磁共振弥散加权成像对宫颈癌盆腔淋巴结转移诊断的应用价值
2017-10-20 10:37董乐丹肖琴琴叶琼许化致杨运俊
中国现代医生 2017年25期
关键词:宫颈癌
董乐丹+肖琴琴+叶琼+许化致+杨运俊


[摘要] 目的 探讨磁共振弥散加权成像对宫颈癌盆腔淋巴结转移诊断的临床应用价值。 方法 收集2015年8月~2016年10月我院收治的26例行盆腔淋巴结清扫术的宫颈癌患者的术前MRI检查资料,术后均经病理检查证实。比较分析宫颈癌原发灶、转移淋巴结及非转移淋巴结的ADC值差异;比较转移淋巴结与非转移淋巴结最长径、最短径及短/长径之比。 结果 ①26例宫颈癌患者中转移性淋巴结56枚,非转移性淋巴结78枚;②转移性淋巴结ADC均值为(874.19±158.72)×10-6 mm2/s),较非转移性淋巴结ADC均值[(921.45±232.98)×10-6 mm2/s]略降低,但两者间差异无统计学意义(P>0.05);宫颈癌原发灶ADC均值为(918.78±146.06)×10-6 mm2/s),与转移淋巴结、非转移淋巴结ADC均值两两比较,差异均无统计学意义(P>0.05);③转移性淋巴结与非转移性淋巴结最长径中位数分别为16.50 mm、7.00 mm,最短径中位数分别为8.50 mm、5.00 mm,短长径比的中位数为0.55、0.65,两两比较差异有统计学意义(P<0.05)。 结论 DWI有利于盆腔淋巴结的检出,但是ADC值测量对转移性淋巴结的临床诊断价值并不大。
[關键词] 宫颈癌;磁共振弥散加权成像;转移性淋巴结;ADC值
[中图分类号] R737.33 [文献标识码] B [文章编号] 1673-9701(2017)25-0101-04
The application value of magnetic resonance diffusion weighted imaging in the diagnosis of pelvic lymph nodes metastasis of cervical cancer
DONG Ledan XIAO Qinqin YE Qiong XU Huazhi YANG Yunjun
Department of Radiology, the First Affiliated Hospital of Wenzhou Medical University, Wenzhou 325000, China
[Abstract] Objective To explore the clinical application value of MR diffusion weighted imaging in the diagnosis of pelvic lymph node metastasis of cervical cancer. Methods The preoperative MRI examination data of 26 patients with cervical cancer who underwent pelvic lymphadenectomy in our hospital from August 2015 to October 2016 were enrolled in this study. The diagnosis of all cases was confirmed by postoperative MRI findings. The differences of ADC values among primary cervical cancer, metastatic lymph nodes and non-metastatic lymph nodes were analyzed. The longest diameter, the shortest diameter and the ratio of the short/long diameter were compared. Results ①There were 56 metastatic lymph nodes and 78 non-metastatic lymph nodes in 26 cases of cervical cancer. ②The mean value of metastatic lymph node ADC[(874.19±158.72)×10-6 mm2/s] was slightly lower than that of non-metastatic lymph node [(921.45±232.98)×10-6 mm2/s], but