股骨头坏死的分期与分型
2017-06-21 10:30孙伟李子荣
中国骨与关节杂志 2017年6期
孙伟 李子荣
. 综述 Review .
股骨头坏死的分期与分型
孙伟 李子荣
股骨头坏死;分期;分型
股骨头坏死是指股骨头血供受损或中断,导致骨髓成分及骨细胞死亡,随后发生修复,继而导致股骨头结构改变甚至塌陷的系列病理改变与临床表现,是目前骨科领域的世界性难题和挑战[1]。股骨头坏死一经诊断,则应分期。分期的目的是用于指导制订治疗方案,判断预后,评估疗效。国际上常用的有 Ficat 和 Alert 分期、Marcus、Enneking 和 Massam 等分期、Sugioka 分期、Pennsylvania大学分期、ARCO 分期、日本骨坏死研究会 ( JIC ) 分型等,都有一定的应用价值。根据近年来的临床实践,以Pennsylvania 大学分期为基础,并作改良,制订了 ONFH中国分期[2]。本文就各种分期与分型逐一介绍如下。
一、Ficat 和 Alert 分期
Ficat 和 Alert 在 1960 年创立了第一个骨坏死的分期[3],最早分为三期,后在 1970 年改良为四期。这一分期目前应用仍较为广泛。这一分期中包含了症状和体征与对应的部分影像学变化,也包含了早期骨坏死功能学检查,如骨扫描,但没有使用 MRI 进行分期。目前仍使用的改良 Ficat 分期包括了 MRI 的应用,而去除了骨扫描和活检等功能学检查方法。这一分期的缺点是没有对坏死的体积和关节受累程度进行评估,因此不能用于判断坏死体积的大小及关节受损程度的进展情况。具体分期如下:
0 期:临床前期及影像学前期;Ficat 认为,当一侧髋关节明确诊断为骨坏死时,另一侧髋关节则很有可能为骨坏死 O 期。Hungerford 将这一阶段称为“静息髋”。
I 期:最早开始出现髋关节疼痛表现,而未发生 X 线改变。
II 期:股骨头出现 X 线改变;骨坏死周围出现硬化带或因脱钙致坏死区域小囊肿形成。
II~III 期移行期:软骨下骨折,新月征形成,股骨头部分塌陷、变扁。
III 期:该期以 X 线片中出现特殊性死骨为特征;由于关节边缘下方骨板不断发生断裂,从而使得死骨变得更加明显,随后股骨头骨坏死区塌陷,但关节间隙正常。
IV 期:股骨头坏死终末期;该期以关节软骨渐进性丢失及髋臼骨赘形成为特征;其 X 线表现为髋关节骨关节炎及股骨头畸形。
二、Marcus,Enneking 和 Massam 分期
1973 年,Marcus,Enneking 和 Massam 创立了骨坏死的影像学六期分期[4],这一分期法将每一期影像学与组织学表现以及患者的症状、体格检查分别对应起来,但没有影像学前期,且那个年代 MRI 也没得到应用,此外这一分期的缺点也是没有对坏死区进行定量。但后来Urbaniak 等[5]进行了改良,Enneking 也将 MRI 和定量方法补充了进来[6-7]。
三、Sugioka 分期
1976 年,Sugioka[8]将股骨头坏死影像学分期简单概括为一个四类分期法,尽管这种分期法没有定量坏死区,但在侧位 X 线上给出了一个测量坏死范围的方法[9]。这对股骨头旋转截骨预后的判断起重要作用,为保证完整的表面部分能转到负重区,可利用坏死区的部位来确定截骨后是向前旋转还是向后旋转。
四、Pennsylvania 大学分期
