
Repetitive transcranial magnetic stimulation combined with venlafaxine and lorazepam for treatment of generalized anxiety
2016-12-09 07:45HuiLingWUMaoRongHUBinYUQiaoShengLIUHuiFangWANG
上海精神医学 2016年4期
HuiLing WU, MaoRong HU*, Bin YU, QiaoSheng LIU, HuiFang WANG
·Original research article·
Repetitive transcranial magnetic stimulation combined with venlafaxine and lorazepam for treatment of generalized anxiety
HuiLing WU, MaoRong HU*, Bin YU, QiaoSheng LIU, HuiFang WANG
generalized anxiety; venlafaxine; transcranial magnetic stimulation; test anxiety scale; China
1. Background
Generalized anxiety disorder (GAD) is one of the common disorders in psychiatric practice. Despite various methods in treatment of GAD - drugs,psychotherapy such as cognitive-behaviour therapy and others - have reached extensive consensus in their efficacy, there are still about 25% GAD patients unresponsive to them. However, a numbers of new methods are constantly emerging with the progressing of neurophysiological research for GAD. Repetitive transcranial magnetic stimulation (rTMS) is an emerging,non-invasive technology of physic therapy, which based on the Faraday’s law of electromagnetic induction,suggesting that electromagnetic field is able to influence the electrical activity of brain tissue, resulting in the depolarization of neurons. This technology is broadly using in treatment of schizophrenia, major depression disorder, generalized anxiety disorder, obsessivecompulsive disorder as well as other types of mental disorders, obtaining satisfied effect.
Yet there is still no conclusion the exactly effect of rTMS in treatment of GAD. A study on animal models found that rTMS has a significant anti-depressive rather than its anxiolytic efficacy, while other researches suggesting that rTMS with significant efficacy of both anti-depressive and anxiolytic. This study discusses the clinical efficacy and safety of the combination of rTMS and venlafaxine in management of GAD, as a part of evaluation of rTMS-drug combined therapy in mental disorders.
2. Objectives and Methods
2.1 Objectives
Ninety-eight patients, including 60 outpatients and 38 inpatients, with a diagnosis of generalized anxiety disorder in JiangXi Mental Health Centre from October 2013 to January 2015, have been recruited. All participants provided written informed consent, which approved by the ethics committee of Jiangxi Mental Health Centre. Inclusion criteria were as follows (a)meet the GAD criteria in ICD-10 diagnostic system;(b) the total score of Hamilton Anxiety Scale (HAMA)greater than 14 and Clinical Global Impression severity(CGI-SI) greater than 3; (c) 20 to 50 years of age, males,received at least middle school education; (d) provided and signed the informed consent; (e) on brain organic diseases, severe physical diseases, drug or alcohol allergy and dependence, anxiety secondary to other disease;(f) no other mental disorders. 28 patients quit at the beginning of observation before performing any kinds of drug treatment, and other 70 patients were meet the criteria and randomized into the research, 34 patients were into the group of rTMS-drug combined therapy, and 36 patients into the group of only drug treatment.
2.2 Methods
2.2.1 Interventions
This study is a randomized paralleled controlled.Considering the efficacy of venlafaxine against anxiety is probably quite different according to the dosages, in this research, we used single initial dose of venlafaxine, 75mg per day, in order to reduce the difficulty of explanation in difference curative effects prompt by unparalleled using unbalanced drug dosages.Specific interventions involve: both two groups were given orally Venlafaxine Hydrochloride Sustainedrelease Tablets (EFEXOR XR, Pfizer) 75mg per day, and lorazepam 1.0 mg orally twice per day, in the morning and night. For the rTMS combined group, the magnetic field therapeutic apparatus (type YRDCCY-I, Wuhan Yiruide Medical Equipment CO., LTD.) were provided to stimulate the dorsolateral right frontal cortex (DLRFC),a treatment area, according to the previous studies,by setting parameters of frequency to 1 Hz, intensity(also motion threshold) to 90% MT, stimulation time to 10s at a 5 second intervals, 20 min a day, 5 days a week, and totally 4 weeks, continuously. The drugonly group was given the fake rTMS, which were same setting as combined group use, excluded the probe of apparatus was always perpendicular to the patient’s skull plane that magnetic signal were unable to via the bone and effect the brain. Other kinds of antipsychotics,antidepressants, anxiolytics and mood stabilizers were inhibited to use during observation (See the Figure 1).
