江西成年人群下颌骨体副孔解剖位置的锥形束CT研究
2017-12-14 10:19柯星李博涵陈林林姜新娣
华西口腔医学杂志 2017年6期
柯星 李博涵 陈林林 姜新娣
南昌大学附属口腔医院口腔颌面外科,江西省口腔生物医学重点实验室,南昌 330006
江西成年人群下颌骨体副孔解剖位置的锥形束CT研究
柯星 李博涵 陈林林 姜新娣
南昌大学附属口腔医院口腔颌面外科,江西省口腔生物医学重点实验室,南昌 330006
目的 应用锥形束CT(CBCT)观测江西成年人群下颌骨体副孔的分布位置,为临床安全操作提供依据。
方法 选取200份江西成年人的CBCT资料,按年龄分为4组,每组男女比例相等。描述下颌骨前牙、前磨牙和磨牙各区域的副孔数目和分布位置,分析年龄、性别和左右侧因素与副孔发生率的关系。结果 发现下颌骨体副孔共
1 123个,人均(5.62±2.10)个。副孔发生率自近中区域向远中降低,舌侧副孔发生率高于颊侧,男女性副孔数目无差异(P=0.195),年龄与副孔数目呈负相关(rs=-0.301)。下颌骨体三处副孔高频区域为:正中联合部(98.0%),中、侧切牙牙槽突舌侧(88.0%),前磨牙区的低位(55.0%)。结论 下颌骨副孔每人均会出现,临床需留意避免损伤副孔内容物而引起并发症。
下颌骨; 副孔; 锥形束CT; 下颌解剖
下颌骨副孔是微小的血管或神经分支进入下颌骨的皮质骨开孔。损伤下颌骨副孔内血管会增加口底出血的风险,若神经受损,可造成患者下唇感觉迟钝或异常。有学者[1]认为在颌面部恶性肿瘤于下颌骨颊舌向侵袭中副孔起到重要的作用。
国外学者已应用锥形束CT(cone beam computed tomography,CBCT)的高空间分辨率特性观测下颌骨副孔。国内多以头颅标本为研究对象,局限于副孔发生率、孔径、位置等基本情况的描述,缺乏相关因素分析。本研究通过观测下颌骨体的CBCT图像,描述副孔的发生、位置及毗邻关系,探讨年龄、性别、部位等因素对副孔发生的影响,从而为种植术、颌面外科手术等临床操作的安全进行提供理论依据。
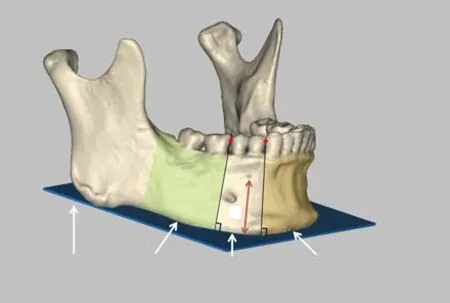
图1 下颌骨体区域划分示意图 Fig 1 Schematic representation of the region division of the man- dibular body
1 材料和方法
1.1 病例收集
收集2014—2015年在南昌大学附属口腔医院行颌骨CBCT扫描的所有患者影像资料。扫描设备和参数:KaVo 3D eXam CBCT,管电压120 kV,管电流5 mA,持续时间14.7 s,直径16 cm,高度13 cm,分辨率(体素)0.25 mm。病例排除标准:1)下颌骨存在病理性损害,包括囊肿、肿瘤、慢性牙周病等;2)有下颌骨骨折和正颌手术病史;3)各种因素造成的CBCT图像模糊,如拍摄移动、金属伪影、操作失误等;4)正畸治疗期间;5)影响下颌骨牙列区域划分的因素,如牙列严重不齐、相邻牙体缺失超过1个。