Pennsylvania 大学分期在 20 世纪 80 年代发展起来[10],该分期将骨坏死分为 7 个明确限定阶段的影像学分期,最初将骨扫描纳入,后来增补并由 MRI 替换。坏死区大小和关节受累程度完美的融合到这一分期,并在每一期再细分为轻、中、重三度。患者症状和体格检查并没有作为分期的组成部分,但明确指出在决定治疗方案时需充分考虑这些因素。Pennsylvania 大学骨坏死分期系统的两大特点为:结合 MRI 检查方法;采用特定的坏死灶测量技术作为该分期系统不可分割的一部分。以上两个特点被认为是所有接受的骨坏死分期系统的必要条件;在骨坏死出现 X 线改变之前,MRI 是早期诊断的最佳检查方式,其灵敏度与特异度已被大家所公认,从而使得侵入性检查、骨扫描技术及 CT 检查不再成为必要检查。
总之分期有两个重要特征,一是其融入了坏死区大小的测量和关节受累的程度,二是使用 MRI 作为确定分期的特定检测方法[11]。目前也被广泛应用。
五、日本骨坏死研究会 ( JIC ) 分期
为使股骨头坏死的临床定义和管理规范化,在卫生福利部门支持下,日本骨坏死研究会在 1986 年制订了股骨头坏死的诊断、分期、分型标准。至今已经修订过三版,并且 2001 年修订版在日本仍然被广泛应用[12-13]。该股骨头坏死分期评估按照 Ficat 的四期法,但在 II 期和 III 期病例中,根据坏死的部位、类型和坏死程度进行了分型,而对 I 期和 IV 期未进行分型,也并未对坏死塌陷和关节受累情况进行评估。这种分期主要在日本国内得到应用。
六、ARCO 分期
国际骨坏死与骨循环协会 ( ARCO ) 在 1991 年对骨坏死进行了命名、诊断标准和分期的统一[14]。ARCO 同样认为建立一个统一的基于疾病不同阶段的分类方法具有十分的必要性。协会认为,分期是定义疾病发展进程的方法。分期须包括疾病发生的起始阶段即 0 期,直至末期关节完全破坏。协会认同对坏死灶范围行定量测量的必要性和建立描述性组织学病理分类方法的迫切性。ARCO 分期基本沿袭了 Pennsylvania 大学分期,1992 年补充进了 JIC 分期中的坏死部位,但后来发现坏死部位的补充使得该分期过于复杂[15-16]。在 1993 年,将 III 期和 IV 期、V 期和 VI 期合并,这样原来的七期分期成为五期[17]。后来,不再将不伴有塌陷的新月征作为单独一期存在,并将补充的 JIC 分期中的坏死部位去除以避免使其分期复杂化。
七、其它评估方法
除了上述分期,还有很多学者进行了坏死区大小的测量研究。1974 年,Kerboul 等[18]指出近端股骨截骨的预后与坏死区的部位和大小程度有关,主要通过测量正侧位X 线片上坏死区的弧度覆盖关节表面的大小,并将其命名为联合坏死角 ( combined necrotic angle ),这些笔者发现了屈曲内收位截骨的预后与坏死区的大小及部位的关系[19]。Wagner 和 Zeiler[20]报道了类似结果。在 1995 年,Koo 和Kim 使用 MRI 代替 X 线进行了相似的角度测量来预测截骨术的预后,这种测量方法被称为坏死指数,其与关节面受累的百分比有关,并用来区分坏死区的大小[21]。2003年,Cherian 等[22]对这种方法进行了很小的改良,即将MRI 的正中矢状位层面替换为面积最大层面,并称其为改良坏死指数。在 2006 年,Ha 等[23]报道使用改良 Kerboul角,测量 MRI 正中冠状位和正中矢状位层面,并将股骨头坏死区分为四级。这些粗略测量坏死角度来评估坏死区大小的方法相对简单,并能初步判断治疗方法如保守治疗、髓芯减压的有效性等[24]。