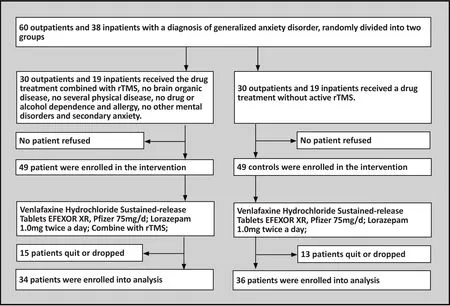
Figure 1. Flow chart of the study
2.2.2 Assessment of Efficacy
The clinical efficacy was assessed using the HAMA scale and side effects were assessed using TESS, both in following time points: before the intervention, in the end of 2ndweek, 4thweek and 6thweek. The severity of disorders evaluated using CGI-SI at the beginning and ending of the treatment period. Also the complete blood cell count, urinalysis, liver and kidney functions test and ECG were performed at same time points. The HAMA reduction rate was used to assess the efficacy at the sixth weekend as following: (a) clinical recovery,HAMA≥75%; (b) significant progress, HAMA 50% to 74%; (c) progress, 25% to 74%; (d) no effect, 0% to 24%.The assessment of CGI-SI scales were by a professional trained psychiatric practitioner on the single blind situation, in contemplation of avoiding the individual differences prompted by multiple evaluators.
2.2.3 Statistic method
Study data were analysed using SPSS (Version 22).Multiple times points within group were compared using repeated measurement of sequence variance analysis and linear regression. General clinical features of both two groups were analysed using paired t test.p<0.05 was considered statistically significant.
3. Results
3.1 Clinical features
Table 1 shows that no significant difference in clinical features in both groups.
3.2 Clinical efficacy
After 6-week treatment, 12 patients in the rTMS-drug combined group were considered as clinical recovery and 22 patients as significant progress, total effective rate 70.6%. In the drug-only group, 27 patients achieved the standard of clinical recovery and 9 cases got progress, with 54.71% total effective rate. The total effective rate of the combined group is significantly higher than the control group.
3.3 HAMA and CGI-SI scores
The HAMA and CGI-SI score of groups before and after treatment period were shown in Table 2 and Figure 2. Table 2 shows the HAMA and CGI-SI score after treatment were significantly lower than before.The comparison of HAMA score within the rTMS-drug combined group were t=34.48, p<0.0001 and CGI-SI,t=12.83, p<0.001; and the HAMA comparison within the only drug group were t=25.03, p<0.0001, and CGI-SI,t=20.63, p<0.001. These results shows that the HAMA score of rTMS-drug combined group is significantly lower than only drug group (F(1,68)=2124.578, p<0.001);meanwhile, the reducing rate increased with a prolonged treatment timeline (Fig. 1, linear regression).At the end of sixth week, both HAMA and CGI-SI score of rTMS-drug combined group are lower than single drug group with significance.
3.4 Adverse reactions
Analysed TESS shows that adverse reactions in both groups appeared more in the early stage of the treatment, mild and with no statistic difference between and within groups. No exception found by the complete blood cell count, urinalysis, liver functions test and ECG of patients.