以年龄组别(20~29岁、30~39岁、40~49岁、50岁及以上共4组)随机抽取患者CBCT影像资料共200份,其中20~29岁组80份,余年龄组各40份,各组男女比例相等。
1.2 测量方法
CBCT影像资料以DICOM格式保存,导入Materialise Mimics 17.0软件中,由2位经过培训的医师分别对下颌骨体部进行观测,并于2周后重复观测。副孔判定标准:从下颌骨皮质骨外侧贯穿至松质骨内的类圆形边界清晰的低密度影。
如图1所示,以尖牙和第一前磨牙冠邻接点、第二前磨牙和第一磨牙冠邻接点作下颌平面垂线(分界线),将下颌骨分为前牙区、前磨牙区和磨牙区,按照左右和颊舌方位共分为12区域,副孔依其所在的位置划分入各区域内。测量副孔中心到下颌平面的垂直距离(记为高度H)以及每个副孔的直径Φ。
1.3 统计学分析
使用IBM SPSS Statistic 20统计软件对实验数据进行统计学分析,副孔数目在年龄、性别上的差异采用秩和检验,不同区域副孔高度的差异采用t检验,α=0.05。
2 结果
本实验观测的200份CBCT影像对应的受试者年龄范围为20~75岁,平均年龄为(35.77±11.81)岁。共发现下颌骨体副孔1 123个,所有受试者均发现副孔,出现率为100%,个体副孔数目1~12个不等,人均(5.62±2.10)个。不同性别和年龄的副孔数目分布情况见表1、2。男性副孔总数为587个,女性副孔总数为536个,男性多于女性,经Mann-Whitney U检验分析得出,二者间差异无统计学意义(P=0.195)。20~29岁、30~39岁、40~49岁、50岁及以上各年龄组的副孔数目分别为508、227、182、206个,经Kriskal-Wallis H检验分析显示,各组副孔数目分布有显著差异(Plt;0.001),年龄和副孔数目呈负相关(rs=-0.301)。
表 1 男女性受试者的下颌骨体副孔数目频数分布情况Tab1 Frequency distribution of male and female subjects with accessory mandibular foramina

表 2 各年龄段受试者的下颌骨体副孔数目频数分布情况Tab 2 Frequency distribution of subjects with accessory mandibular foramina on age groups
