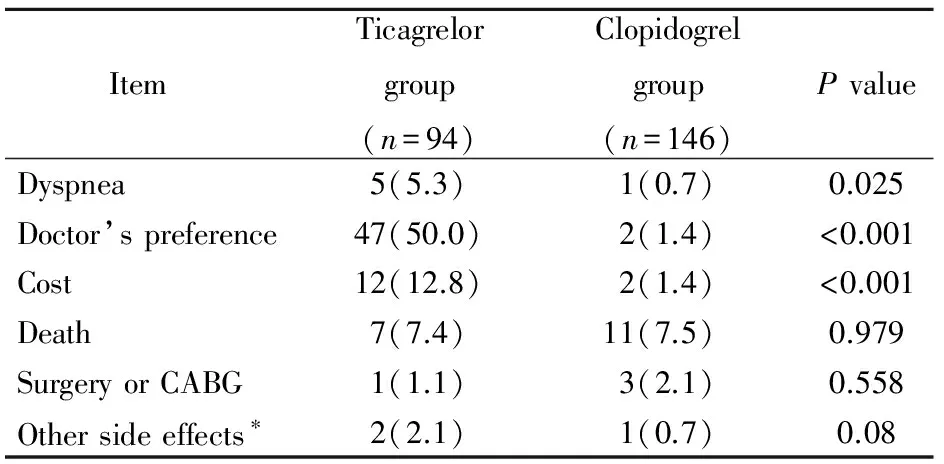
Item Ticagrelorgroup(n=94)Clopidogrelgroup(n=146)PvalueDyspnea5(5.3)1(0.7)0.025Doctor’spreference47(50.0)2(1.4)<0.001Cost12(12.8)2(1.4)<0.001Death7(7.4)11(7.5) 0.979SurgeryorCABG1(1.1)3(2.1)0.558Othersideeffects∗2(2.1)1(0.7)0.08
*other side effects include high serum uric acid level in ticagrelor group and allergic to clopidogrel in clopidogrel group. CABG: coronary artery bypass grafting
表5院内及出院后12个月MACE
Table 5 MACE during hospital staying and 12-month’s follow-up [n(%)]
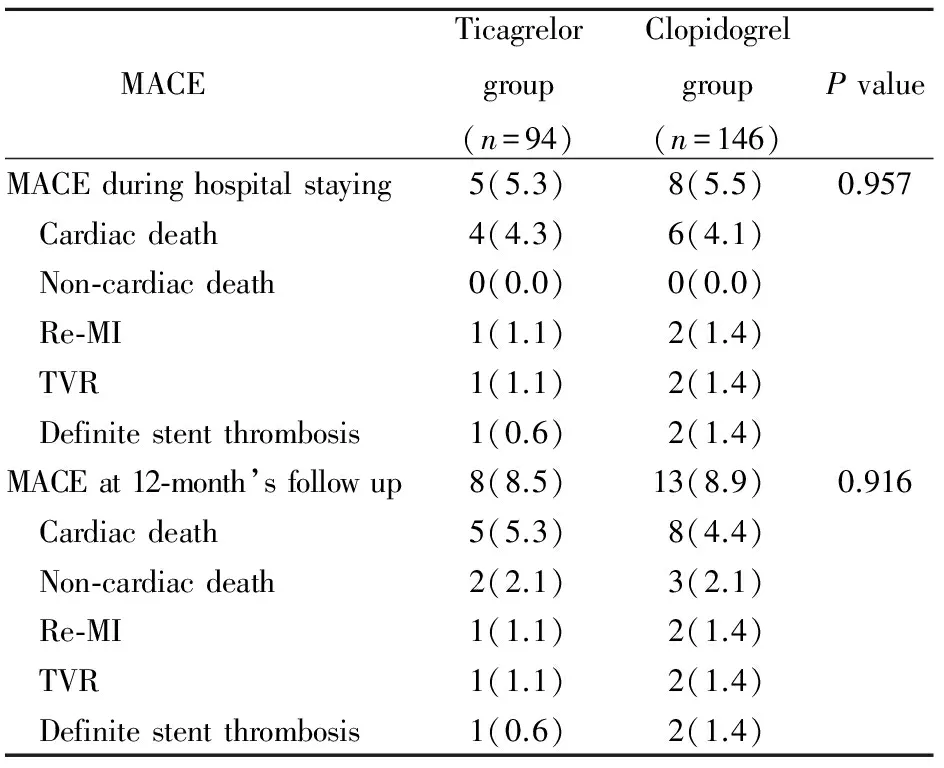
MACE Ticagrelorgroup(n=94)Clopidogrelgroup(n=146)PvalueMACEduringhospitalstaying5(5.3)8(5.5)0.957 Cardiacdeath4(4.3)6(4.1) Non⁃cardiacdeath0(0.0)0(0.0) Re⁃MI1(1.1)2(1.4) TVR1(1.1)2(1.4) Definitestentthrombosis1(0.6)2(1.4)MACEat12⁃month’sfollowup8(8.5)13(8.9)0.916 Cardiacdeath5(5.3)8(4.4) Non⁃cardiacdeath2(2.1)3(2.1) Re⁃MI1(1.1)2(1.4) TVR1(1.1)2(1.4) Definitestentthrombosis1(0.6)2(1.4)
MACE: major adverse cardiac events; Re-MI: recurrent myocardial infarction; TVR: target vessel revascularization
3 讨 论