2013 年 3 月,ARCO 在国际骨坏死论坛之前组织全世界各国专家就骨坏死分期进行了一个研讨会。笔者有幸受到邀请参加了此次在芝加哥举办的研讨会。与会专家一致认为骨坏死分期治疗将对指导制订治疗方案,判断预后,评估疗效起到重要作用,这需要更深入系统的研究,很多专家对该领域很感兴趣。
八、中国分期和中日友好医院 ( CJFH ) 分型
2014 年 12 月,中华医学会骨科学分会关节外科学组召集国内骨坏死研究及诊疗专家讨论,制订了《股骨头坏死临床诊疗规范》[2],制订了中国分期,见表 1。同时,推荐使用中日友好医院分型[25],见图 1。
综上所述,股骨头坏死分期与分型有很多种,各种分期制订在不同的时代背景下,各有自己使用的优点及局限性,最近一些综述发现 25 年来骨坏死治疗的报道仍多使用非定量的分期方法,尤其是 Ficat 四期法使用最多,但有逐渐被 ARCO 和 Pennsylvania 大学分期替代的趋势。中国作为骨坏死的第一大国,中国医师拥有大量的临床实践,并在临床实践中发现了原分期的各自局限性,制订中国分期是必要的,目前中国分期和中日友好医院分型的使用仍需推广,并应该将我国的骨坏死研究成果推向世界。
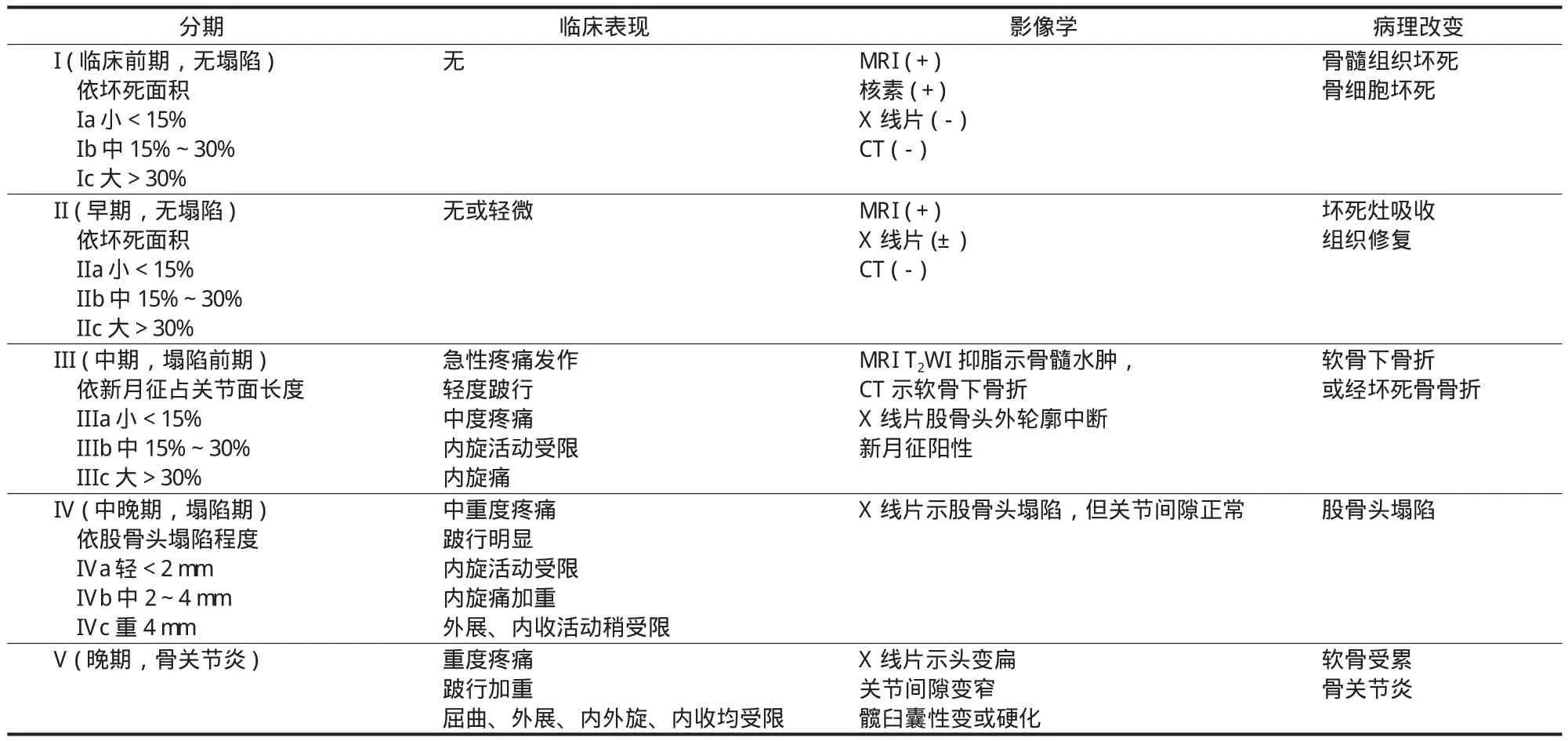
表 1 股骨头坏死:中国分期Tab.1 Schematic representation of the China-Japan Friendship Hospital classif i cation of osteonecrosis of the femoral head based on the three pillars

图 1 中日友好医院分型是以股骨头三柱结构为基础,以坏死灶占据的三柱结构情况,选用 MRI 或 CT 扫描冠状位正中层面,分为:M 型 ( 内侧型 ) 坏死灶占据内侧柱;C 型 ( 中央型 ) 坏死灶占据中央柱;L1 型 ( 次外侧型 ) 坏死灶占据外、中及内侧柱,但外侧柱部分存留;L2 型 ( 极外侧型 ) 坏死灶占据外侧柱,中央、内侧柱存留;L3 型 ( 全股骨头型 ) 坏死灶占据全股骨头Fig.1 Schematic representation of the China-Japan Friendship Hospital classif i cation of osteonecrosis of the femoral head based on the three pillars. Type M: necrosis involved the medial pillar. Type C: necrosis involved both medial and central pillars. Type L1: necrosis involved the three pillars, but the partial lateral pillar was persevered. Type L2: necrosis involved whole lateral pillar and partial central pillar. Type L3: necrosis involved the three pillars including the cortical bone and marrow
[1] Choi HR, Steinberg ME, Y Cheng E. Osteonecrosis of the femoral head: diagnosis and classif i cation systems[J]. Curr Rev Musculoskelet Med, 2015, 8(3):210-220.