下颌骨体副孔在不同区域的分布情况见表3。正中联合部是下颌骨正中连接部位,共196名受试者于此处发现副孔,发生率最高(98.0%),副孔平均高度为(8.21±3.83) mm;其次为左右舌侧前牙区(86.0%,85.0%);颊侧磨牙区发生率最小(5.5%)。由近中向远中副孔发生率呈降低趋势。左右同名牙区域副孔发生率和高度无统计学差异(Pgt;0.05)。
下颌骨体某些特定区域副孔出现次数远高于其他区域,称之为副孔高频区,分别有中、侧切牙牙槽突舌侧(图2),正中联合部(图3),前磨牙区的低位(图4)。这三处高频区副孔分布情况见表4。正中联合部副孔按其所在位置可细分为舌侧颏棘上部、下部以及唇侧3个部分,副孔发生率分别为83.0%、47.5%和3.0%,平均高度分别为(11.07±1.59)、(4.38±2.23)和(3.88±1.96) mm,平均直径分别为(0.92±0.23)、(0.75±0.18)和(0.71±0.19) mm。

表 3 下颌骨体不同区域的副孔分布情况Tab 3 Regional distribution of accessory mandibular foramina according to the tooth area

图2 下颌中、侧切牙牙槽突舌侧副孔,左右侧各1个Fig 2 Accessory mandibular foramina in lingual alveolar area of lower medial and lateral incisors,there are one foramen in each left and right sides
中、侧切牙牙槽突舌侧副孔发生率为88.0%,其中双侧均发生的受试者129人(64.5%),副孔平均高度为(26.45±2.31) mm,平均直径为(0.81±0.23)mm。前磨牙区低位副孔发生率为55.0%,其中双侧均发生的受试者有35人,发生率为17.5%,副孔高度为(3.05±2.17) mm,平均直径为(0.88±0.19)mm。

图3 下颌正中联合部副孔,颏棘上方、下方和唇侧各1个 Fig 3 Accessory mandibular foramina in mandibular symphysis area, there are one foramen in each superior and inferior ge- nial spinal and the labial side
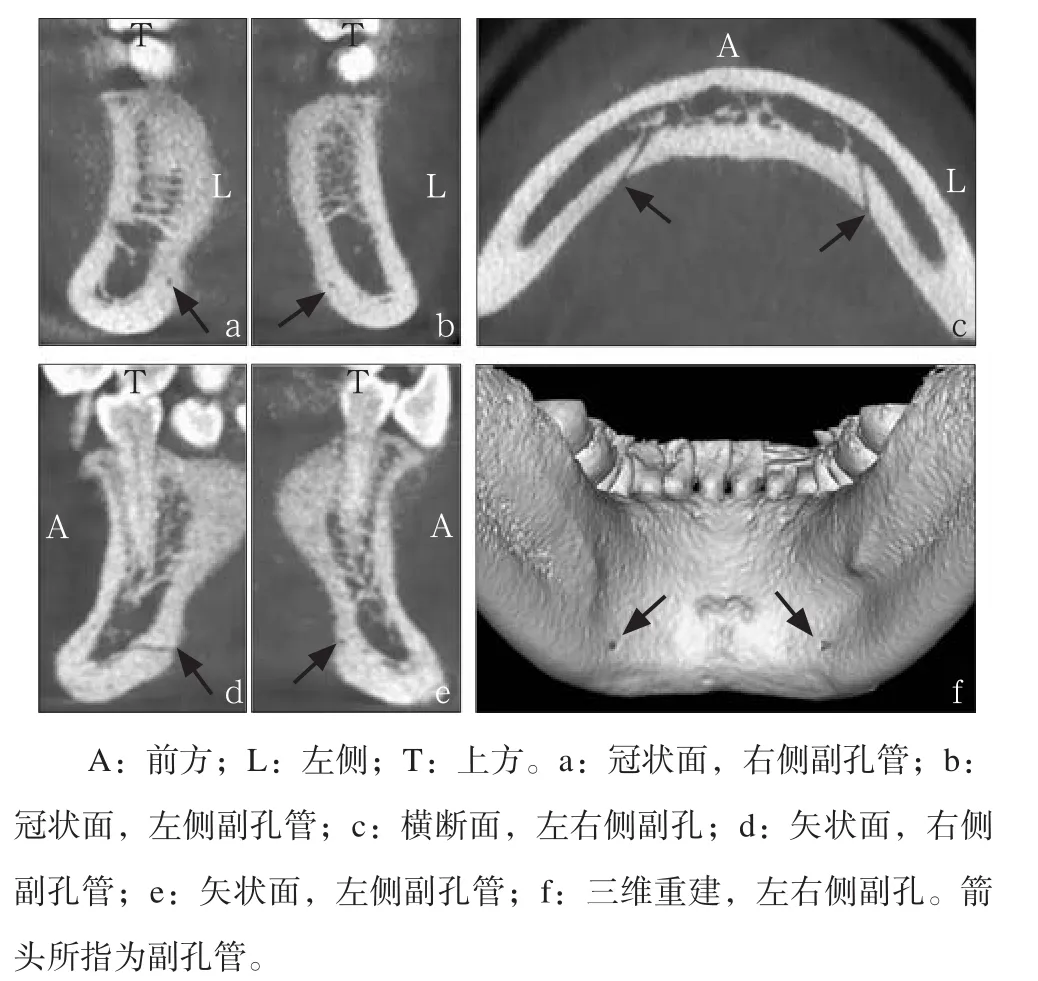