there was no significant difference between the two groups(P>0.05). There was no significant difference in the ADC value among the primary tumor[(918.78±146.06)×10-6 mm2/s], metastatic lymph node and non-metastatic lymph node of cervical cancer(P>0.05). ③The median of the longest diameter of the metastatic lymph nodes and the non-metastatic lymph nodes was 16.50 mm and 7.00 mm, respectively. The median of the shortest diameter was 8.50 mm and 5.00 mm, respectively. The median of short diameter/long diameter was 0.55, 0.65 respectively. There was statistically significant difference among the groups(P<0.05). Conclusion DWI is helpful for the detection of pelvic lymph nodes, but the clinical diagnostic value of ADC measurement is not significant.endprint
[Key words] Cervical cancer; Magnetic resonance diffusion weighted imaging; Metastatic lymph node; ADC value
宫颈癌是我国女性生殖系统最常见的恶性肿瘤[1]。按照国际FIGO系统,宫颈癌的临床分期与淋巴结是否转移并无直接关联[2],但是具体治疗方案、疗效及预后情况与淋巴结是否转移密切相关[3]。国内外大量文献已经证实淋巴结转移是宫颈癌患者重要的独立危险因素之一[4]。因此,盆腔淋巴结转移是判断预后及指导治疗方案的重要依据[5,6],目前临床工作中MRI诊断主要依据淋巴结形态学改变来判断是否存在转移。国内外许多的研究认为DWI对盆腔各类恶性肿瘤的淋巴结检出及是否转移具有较高的临床价值[7-9],但在确诊盆腔转移性淋巴结尚存在诸多争议[10],本研究主要探讨MRI检查对宫颈癌盆腔淋巴结是否转移的诊断价值,并探讨ADC值的临床价值。
1 资料与方法
1.1一般资料
选择2015年8月~2016年10月于我院行MRI检查且经病理组织检查证实的宫颈癌患者26例作为研究对象,年齡31~76岁,平均53岁,其中鳞癌24例,腺癌1例,其他(原始神经外胚叶肿瘤)1例。纳入标准:(1)经宫颈活检病理诊断明确,临床分期为Ⅰa~Ⅱa期;(2)术前无放化疗等辅助治疗;(3)术前常规行盆腔MRI检查;(4)均行全子宫切除加淋巴结清扫术,术中清楚记录淋巴结部位及数目,术后均有病理结果。排除标准:(1)术前行放化疗检查患者;(2)术前MRI检查时间与手术时间超过20 d。
1.2 仪器与方法
本组所有患者均使用飞利浦Achieva 3.0T TX超导型磁共振扫描,行盆腔MRI常规检查,采用腹部16通道相控阵线圈,依次行DWI、T1WI、轴位T2WI、矢状位T2WI及冠状位T2WI。
1.3 图像处理及评定标准
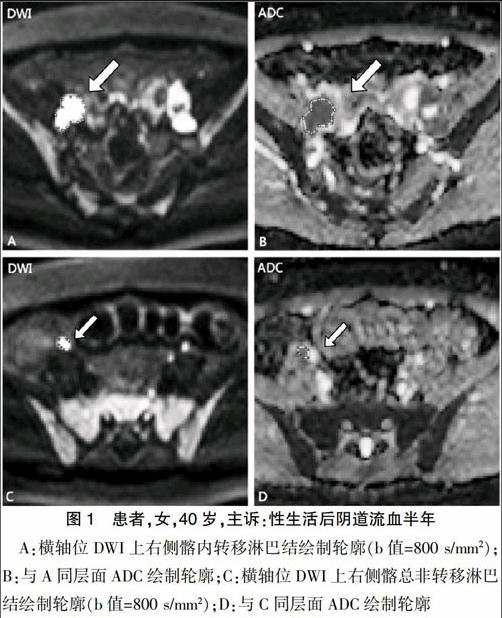
所有数据处理均由具备临床工作经验的两名放射科医师进行。根据手术记录资料、病理结果及常规MR图像,确定子宫原发灶、转移淋巴结及非转移淋巴结。转移淋巴结判定:转移淋巴结指影像上存在1个或1个以上转移征象,手术中确认部位及病理结果确诊,对不能确认者予以剔除。首先将轴位T2WI图像上所有淋巴结短径(Short-axis diameter)≥3 mm者纳入本组研究,同时测量淋巴结长径(Long-axis diameter)。联合常规T1WI及T2WI图像,使用Image Analyzer软件结合DWI于ADC图上绘制宫颈癌原发灶、转移及非转移淋巴结的每一层面感兴趣区而获得病灶体积感兴趣(VOI),然后通过使用Matelab软件计算获得ADC值,如图1所示。
1.4 统计学方法