3.5 Statistical analysis
The HAMA scores before and after treatment were examined using repeated measurement of sequence variance analysis and linear regression; the general information of groups and CGI-SI assessment before and after treatment of them were analysed using paired t test, the significance was p<0.05 in all these aspectsScale Group Before treatment Statistic value
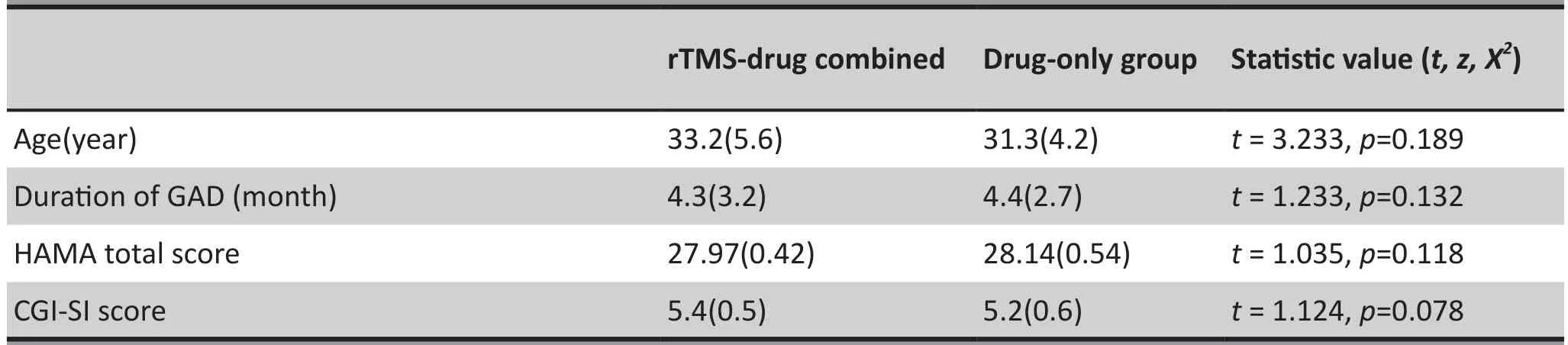
Table 1. The comparison of mean and standard of deviation between groups
(t, z, X2) 2ndweekend p-value 4thweekend p-value 6thweekend p-value
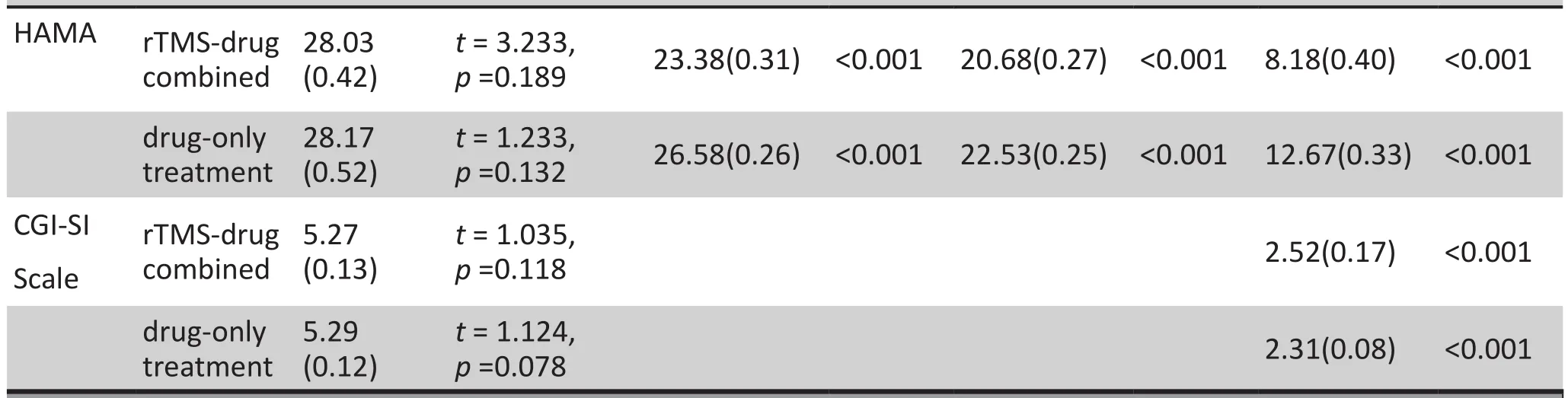
Table 2. The comparison of mean and standard of HAMA, CGI-SI before and after treatment

Figure 2. The HAMA scores in rTMS-drug combined group and drug-only group
4. Discussion
4.1 Main finding
The essential feature of generalized anxiety disorder is persistent and excessive worry about several aspects of one’s life or the welfare of loved ones. Results suggest that clinical symptoms of GAD could improve both on rTMS-drug combined group and single drug group, but efficacy of rTMS-drug groups are better than single drug treatment group. Low frequency rTMS (1Hz), which we used, were been reported in a previous study as an effective way in treatment to posttraumatic stress disorder without major depression disorder. Likewise,we found it do have effect on treatment of GAD. Since the right anterior frontal lobe of brain is related to maintenance of attention, and the rTMS could influence the processing of emotion of right anterior frontal lobe, hence the mechanism of improvement of GAD symptoms prompt by rTMS is probably associated with refining process of attention and emotion in the right anterior frontal lobe.