本研究发现,与氯吡格雷相比,替格瑞洛用于老年STEMI患者急诊PCI治疗能改善术后TIMI 3级血流且不增加出血,是有效和安全的。两组院内和12个月MACE发生率相似,临床替格瑞洛停换药常见,原因多见医师更改抗栓方案、经济原因和呼吸困难。
老年STEMI患者急诊PCI治疗能够明显改善预后,但成功率低、出血发生率高[7]。与氯吡格雷相比,新一代本身具有活性的P2Y12受体拮抗剂替格瑞洛能明显降低患者的血管性死亡、心肌梗死和卒中的发生,同时并不增加主要出血的发生且获得指南推荐用于急性冠脉综合征患者[8-10]。但替格瑞洛在国内应用时间短,尤其在老年急诊PCI患者中应用经验不足。本研究中发现替格瑞洛组术后TIMI 3级血流比例高于氯吡格雷组,其原因是替格瑞洛抗血小板作用强,通过抑制红细胞对腺苷的摄取增加血浆腺苷浓度,从而发挥腺苷介导的冠状动脉血流增加,抑制血小板聚集[11,12]。
虽然替格瑞洛在疗效方面优势明显,但老年人因常合并其他系统疾病,器官储备功能差,出血发生率高,应引起临床重视[13,14]。本研究中两组总的BARC出血分型发生率分别为28.7%和24.0%(P>0.05)。BARC 3型出血发生率两组差异无统计学意义(2.2%vs1.8%,P=0.654),替格瑞洛组消化道出血2例均有肾功能不全病史。氯吡格雷组脑出血死亡1例患者与GP Ⅱb/Ⅲa受体拮抗剂的应用、置入IABP有关。本研究严重出血发生率均低于PLATO心肌梗死亚组报道的替格瑞洛4.1%和氯吡格雷3.8%的非搭桥相关的严重出血发生率[15],可能与本组研究病例数少有关。
本研究分析了老年STEMI患者PCI出院时、术后1个月、3个月、6个月和12个月内停服替格瑞洛的原因。结果发现替格瑞洛停换药常见原因是医师更改抗栓方案、经济原因和呼吸困难,与国内报道基本一致[6]。提高心血管医师对替格瑞洛的理解有助于减少抗栓方案的更改。
除急诊PCI即刻的效果外,术后心肌梗死复发和支架血栓形成也是影响远期预后的重要因素。本研究两组死亡率、支架内血栓形成等无差异可能与回顾性研究样本量小、采用ITT分析方法使替格瑞洛降低MACE的作用被换成氯吡格雷所稀释等有关。
随着替格瑞洛在老年STEMI患者中应用经验的积累,将有更多的老年STEMI患者从中获益。但也需要大样本随机对照试验进一步证实。
【参考文献】
[1] Windecker S, Kolh P, Alfonso F,etal. 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI)[J]. Eur Heart J, 2014, 35(37): 2541-2619.