图4 下颌前磨牙区的低位副孔,左右侧各1个 Fig 4 Accessory mandibular foramina in inferior area of lingual premolar, there are one foramen in each left and right sides
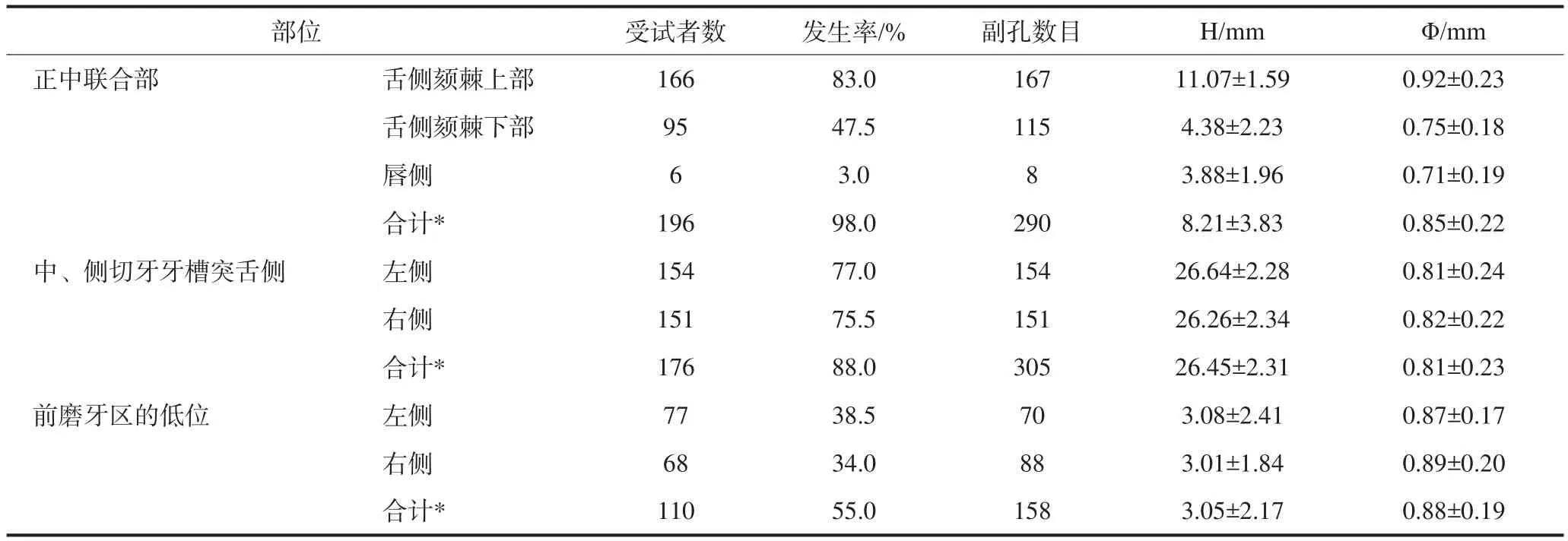
表 4 下颌骨三处副孔高频区的副孔分布情况Tab 4 Distribution of accessory mandibular foramina in the three highest frequency regions
3 讨论
下颌皮质骨表面广泛存在副孔,近年随着口腔颌面部手术数量的上升,术后临床医师偶见诸如颌下出血、唇部感觉异常等问题,使得学者们逐渐开始重视下颌骨副孔的存在及其影响。
本研究中每名受试者的下颌骨体均出现副孔(100%),个体出现副孔的数目1~12不等,人均(5.62±2.10)个。以往文献关于下颌骨副孔的出现率(29.8%~100%)[1-7]和人均副孔数(0.52~3.78个)[1,2,4,7-8]相差较大。日常观片中需看到皮质骨到松质骨的完整管道样低密度影像,才认定为下颌骨副孔。CT部分容积效应的作用下,若副孔真实直径小于2倍设备分辨率,则极易被忽略甚至不可见,如本实验中副孔直径大于0.50 mm才能被观测到。因此高分辨率的CT设备有利于观测到更小直径级别的副孔,提高副孔的检出率和发现率[1,6-7]。颌骨标本直接观测方式则不受此限制,发现下颌骨副孔数量可更多,单个下颌骨可观测到78.7个副孔,发现率达100%[3],但标本常常缺失对应的本人背景信息,从而限制了年龄、性别、病情等因素的分析。
男性和女性的副孔数目无差异(P=0.195),但副孔数目和年龄有关(Plt;0.001),随着年龄的增长,副孔数目呈减少的趋势。推测随着年龄的增长,部分下颌骨副孔管可能出现狭窄甚至闭锁,使副孔数量减少。下颌骨体自近中向远中区域副孔发生率下降(Plt;0.001),舌侧副孔发生率高于颊侧。下颌磨牙区副孔的发生率最低,且副孔位置散在,表明此区副孔并不高发,可认为是种植术相对安全的区域。
通过对副孔所在位置进行分析,发现有3处副孔高频区域:正中联合部,中、侧切牙牙槽突舌侧以及前磨牙区舌侧的低位。
下颌骨正中联合部副孔又被称为正中孔(midline foramina,MLF),以往报道称此处副孔发生率为88.9%~100.0%[2,9],本实验发生率为98.0%。口底解剖发现双侧舌下动脉在正中线上吻合并发出下颌骨穿支经过MLF进入下颌骨内,营养下颌骨前部骨质及牙齿[2]。熟悉MLF的高度位置有利于避免损伤副孔内血管引起出血,国外文献报道MLF平均高度为9.34~11.02 mm[2,7,10],本研究MLF平均高度为(8.21±3.83) mm,小于前者,这可能与国内外人种下颌骨高度差异有关。