This study indicated that scores of HAMA and CGI-SI of both two groups after treatment are significantly lower than the scores before it. After a 6-week treatment, the HAMA and CGI-SI scores of drugcombined groups are significantly lower than group only used drug, meanwhile the reduce rate of HAMA score increased with prolonged treatment time. No several adverse effects occurred in both groups. A previous research shows that comparing with paroxetine alone, the combination with rTMS could relive anxiety symptoms in short period of time. We infer, accordingly,the rTMS’s efficacy in treatment of GAD is not related to what types of drugs it combines.
4.2 Limitations
Although the rTMS combined with venlafaxine and lorazepam have a significant efficacy in the treatment of GAD, the current research is unable to determine the precise role of rTMS in anti-anxious treatment such as whether the rTMS only has effect as a synergist of drugs or it do has independent anxiolytic effect, and would there any difference between various drugs combined with rTMS. Another limitation is that the long-term efficacy such as recurrence is still not unclear after this 6-week, short-term observation. In this study, in order to avoid the explanation difficulty of anxiety impacted by menstrual cycle, only males were included in. It will be necessary for future clinical studies aiming at females on a large scale, which is absent yet.
4.3 Implication
This study found that rTMS combined with venlafaxine has a significant efficacy in treatment of generalized anxiety. This article also provided a new possibility to direct the treatment of GAD.
Funding
This research was supported by the National Nature Science Fund of China (grant number: 81360211).
Conflict of interest statement
All authors report that no conflict of interest related to this article.
Informed consent
All participants provided the informed consent in handwriting form.
Ethical review approval
All procedures of the study were being consent by ethic committee of JiangXi Mental Health Centre.
Author contributions
WHL was in charge of project design, data analysis,article writing, and data collection. HMR was in charge of project design and communication. LQS was in charge of data collection and analysis. ZXM, LP, BC,SYH, and CL were in charge of data collection.
Reference:
1. Hill MN, Gorzalka BB. The endocannabinoid system and the treatment of mood and anxiety disorders. CNS Neurol Disord Drug Targets. 2009; 8(6): 451-458. doi: http://dx.doi.org/10.2174/187152709789824624
2. Ressler KJ, Mayberg HS. Targeting abnormal neural circuits in mood and anxiety disorders: from the laboratory to the clinic. Nat Neurosci. 2007; 10(9): 1116-1124. doi: http://dx.doi.org/10.1038/nn1944
3. Tyc F, Boyadjian A. Cortical plasticity and motor activity studied with transcranial magnetic stimulation. Reviews In The Neurosciences. 2006; 17: 469-496. doi: http://dx.doi.org/10.1515/REVNEURO.2006.17.5.469
4. Wan JG. [A control study of sertraline plus RTMS in the treatment of treatment-resistant depression]. Lin Chuang Xin Shen Ji Bing Za Zhi. 2011; 17: 202-204.Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1672-187X.2011.03.0202-006-03
5. Huang JW, Lv WZ, Liu GN, Li YT. [A control study of sertraline plus repetitive transcranial mag-netic stimulation in treatment-refractory obsessive-compulsive disorder].Lin Chuang Xin Shen Ji Bing Za Zhi. 2013; 19: 407-409.Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1672-187X.2013.05.009-0407-03
6. Liu R, Wang JJ, Liu Y, Li H, Zhang MD, Jiang KD, et al.[Comparative study for influence of rTMS on cognitive function in schizophrenia]. Shanghai Arch Psychiatry. 2008;20: 257-260. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1002-0829.2008.05.001
