
Hydrochloric acid enhanced radiofrequency ablation for treatment of large hepatocellular carcinoma in the caudate lobe:Report of three cases
2019-04-16 08:23HanXiaDengJinHuaHuangWanYeeLauFeiAiMinShanChenZhiMeiHuangTianQiZhangMengXuanZuo
World Journal of Clinical Cases 2019年4期
Han-Xia Deng,Jin-Hua Huang,Wan Yee Lau,Fei Ai,Min-Shan Chen,Zhi-Mei Huang,Tian-Qi Zhang,Meng-Xuan Zuo
Abstract
Key words: Hydrochloric acid;Radiofrequency ablation;Hydrochloric acid enhanced radiofrequency ablation;Caudate lobe;Large hepatocellular carcinoma;Case report
INTRODUCTION
Hepatocellular carcinoma(HCC)arising from the caudate lobe is rare[1].The caudate lobe is situated deep between the hepatic hilum and the inferior vena cava.Caudate lobectomy is considered to be technically difficult even for small tumors,with high risks of local recurrence and poor overall survival[2,3].For large tumors in the caudate lobe,resection is challenging even in the hands of experienced liver surgeons[4,5].Interventional therapies,including various intravascular and extravascular procedures,have been reported to treat caudate lobe HCC[6-14].However,most of those focused on treating small HCC(maximum diameter < 5 cm).This is a retrospective study on three patients with HCC ≥ 5 cm in the caudate lobe treated by hydrochloric acid(HCl)enhanced radiofrequency ablation(HRFA).
CASE PRESENTATION
Case 1
A 61-year-old woman was found to have a caudate lobe lesion(55 mm × 57 mm × 63 mm)on magnetic resonance imaging(MRI).The patient had a history of chronic hepatic B virus(HBV)infection,with Child-Pugh A liver function and a negative serum alpha-fetoprotein(AFP)concentration(0.71 ng/mL).A biopsy confirmed HCC.Transarterial chemoembolization(TACE)using an emulsion of tetrahydropalmatine(THP)50 mg,lobaplatin 50 mg,and lipiodol 10 mL was performed in August 2013.One month later,computed tomography(CT)showed that the tumor had enlarged(72 mm × 75 mm × 81 mm),and was separated into the superior and inferior parts by a fibrous septum.
Since the tumor enlarged after TACE,the patient was suggested to undergo ablation therapy.Conventional RFA was insufficient to ablate such a huge tumor.Thus,the patient received two sessions of HRFA in September and December 2013,respectively,to ablate the superior and inferior parts of the tumor.HRFA was applied for 60 min in the first and 30 min in the second session.No discomfort during ablation and no complications such as fever,pain,or hemorrhage after HRFA were observed.
One month after the first HRFA,a peripheral hyper-metabolic nodule was detected by PET-CT.Thus,the patient underwent two more sessions of COOL-TIP RFA in December 2013 and March 2014,respectively.After that,the hypermetabolic lesion was no longer visible.The last follow-up CT in July 2018 showed that the tumor had decreased to an inactive fibrous tissue mass of about 2 cm in diameter.During the course of treatment and follow-up,there were no major complications.A minor complication was asymptomatic slight dilation(total bilirubin concentration once elevated to 72 μmol/L 18 mo after HRFA and returned normal without any treatment)of bile ducts(Figure 1).
Case 2
A 69-year-old man was found on health checkup to have a caudate lobe tumor,17 mm× 25 mm on PET-CT in June 2013.He had a history of chronic HBV infection.The AFP concentration was negative,and he had Child-Pugh A liver function.A biopsy confirmed the diagnosis of HCC.The patient received two sessions of TACE in August and November 2013,respectively.CT performed in March 2014 showed that the lesion had enlarged to 47 mm × 57 mm,with poor lipiodol deposition.Besides,the patient had a history of tongue cancer and received radiotherapy 4 years ago.
In March 2014,HRFA through an anterior approach was applied for 60 min.There was no acute adverse effect occurring in the peri-ablation and post-ablation periods,and an MRI scan one month later showed no areas of enhancement.
Ten months after HRFA,in January 2015,MRI showed the margin of the lesion to be suspiciously enhanced by contrast.He underwent one session of COOL-TIP RFA.No visible active lesion was detected in the next MRI scan.The last MRI scan in December 2015 found no active lesion in the liver.Twenty-four months after HRFA,the patient died of recurrent tongue cancer(Figure 2).