[2] 李子荣. 股骨头坏死临床诊疗规范[J]. 中华骨与关节外科杂志, 2015, 8(1):1-6.
[3] Arlet J, Ficat P. Forage-biopsie de la tete femorale dans l’osteonecrose primitive. Observations histopathologiques portent sur huit foranes[J]. Rev Rheum, 1964, 31:257-264.
[4] Marcus ND, Enneking WF, Massam RA. The silent hip in idiopathic aseptic necrosis: treatment by bone grafting[J]. J Bone Joint Surg Am, 1973, 55(7):1351-1366.
[5] Urbaniak JR, Coogan PG, Gunneson EB, et al. Treatment of osteonecrosis of the femoral head with free vascularized fi bular grafting[J]. J Bone Joint Surg Am, 1995, 77(5):681-694.
[6] Enneking WF. Classification of nontraumatic osteonecrosis of the femoral head. In: Urbaniak JR, Jones JP, editors. Osteonecrosis: etiology, diagnosis and treatment[M]. Rosemont: American Academy of Orthopaedic Surgeons, Developed by the American Orthopaedic Association. 1997: 269-725.
[7] Alolriclge JM 3rd, Berend KR, Gunneson EE, et al. Free vascularized fabular grafting for the treatment of post collapse osteonecrosis of the femoral head surgical techigne[J]. J Bone Joint Surg Am, 2004, 86-A(Suppl 1):87-101.
[8] Sugioka Y. Transtrochanteric anterior rotational osteotomy of the femoral head in the treatment of osteonecrosis affecting the hip[J]. Clin Orthop, 1978, 130(130):191-201.
[9] Sugioka Y, Katsuki I, Hotokebechi T. Transtrochanteric rotational osteotomy of the femoral head for the treatment of osteonecrosis: follow-up statistics[J]. Clin Orthop, 1982, 46(169):115-126.
[10] Steinberg ME, Hayken GD, Steinberg DR. A quantitative system for staging avascular necrosis[J]. J Bone Joint Surg Br, 1995, 77(1):34-41.
[11] Steinberg ME, Hayken GD, Steinberg DR. A new method for evaluation and staging of avascular necrosis of the femoral head. In: Arlet J, Ficat RP, Hungerford DS, editors. Bone circulation[M]. Baltimore: Williams & Wilkins. 1984: 398-403.
[12] Ono K. Diagnostic criteria, staging system and roentgenographic classifi cation of avascular necrosis of the femoral head (steroid induced, alcohol associated or idiopathic nature (in Japanese). In:Ono K, editor. Annual report of Japanese investigation committee for intractable disease, avascular necrosis of the femoral head[M]. Tokyo: Ministry of Health and Welfare. 1987: 331-336.
[13] Sugano N, Takaoka K, Ohzono K, et al. Rotational osteotomy for of non-traumatic avascular necrosis of the femoral head: signif i cance of location and size of the necrotic lesion[J]. Clin Orthop, 1992, 74(5):734-739.
[14] Gardeniers J. ARCO committee on terminology and staging. A new proposition of terminology and an international classif i cation of osteonecrosis[J]. ARCO Newslett, 1991, 3:153-159.
[15] Gardeniers JWM. A new international classifi cation of osteonecrosis of the ARCO committee on terminology and classif i cation[J]. ARCO Newslett, 1992, 4:41-46.