应用SPSS23.0软件包进行数据分析,盆腔淋巴结长径、短径测量值为偏态分布计量资料,淋巴结最长径、最短径采用中位数及四分位数表示,两组最长径、最短径及短长比采用独立样本秩和检验;两组原发病灶及淋巴结所测ADC均值为计量资料,宫颈癌原发病灶、转移淋巴结及非转移淋巴结三组之间的比较采用方差分析,检验水准α=0.05,P<0.05为差异有统计学意义。
2 结果
2.1 盆腔淋巴结基本资料分析结果
转移性淋巴结与非转移性淋巴结基本分析(部位、形态及边缘)见表1。共收集盆腔淋巴结134枚,其中非转移淋巴结78枚,转移淋巴结56枚。结果提示非转移性淋巴结形态以椭圆形为主,边缘基本光整,淋巴结在盆腔扫描中均可显示。转移性淋巴结仍以椭圆形为主,但在影像上不规则或融合形态更能提示转移性;边缘显示则以毛糙改变为主,盆腔部位并无特殊性。
2.2 转移性淋巴结与非转移性淋巴结最长径、最短径及短长径比
转移性淋巴结与非转移性淋巴结最长径、最短径及短长径比分析见表2。结果表明,盆腔转移性淋巴结与非转移性淋巴结最长径、最短径及短/长径比之间的差异有统计学意义(P均<0.05)。
2.3 宫颈癌原发灶及盆腔淋巴结ADC值分析结果
宫颈癌原发灶、盆腔转移性淋巴结和非转移性淋巴结之间ADC均值结果比较,见表3。结果提示宫颈癌原发病、转移性淋巴结与非转移性淋巴结之间两两比较,差异均无统计学意义(P>0.05)。
3 讨论
宫颈癌是女性生殖系统中最常见的恶性肿瘤之一[1],严重威胁女性的身心健康。宫颈癌的早期诊断、正确分期及淋巴结是否转移的评判对手术方式的选择以及疗效、预后都具有重要意义[2,11]。目前临床上宫颈癌手术均采用全子宫切除加盆腔淋巴结清扫,对患者的创伤较大,会伴有神经损伤、淋巴管囊肿等并发症,因此术前正确评估对临床选择个体化治疗具有重要意义[12],部分患者可以避免盆腔淋巴结的清扫。
磁共振扩散加权成像(DWI)是临床上应用较广泛的功能成像之一,也是目前影像学检查中唯一能够观察组织水分子活动的无创性检查手段[13,14]。DWI成像原理的主要病理性改变是正常组织局部发生病变时,细胞密度、细胞代谢等发生变化,致使水分子的扩散也发生不同程度的变化[7,15]。基于这样的原理磁共振DWI最早是应用于中枢神经系统,尤其是急性脑卒中患者的检查,这是因为急性脑卒中会导致水分子扩散受限[16]。目前也证实DWI对于组织器官良恶性肿瘤的鉴别是很重要的检查手段之一[17],因为恶性肿瘤细胞比正常组织密集以及细胞体积较大[18],因此DWI图像上呈明显高信号,ADC图上呈明显低信号。另外,很多的研究也认为淋巴结在DWI上可以清楚显示高信号[19]。因此关于DWI检查来鉴别转移性淋巴结与非转移性淋巴结的临床价值尚有很多争议[3],部分研究认为于DWI上测量ADC值可以从影像上定量性区分转移及非转移性淋巴结,但目前尚无明确标准值参考范围[7-8];也有部分研究认为DWI联合T2WI上描述淋巴结形态、大小及边缘可以大致检出及评估转移性淋巴结与非转移性淋巴结[18,20]。endprint
本研究結果显示评估盆腔淋巴结是否转移,T2WI对淋巴结形态、边缘及大小的评判可以提供重要的信息,转移性淋巴结形态常显示不规则或融合状态,边缘常常显示毛糙或伴有渗出的改变,同时也可以呈椭圆形或圆形以及边缘光整,因此对淋巴结形态及边缘的描述可以提供一定的信息,但不足以评判是否转移。本研究结果还表明转移性淋巴结与非转移信淋巴结两组间的最长径、最短径及短/长径比之间具有明显差异,且两组间的差异有统计学意义。这与贺李等[21]研究者认为淋巴结的大小可以作为影像评判的主要指标之一相符,该研究还认为淋巴结短径>20 mm,常规MRI基本可以准确诊断为转移性淋巴结,但同时也表明尚不能将短径>10 mm作为评判标准之一,许多研究者通过严格的“点对点”影像及病理结合研究发现<10 mm的转移性淋巴结并不少见[13,18],本研究中也发现此现象。另外,许多的研究[22]认为ADC值可以反映病变组织的特性,可以定量评估转移性淋巴结[23]。本研究发现转移性淋巴结ADC均值低于非转移性淋巴结及宫颈癌原发灶,但是组间差异无统计学意义。虽然目前有研究发现盆腔转移与非转移性淋巴结之间ADC值差异具有显著性差压,但是有研究[24]结果显示ADC值测量对诊断淋巴结是否转移并没有很大贡献。但就本研究分析原因可能如下:(1)大部分研究所测的ADC值是淋巴结或宫颈癌原发病灶单层图像上所画取的兴趣区(region of interest,ROI)ADC值,本研究所测的ADC值为淋巴结或宫颈癌原发灶全体积ADC值的均值,因此可能与研究者使用的方法不同存有一定的关系,而目前尚较少文献使用该方法对淋巴结的是否转移情况进行研究,因此该方法还需要更多的研究。(2)可能与本研究样本不足有一定关系,因此下一步研究需要扩大样本量,此外还可能与研究工作中研究者与的手工画取感兴趣区存有一定的误差有关。