7. Zhang C, Zhang YH. [A control study of paroxetine plus rTMS in generalized anxiety disorders]. Lin Chuang Xin Shen Ji Bing Za Zhi. 2015; 21: 24-26. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1672-187X.2015.01.008-0024-03
8. Zhang XM, Han P, Cheng HL, Yang P, Liu KZ, Hu JM, et al.[Preliminary study on the early-stage efficacy of repetitive transcranial magnetic stimulation(rTMS)in combination with medication in the treatment of generalized anxiety disorder(GAD)]. Shen Jing Ji Bing Yu Jing Shen Wei Sheng.2010; 10(6): 569-571. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1009-6574.2010.06.010
9. Hu XH, Zou HL, Tang BL, Lei GS, Su CJ. [Clinical observation of repetitive transcranial magnetic stimulation in the treatment of anxiety insomnia in 38 patients]. Zhong Hua Shi Yong Zhen Duan Yu Zhi Liao Za Zhi. 2014; 28(2):158-159. Chinese. doi: http://dx.chinadoi.cn/10.13507/j.issn.1674-3474.2014.02.022
10. Hao HJ, Wang XY. [Clinical effect of repeat transcranial magnetic stimulation of electric acupuncture combined with drug in treating anxiety disease]. Tianjin Zhong Yi Yao. 2011;28(2): 125-127. Chinese
11. Isogawa K, Fujiki M, Akiyoshi J, Tsutsumi T, Horinouchi Y,Kodama K, et al. Anxiety induced by repetitive transcranial magnetic stimulation is suppressed by chronic treatment of paroxetine in rats. Pharmacopsychiatry. 2003; 36: 7-11. doi:http://dx.doi.org/10.1055/s-2003-38085
12. Keck ME, Welt T, Post A, Müller MB, Toschi N, Wigger A,et al. Neuroendocrine and behavioral effects of repetitive transcranial magnetic stimulation in a psychopathological animal model are suggestive of antidepressant-like effects.Neuropsychopharmacology. 2001; 24(4): 337-349. doi:http://dx.doi.org/10.1016/S0893-133X(00)00191-3
13. Kanno M, Matsumoto M, Togashi H, Yoshioka M, Mano Y.Effects of repetitive transcranial magnetic stimulation on behavioral and neurochemical changes in rats during an elevated plus-maze test. J Neurol Sci. 2003; 211: 5-14. doi:http://dx.doi.org/10.1016/S0022-510X(03)00030-3
14. Wang C, Chu YM, Zhang YL, Zhang N, Zhang J, Yang H, et al. [Factorial structure of the Hamilton anxiety scale]. Lin Chuang Jing Shen Yi Xue Za Zhi. 2011; 21(5): 266-301.Chinese
15. Zuo S, Byrne LK, Peng D, Mellor D, McCabe M, Zhang J, et al. Symptom severity is more closely associated with social functioning status in inpatients with schizophrenia than cognitive deficits. Shanghai Arch Psychiatry. 2012; 24(2): 83.doi: http://dx.doi.org/10.3969/j.issn.1002-0829.2012.02.003
16. Pallanti S, Bernardi S. Neurobiology of repeated transcranial magnetic stimulation in the treatment of anxiety: a critical review. Int Clin Psychopharmacol. 2009; 24(4): 163-173. doi:http://dx.doi.org/10.1097/YIC.0b013e32832c2639
17. Rosenberg PB, Mehndiratta RB, Mehndiratta YP, Wamer A, Rosse RB, Balish M. Repetitive transcranial magnetic stimulation treatment of comorbid posttraumatic stress disorder and major depression. J Neuropsychiatry Clin Neurosci. 2002; 14: 270-276. doi: http://dx.doi.org/10.1176/jnp.14.3.270
18. Cabeza R, Nyberg L. Imaging cognition II: An empirical review of 275 PET and fMRI studies. J Cogn Neurosci. 2000; 12: 1-47.
19. van Honk J, Schutter DJ, d’Alfonso AA, Kessels RP, de Haan EH. 1 hz rTMS over the right prefrontal cortex reduces vigilant attention to unmasked but not to masked fearful faces. Biol Psychiatry. 2002; 52(4): 312-317. doi: http://dx.doi.org/10.1016/S0006-3223(02)01346-X

Dr. Huiling Wu obtained a bachelor degree of Nanchang University, the Second Clinical Medical College in 2007. Now she is studying the Master program in psychiatry and mental health at Nanchang University. She started to work at department of psychology of JiangXi Mental Health Centre since 2007, and now she has been an attending physician. Her main research interests focus on the drug treatment and psychotherapy on depressive disorder, anxiety disorder, and obsessivecompulsive disorder.