[2] Roffi M, Patrono C, Collet JP,etal. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2016, 37(3): 267-315.
[3] Levine GN, Bates ER, Blankenship JC,etal. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction[J]. J Am Coll Cardiol, 2016, 67(10): 1235-1250.
[4] Society of Cardiovascular Diseases of Chinese Medical Association, Editor Committee of Chinese Journal of Cardiology. Guidelines on the diagnosis and therapy of ST-segment elevation myocardial infarction[J]. Chin J Cardiol, 2015, 43(5): 380-393.[中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 急性ST段抬高型心肌梗死诊断和治疗指南[J]. 中华心血管病杂志, 2015, 43(5): 380-393.]
[5] Mehran R, Rao SV, Bhatt DL,etal. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium[J]. Circulation, 2011, 123(23): 2736-2747.
[6] Wang XY, Xi SZ, Liu J,etal. The reasons and impact of ticagrelor withdrawal in patients with coronary artery disease[J]. Chin J Mult Organ Dis Elderly, 2016, 15(3): 231-236.[王绪云, 席少枝, 刘 佳, 等. 冠心病患者替格瑞洛停药原因及停药对临床转归的影响分析[J]. 中华老年多器官疾病杂志, 2016, 15(3): 231-236.]
[7] Fach A, Bünger S, Zabrocki R,etal. Comparison of outcomes of patients with ST-segment elevation myocardial infarction treated by primary percutaneous coronary intervention analyzed by age groups (<75, 75 to 85, and >85 years); (results from the Bremen STEMI registry)[J]. Am J Cardiol, 2015, 116(12): 1802-1809.
[8] Wallentin L, Becker RC, Budaj A,etal. Ticagrelorversusclopidogrel in patients with acute coronary syndromes[J]. N Engl J Med, 2009, 361(11): 1045-1057.
[9] O’Gara PT, Kushner FG, Ascheim DD,etal. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines[J]. J Am Coll Cardiol, 2013, 61(4): e78-140.
[10] Wang H, Wang X. Efficacy and safety outcomes of ticagrelor compared with clopidogrel in elderly Chinese patients with acute coronary syndrome[J]. Ther Clin Risk Mana, 2016, 12: 1101-1105.
[11] Bonello L, Laine M, Kipson N,etal. Ticagrelor increases adenosine plasma concentration in patients with an acute coronary syndrome[J]. J Am Coll Cardiol, 2014, 63(9): 872-877.
[12] Nylander S, Femia EA, Scavone M,etal. Ticagrelor inhibits human platelet aggregationviaadenosine in addition to P2Y12 antagonism[J]. J Thromb Haemost, 2013, 11(10): 1867-1876.
[13] Singh M. Bleeding avoidance strategies during percutaneous coronary interventions[J]. J Am Coll Cardiol, 2015, 65(20): 2225-2238.
[14] Storey RF, Angiolillo DJ, Patil SB,etal. Inhibitory effects of ticagrelor compared with clopidogrel on platelet function in patients with acute coronary syndromes: the PLATO (platelet inhibition and patient outcomes) PLATELET substudy[J]. J Am Coll Cardiol, 2010, 56(18): 1456-1462.
[15] Steg PG, James S, Harrington RA,etal. Ticagrelorversusclopidogrel in patients with ST-elevation acute coronary syndromes intended for reperfusion with primary percutaneous coronary intervention: A platelet inhibition and patient outcomes (PLATO) trial subgroup analysis[J]. Circulation, 2010, 122(21): 2131-2141.
猜你喜欢
中国典型病例大全(2022年16期)2022-06-10
健康体检与管理(2022年4期)2022-05-13
中国典型病例大全(2022年10期)2022-05-10
现代临床医学(2021年1期)2021-01-26
中华养生保健(2020年9期)2021-01-18
中国药学药品知识仓库(2021年15期)2021-01-14
中西医结合心血管病杂志(电子版)(2020年9期)2020-12-09
中华养生保健(2020年7期)2020-11-16
河南医学研究(2020年22期)2020-09-03
保健与生活(2019年21期)2019-11-25