综上所述,3.0T磁共振DWI对宫颈癌盆腔淋巴结的显示具有明显优势,转移性及非转移性淋巴结的最长径、最短径及短/长径比之间的差异有统计学意义,结合淋巴结形态及边缘情况的综合评判可以提高淋巴结转移性诊断的准确性。
[参考文献]
[1] Waggoner SE. Cervical cancer[J]. The Lancet,2003,361(9376):2217-2225.
[2] Pecorelli S. Revised figo staging for carcinoma of the vulva,cervix,and endometrium[J]. International Journal of Gynecology & Obstetrics,2009,105(2):103-104.
[3] Wang YT,Li YC,Yin LL,et al. Can diffusion-weighted magnetic resonance imaging predict survival in patients with cervical cancer? A meta-analysis[J]. European Journal of Radiology, 2016,85(12):2174-2181.
[4] Kim JK,Kim KA,Park BW,et al. Feasibility of diffusion-weighted imaging in the differentiation of metastatic from nonmetastatic lymph nodes:Early experience[J]. Journal of Magnetic Resonance Imaging:JMRI,2008,28(3):714-719.
[5] Liu Y,Liu H,Bai X,et al. Differentiation of metastatic from non-metastatic lymph nodes in patients with uterine cervical cancer using diffusion-weighted imaging[J]. Gynecologic Oncology,2011,122(1):19-24.
[6] Martí-Bonmatí L. Lymph node assessment by diffusion weighted imaging in cervical cancer[J]. European Radiology,2011,21(3):474-477.
[7] Papalia R,Simone G,Grasso R,et al. Diffusion-weighted magnetic resonance imaging in patients selected for radical cystectomy:Detection rate of pelvic lymph node metastases[J]. BJU International,2012,109(7):1031-1036.
[8] Demirbas T,Cimilli T,Bayramoglu S,et al. Contribution of diffusion-weighted imaging to diagnosis and staging of cervical cancer[J]. Balkan Medical Journal,2014,31(2):154-157.
[9] Kuang F,Ren J,Zhong Q,et al. The value of apparent diffusion coefficient in the assessment of cervical cancer [J].European Radiology,2012,23(4):1050-1058.endprint
[10] Chen YB,Liao J,Xie R,et al. Discrimination of metastatic from hyperplastic pelvic lymph nodes in patients with cervical cancer by diffusion-weighted magnetic resonance imaging[J]. Abdominal Imaging,2011,36(1):102-109.