重复经颅磁刺激联合文拉法辛及劳拉西泮治疗广泛性焦虑
吴慧玲,胡茂荣,余斌,刘桥生,王慧芳
广泛刺激性焦虑;文拉法辛;低频重复经颅磁;汉密尔顿焦虑量表;临床疗效总评量表-病情严重程度分量表
Background:Generalized Anxiety Disorder (GAD) is one of common disorder in psychiatric department.However, about 25% patients are unresponsive to both drug and psychotherapy such as cognitive behaviour therapy. The repetitive transcranial magnet stimulation (rTMS) is widely applied in treatment of schizophrenia, major depression disorder, generalized anxiety disorder, obsessive-compulsive disorder and other types of mental disorders, and has a promising effect.Aim:To evaluate the curative effect and safety using venlafaxine combined with repetitive transcranial magnet stimulation in treatment of generalized anxiety disorder.Methods: Seventy patients with a diagnosis of GAD were recruited and randomly divided into two groups.The study group received oral administration of venlafaxine and lorazepam and stimulation of repetitive transcranial magnet. The control group only received venlafaxine and lorazepam. After 6-week observation,Hamilton Anxiety Scale (HAMA) and Clinical Global Impression Severity (CGI-SI) were performed to evaluate the effect of treatment, and Treatment Emergent Symptoms Scale to assess the side effects.Results:While the symptoms of GAD were improved in both groups after 6-week therapy, the efficacy of the drug-rTMS combined group is superior to another.Conclusions:The findings of this study indicate that repetitive transcranial magnet stimulation combined with venlafaxine has a significant therapeutic effect treating GAD.
[Shanghai Arch Psychiatry. 2016; 28(4): 212-217.
http://dx.doi.org/10.11919/j.issn.1002-0829.215092]
Jiangxi Mental Health Centre, Nanchang, Jiangxi Province, China
*Correspondence: MaoRong HU, Mailing address: JiangXi Mental Health Centre, Nanchang, Jiangxi, China. Postcode: 330029. E-Mail: 22345088@qq.com
背景:焦虑障碍是精神科最常见的疾病之一,但是25%的患者对药物,心理及认知行为治疗等无反应。重复经颅磁刺激目前已广泛用于精神分裂症,抑郁症,焦虑症,强迫症等精神障碍的治疗,并取得了满意的疗效。目标:探讨文拉法辛联合重复经颅磁刺激治疗广泛性焦虑症的疗效和安全性。方法:70例广泛性焦虑症患者随机分为两组,研究组口服文拉法辛及劳拉西泮联合重复经颅磁刺激治疗,对照组单用文拉法辛劳拉西泮治疗,连续观察6周。与治疗前后采用汉密尔顿焦虑量表及临床疗效总评量表-病情严重程度分量表评定临床疗效,副反应量表评定不良反应。结果:治疗后两组均能改善广泛性焦虑患者的临床症状,但是药物联合rTMS治疗组疗效要优于单纯药物治疗组。结论:重复经颅磁刺激治联合文拉法辛治疗对广泛性焦虑有显著的疗效
猜你喜欢
基层中医药(2022年5期)2022-10-24
中国药学药品知识仓库(2022年9期)2022-05-23
神州·中旬刊(2019年3期)2019-04-07
新世纪智能(语文备考)(2018年9期)2018-11-08
国外医药(抗生素分册)(2016年6期)2016-07-10
四川精神卫生(2015年4期)2015-12-23
四川精神卫生(2015年4期)2015-12-23
四川精神卫生(2015年4期)2015-12-23
中国火炬(2012年7期)2012-07-25
- 上海精神医学的其它文章
- Some thoughts on the common issue of psychotherapy in different cultures — report on the China conference of psychoanalysis
- Treatment effect of antipsychotics in combination with horticultural therapy on the inpatients with schizophrenia: a randomized, case-controlled study
- A comparison study of Quetiapine and Risperidone’s effectiveness and safety on treating alcohol-induced mental disorder
- The prospects for the clinical application of exploratory eye movement among patients with psychotic disorders
- A case report of psychoactive drugs aggravating and alleviating Meige syndrome
- Malignant syndrome or withdrawal reaction?