[16] Gardeniers JWM. The ARCO perspective for reaching one uniform staging system of osteonecrosis. In: Schoutens A, Arlet J, Gardiniers JWM, Hughs SPF, editors. Bone circulation and vascularization in normal and pathological conditions[M]. New York: Plenum Press. 1993: 375-380.
[17] Gardeniers JWM. ARCO Committee on Terminology and Staging. Report on the Committee Meeting at Santiago de Compostella[J]. ARCO Newslett, 1993, 5:79-82.
[18] Kerboul M, Thomine J, Postel M, et al. The conservative surgical treatment of idiopathic aseptic necrosis of the femoral head[J]. J Bone Joint Surg Br, 1974, 56(2):291-296.
[19] Mont MA, Jones LC, Pacheo I, et al. Radiographic predictors of outcome of core decompression for osteonecrosis stage III[J]. Clin Orthop, 1998, 354(354):159-168.
[20] Wagner H, Zeiler G. Idiopathic necrosis of the femoral head: results of intertrochanteric osteotomy and joint resurfacing. In: Weill U, editor. Segmental idiopathic necrosis of the femoral head: progress in orthopaedic surgery[M]. Berlin: Springer. 1981: 87-116.
[21] Röntgen KH. Quantifying the extent of osteonecrosis of the femoral head: a new method using MRI[J]. J Bone Joint Surg Br, 1995, 77(6):875-880.
[22] Cherian SF, Laorr A, Saleh KJ, et al. Quantifying the extent of femoral head involvement in osteonecrosis[J]. J Bone Joint Surg Am, 2003, 85-A(2):309-315.
[23] Ha YC, Jung WH, Kim JR, et al. Prediction of collapse in femoral head osteonecrosis: a modif i ed Kerboul method with use of magnetic resonance images[J]. J Bone Joint Surg, 2006, 88-A(Suppl 3):S35-40.
[24] Steinberg DR, Steinberg ME, Garino JP, et al. Determining lesion size in osteonecrosis of the femoral head[J]. J Bone Joint Surg, 2006, 88-A(Suppl 3):S27-34.
[25] 李子荣, 刘朝晖, 孙伟, 等. 基于三柱结构的股骨头坏死分型——中日友好医院分型[J]. 中华骨科杂志, 2012, 32(6): 515-520.
( 修回日期:2017-01-14 )
( 本文编辑:裴艳宏 )
Staging classif i cation of osteonecrosis of femoral head
SUN Wei, LI Zi-rong. Department of Orthopedics, China-Japan Friendship Hospital, Beijing, 100029, China
LI Zi-rong, Email: lizirongon@163.com
Osteonecrosis of femoral head is a kind of chronic, progressive and disabling disease. Once the diagnosis is established, staging classif i cation is needed for guidance of treatment, prognosis and evaluation of curative effects. Currently, many staging classif i cation methods are used, such as Ficat and Alert, Marcus, Enneking & Massam, Sugioka, the university of Pennsylvania, ARCO staging system and Japan research institute ( JIC ) classif i cation, etc. Each of these systems has its advantages and application values, as well as its shortcomings and limitations. And the most widely applied is 4 stages of Ficat staging system in early times, which has been modif i ed to 6 stages now and gradually replaced by ARCO and the university of Pennsylvania staging system. Chinese doctors have a large number of cases, and have found their respective limitations of the original staging and classification systems in clinical practice. We’ve made our own Chinese staging system and China-Japan Friendship Hospital ( CJFH ) classif i cation, these staging and classif i cation systems still need to be promoted at present.
Femur head necrosis; Staging; Types
10.3969/j.issn.2095-252X.2017.06.013
R684
国家自然科学基金 ( 81372013,81672236 );中日友好医院青年科技英才计划 ( 2004-QNYC-A-06 )
作者单位:100029 北京,中日友好医院骨科
李子荣,Email: lizirongon@163.com
2015-09-24 )
猜你喜欢
中日友好医院学报(2022年2期)2022-11-26
中华骨与关节外科杂志(2022年1期)2022-08-31
基层中医药(2022年4期)2022-07-22
昆明医科大学学报(2021年5期)2021-07-22
中日友好医院学报(2021年2期)2021-01-03
中日友好医院学报(2021年1期)2021-01-02
中日友好医院学报(2020年2期)2020-01-10
中国中医急症(2019年10期)2019-05-21
老友(2018年2期)2018-04-08
药学研究(2015年11期)2015-12-19