超声检查舌侧正中管外动脉血管平均直径为1.41 mm,平均血流量为2.92 mL·min-1,若损伤的副孔内血管直径大于1.0 mm,或损伤点与舌侧骨皮质缘水平距离小于1.0 mm[11],则极易引起口底软组织血肿。本实验平均副孔直径为0.85 mm,国外报道称该数值为0.70~0.97 mm[2,7,9,12]。MLF中颏棘上方发生最高(83.0%),其次为颏棘下方(47.5%),唇侧最少(3.0%)。颏棘上方MLF平均高度(11.07±1.59) mm,平均直径(0.92±0.23) mm。因此应留意颏棘上方MLF,避免损伤血管而引起血肿。临床中此区域种植术应保持种植体底与下颌下缘12 mm以上的垂直距离。
下颌中、侧切牙牙槽突舌侧副孔大多数人会出现(88.0%),常呈左右对称性出现(73.3%)。双侧舌下动脉各发出牙槽嵴支从侧切牙区近牙槽嵴顶的位置穿舌侧皮质骨板进入下颌骨内,营养该处牙龈和骨质[9]。下切牙神经可发出分支经过中、侧切牙牙槽突舌侧孔,支配双侧切牙区舌侧牙龈。CBCT图像显示此副孔管始于下颌切牙管,向上竖直走行,开口于平均高度为(26.45±2.31)mm的中、侧切牙牙槽突舌侧,牙槽嵴顶下约6 mm位置,平均直径(0.81±0.23) mm。临床中对此区域操作时应添加局部浸润麻醉并注意手术止血。
颏下动脉或舌下动脉分支形成的下颌舌骨肌动脉[13],营养骨膜,发出穿支经前磨牙区低位皮质骨自后向前走行进入骨内,与下牙槽动脉交通[14]。以往报道此处的副孔发生率为27.5%~39.7%[13,15],而本实验的发生率为55.0%,副孔平均高度为(3.05±2.17) mm,平均直径(0.88±0.19) mm,颌面外科手术应注意此位置以避免不必要的出血。
下颌骨作为动脉终末分支供应器官之一,血液供应呈多源性。下牙槽动脉、舌下动脉和颏下动脉的分支通过副孔的连通在下颌骨骨内形成复杂的微动脉血管网[16]。颌周软组织恶性肿瘤细胞可以依附此管道浸润到骨髓腔,沿下颌管迅速扩散至其他部位甚至全身转移。为了保证肿瘤相连通的副孔血管一并切除,手术切骨边界则应在受累区边缘外2.0~2.5 cm[17]。为了减少舌侧副孔转移侧可能性,牺牲牙槽突和舌侧骨板的下颌骨上缘斜行切除术,此术式不仅切除了已侵犯的舌侧骨板副孔而且保留了颊侧骨板[1],有利于减轻术后患者颌面部的畸形。
[1] Patil S, Matsuda Y, Okano T. Accessory mandibular foramina: a CT study of 300 cases[J]. Surg Radiol Anat, 2013, 35(4):323-330.