[11] Marzi S,Piludu F,Sanguineti G,et al. The prediction of the treatment response of cervical nodes using intravoxel incoherent motion diffusion-weighted imaging[J]. EuroPean Journal of Radiology,2017,92(6):93-102.
[12] Vandecaveye V,Dresen R,De Keyzer F. Novel imaging techniques in gynaecological cancer[J]. Current Opinion in Oncology,2017,29(5):335-342.
[13] Choi HJ,Roh JW,Seo SS,et al. Comparison of the accuracy of magnetic resonance imaging and positron emission tomography/computed tomography in the presurgical detection of lymph node metastases in patients with uterine cervical carcinoma:A prospective study[J]. Cancer, 2006,106(4):914-922.
[14] Liu B,Gao S,Li S. A comprehensive comparison of ct,mri,positron emission tomography or positron emission tomography/ct,and diffusion weighted imaging-mri for detecting the lymph nodes metastases in patients with cervical cancer:A Meta-analysis based on 67 studies[J]. Gynecologic and Obstetric Investigation,2017,82(3):209-222.
[15] Godeny M,Lengyel Z,Polony G,et al. Impact of 3t multiparametric mri and fdg-pet-ct in the evaluation of occult primary cancer with cervical node metastasis[J]. Cancer Imaging:The Official Publication of the International Cancer Imaging Society,2016,16(1):38.
[16] von Kummer R,Dzialowski I. Imaging of cerebral ischemic edema and neuronal death[J]. Neuroradiology,2017, 59(6):545-553.
[17] Oh E,Yoon YC,Kim JH,et al. Multiparametric approach with diffusion-weighted imaging and dynamic contrast-enhanced mri:A comparison study for differentiating between benign and malignant bone lesions in adults[J]. Clinical radiology,2017,72(7):552-559.
[18] Roy C,Bierry G,Matau A,et al.Value of diffusion-weighted imaging to detect small malignant pelvic lymph nodes at 3 t[J]. European radiology,2010,20(8):1803-1811.
[19] Liang L,Luo X,Lian Z,et al. Lymph node metastasis in head and neck squamous carcinoma:Efficacy of intravoxel incoherent motion magnetic resonance imaging for the differential diagnosis[J]. European Journal of Radiology,2017, 90(5):159-165.
[20] Kitajima K,Yamasaki E,Kaji Y,et al. Comparison of dwi and pet/ct in evaluation of lymph node metastasis in uterine cancer[J]. World Journal of Radiology,2012,4(5):207-214.
[21] 賀李,余深平,庄晓盟,等. 3.0T磁共振DWIBS诊断宫颈癌转移性淋巴结初探[J].影像诊断与介入放射学,2012,19(5):273-276.
[22] Himoto Y,Fujimoto K,Kido A,et al. Pretreatment mean apparent diffusion coefficient is significantly correlated with event-free survival in patients with international federation of gynecology and obstetrics stage ib to iiib cervical cancer[J]. International Journal of Gynecological cancer:Official Journal of the International Gynecological Cancer Society,2015,25(7):1079-1085.
[23] Ju FJ. Evaluation of the efficacy of chemoradiotherapy in cervical cancer using diffusion-weighted imaging and apparent diffusion coefficient[J]. OncoTargets and Therapy, 2016,9(11):7555-7561.
[24] Nakai G,Mitsuru M,Inada Y,et al. Detection and evaluation of pelvic lymph nodes in patients with gynecologic malignancies using body diffusion-weighted magnetic resonance imaging[J]. J Comput Assist Tomogr,2008,32(5):764-768.endprint
猜你喜欢
中老年保健(2021年12期)2021-08-24
中华养生保健(2020年10期)2021-01-18
中国生殖健康(2020年7期)2021-01-18
中国生殖健康(2020年2期)2021-01-18
抗癌之窗(2020年2期)2020-07-14
中国生殖健康(2018年2期)2018-11-06
河北医学(2016年5期)2016-12-01
食管疾病(2015年3期)2015-12-05
中国当代医药(2015年31期)2015-03-01
中国当代医药(2015年17期)2015-03-01