[2] Gahleitner A, Hofschneider U, Tepper G, et al. Lingual vascular canals of the mandible: evaluation with dental CT[J]. Radiology, 2001, 220(1):186-189.
[3] 李学雷,张建斌,刘学敏,等. 下颌骨内侧面副孔的观测及其临床意义[J]. 中国临床解剖学杂志, 2002, 20(6):451-453.Li XL, Zhang JB, Liu XM, et al. Measurement of accessory foramina on the medial mandibular surface and its clinical significance[J]. Chin J Clin Anat, 2002, 20(6):451-453.
[4] Scaravilli MS, Mariniello M, Sammartino G. Mandibular lingual vascular canals (MLVC): evaluation on dental CTs of a case series[J]. Eur J Radiol, 2010, 76(2):173-176.
[5] Murlimanju BV, Prakash KG, Samiullah D, et al. Accessory neurovascular foramina on the lingual surface of mandible: incidence, topography, and clinical implications[J]. Indian J Dent Res, 2012, 23(3):433.
[6] Eshak M, Brooks S, Abdel-Wahed N, et al. Cone beam CT evaluation of the presence of anatomic accessory canals in the jaws[J]. Dentomaxillofac Radiol, 2014, 43(4):20130259.
[7] Sekerci AE, Sisman Y, Payveren MA. Evaluation of location and dimensions of mandibular lingual foramina using cone-beam computed tomography[J]. Surg Radiol Anat, 2014, 36(9):857-864.
[8] Sanomiya Ikuta CR, Paes da Silva Ramos Fernandes LM, Poleti ML, et al. Anatomical study of the posterior mandible: lateral lingual foramina in cone beam computed tomography[J]. Implant Dent, 2016, 25(2):247-251.
[9] McDonnell D, Reza Nouri M, Todd ME. The mandibular lingual foramen: a consistent arterial foramen in the middle of the mandible[J]. J Anat, 1994, 184 (Pt 2):363-369.
[10] Babiuc I, Tărlungeanu I, Păuna M. Cone beam computed tomography observations of the lingual foramina and their bony canals in the median region of the mandible[J]. Revue roumaine de morphologie et embryologie, 2011, 52(3):827-829.
[11] Mardinger O, Manor Y, Mijiritsky E, et al. Lingual perimandibular vessels associated with life-threatening bleeding: an anatomic study[J]. Int J Oral Maxillofac Implants, 2007, 22(1):127-131.
[12] Liang X, Jacobs R, Lambrichts I. An assessment on spiral CT scan of the superior and inferior genial spinal foramina and canals[J]. Surg Radiol Anat, 2006, 28(1):98-104.
[13] Katakami K, Mishima A, Kuribayashi A, et al. Anatomical characteristics of the mandibular lingual foramina observed on limited cone-beam CT images[J]. Clin Oral Implants Res, 2009, 20(4):386-390.
[14] Nakajima K, Tagaya A, Otonari-Yamamoto M, et al. Composition of the blood supply in the sublingual and submandibular spaces and its relationship to the lateral lingual foramen of the mandible[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2014, 117(1): e32-e38.
[15] von Arx T, Matter D, Buser D, et al. Evaluation of location and dimensions of lingual foramina using limited cone-beam computed tomography[J]. J Oral Maxillofac Surg, 2011, 69(11):2777-2785.
[16] 廖进民, 王兴海, 李忠华, 等. 下颌骨血供及血管构筑的临床解剖学研究[J]. 中国临床解剖学杂志, 2005, 23(1):27-30.Liao JM, Wang XH, Li ZH, et al. The clinical anatomic study on the blood supplying system and its vessel architecture of the mandible[J]. Chin J Clin Anat, 2005, 23(1):27-30.
[17] 王伯钧, 秦小云, 周思, 等. 下颌骨副孔分布与安全手术切缘的相关性研究[J]. 中国临床解剖学杂志, 2008, 26(4):451-454.Wang BJ, Qin XY, Zhou S, et al. The relationship between accessory foramina on the medial and lateral mandibular surface and surgical margins[J]. Chin J Clin Anat, 2008, 26(4):451-454.
A cone beam computed tomography study on the anatomical position of accessory mandibular foramina in Jiangxi adults
Ke Xing, Li Bohan, Chen Linlin, Jiang Xindi.
(Dept. of Oral and Maxillofacial Surgery, Affiliated Stomatological Hospital of Nanchang University, The Key Laboratory of Oral Biomedicine, Jiangxi Province, Nanchang 330006, China)
Supported by: The Science and Technology Planning Project of Jiangxi Health and Family Planning Commission (20151951);The Key Research and Development Project of Jiangxi Provincial Department of Science and Technology (20161BBG70151).Correspondence: Chen Linlin, E-mail: oral_surgery@sina.com.
Objective This study used cone beam computed tomography (CBCT) to access the distribution and position of accessory mandibular foramina in the mandibular body of Jiangxi adults, and some safety rules of operation for clinics were provided. Methods Two hundred CBCT image subjects of Jiangxi adults were selected, which were divided into 4 groups by age with the same sex ratio. The number and position of accessory mandibular foramina in mandibular anterior teeth, premolars and molars region were described and the relationship between accessory mandibular foramina incidence and factors of age, gender and lateral were analyzed. Results A total of 1 123 accessory mandibular foramina were found, with a mean of 5.62±2.10 per person. The accessory mandibular foramina incidence decreased from the mesial region to the distal, and the lingual was higher than the buccal. There was no significant difference in the number of accessory mandibular foramina in male and female (P=0.195). However, the number of accessory mandibular foramina was negatively correlated with age (rs=-0.301). Three highest frequency regions of accessory mandibular foramina were mandibular symphysis area (98.0%), lingual alveolar area of lower medial (88.0%) and lateral incisors and inferior area of lingual premolar (55.0%). Conclusion Accessory mandibular foramina are widely presented in the body of everyone’s mandible, addition attention should be paid to avoid the complications causing by the damage of canal contents in the clinics.
mandible; accessory mandibular foramen; cone beam computed tomography; mandibular anatomy
R 81
A
10.7518/hxkq.2017.06.009
2017-01-17;
2017-09-08
江西省卫计委科技计划(20151951);江西省科技厅重点研发计划项目(20161BBG70151)
柯星,住院医师,硕士,E-mail:kexindewo@foxmail.com
陈林林,教授,硕士,E-mail:oral_surgery@sina.com
(本文编辑 杜冰)
猜你喜欢
小猕猴智力画刊(2021年6期)2021-08-05
昆明医科大学学报(2021年1期)2021-02-07
民族音乐(2019年6期)2020-01-15
童话世界(2019年35期)2020-01-04
风采童装(2018年1期)2018-04-12
中国民族医药杂志(2016年5期)2016-05-09
作文大王·低年级(2016年3期)2016-03-11
西南医科大学学报(2016年4期)2016-01-03
中国医疗美容(2015年1期)2015-07-12
中国医疗美容(2015年1期)2015-07-12