Case 3
A 73-year-old man presented with chest and abdomen pain in February 2016.CT showed a mass in the pancreatic neck and a low density lesion,35 × 50 mm,in the caudate lobe.The patient had a history of chronic HBV infection,Child-Pugh A disease,and a negative serum AFP concentration.The PIVKA level was 20.266 AU/m.An exploratory laparotomy showed a primary tumor in the caudate lobe and that the lesion in pancreatic neck was a spontaneous hematoma.Frozen section analysis of an enlarged portal lymph node showed metastatic HCC.TACE was performed in April 2016,with an emulsion of THP 30 mg,lobaplatin 30 mg,and lipiodol 10 mL.CT after TACE showed good lipiodol deposition.
Three days later,HRFA was applied for 15 min through an anterior approach.No major complications occurred.One month later,the PIVKA concentration dropped to 2.566 AU/mL and no visible contrast enhanced areas on MRI.Follow-up at 28 mo after HRFA showed no signs of relapse or metastasis.(Figure 3)
The summary of the three patients is shown in Table1.
DISCUSSION
Surgical resection of a caudate lobe tumor is technically challenging as the caudate lobe is situated deep between the hepatic hilum and the inferior vena cava[1].In a report on 12 patients,the median operative time was 568 min,the median intraoperative blood loss was 550 mL,and five patients developed postoperative bile leak with problems in renal function[4].Caudate lobectomy is commonly combined with major or extended hepatectomy with sacrifice of a large amount of nontumorous liver parenchyma which increases the risk of postoperative liver failure.
Compared to surgery,interventional therapies such as TACE or RFA have a lower risk of treatment morbidities.In 1986,Takayasuet al[6]reported five patients who underwent transcatheter arterial infusion(TAI)or transcatheter arterial embolization(TAE)for treating advanced-stage caudate lobe HCC.Unfortunately,four of these patients died during a mean of 5.5 mo.With advances in interventional technology and a better understanding of arterial blood supply of caudate lobe HCC[8,15,16],the success rate of selective subsegmental TACE in treating caudate lobe HCC has been greatly improved.However,long-term survival after treatment remains a problem.Kimet al[9]performed selective TACE to treat 34 patients with caudate lobe HCC with a diameter of less than 3 cm.The 5-year overall survival and progression-free rates were 72% and 21%,respectively.TACE cannot completely block the feeding arteries and gain a complete tumor necrosis,which causes recurrence[10].For a large caudate lobe HCC,the results of TACE are even worse.
服务特点:第一个将工程学与应用科学进行融合服务的平台,图书、工具书提供条目和全书付费方式,特色在材料物性、方程式的检索,同时提供强大的表格分析工具。Knovel提供工具供用户对结果进行深入分析。使用超过80,000 种互动表格、图解和公式,具体 1) 客制化并操作数据呈现方式,同时可以轻松的在工作表中排序 2) 直接在图表中绘制一个或多个数据点和曲线;3) 汇出数据到指定的格式和文件 (Excel, MathCAD)。
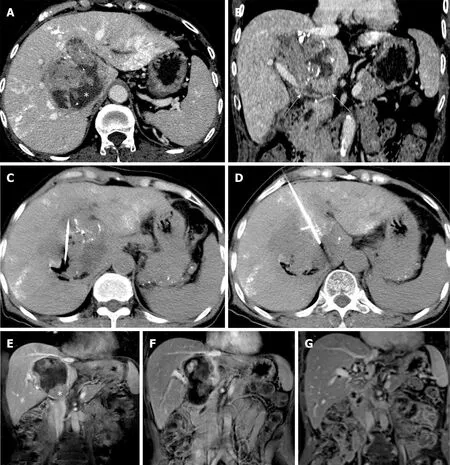
Figure1 Arterial-phase computed tomography images showing a large caudate lobe tumor enhanced after transarterial chemoembolization in a 61-yearold woman with confirmed hepatocellular carcinoma.
Percutaneous ablation therapies,including percutaneous ethanol injection(PEI),RFA,and MWA,are well-established and widely used treatments for HCC.In 2002,Shibataet al[11]first introduced PEI with or without TAE to treat 25 patients with caudate lobe HCC(average diameter,27 mm).Penget al[13]reported on 17 patients who underwent RFA treatment for caudate lobe HCC(average diameter,31 mm).However,most of these studies focused on treating small caudate lobe tumors.Nevertheless,incomplete ablation and recurrence still happened.Nishigakiet al[14]compared the recurrence rates in patients with caudate lobe HCC or HCC located in other liver segments.They found that the caudate lobe patients had a higher risk of developing tumor recurrence.Caudate lobe HCCs are more difficult to be completely ablated than those in other liver segments due to the restricted approach through which an RFA electrode can be introduced,and the heat sink effect of the inferior vena cava.
In the last decade,several new techniques,such as normal saline perfused radiofrequency ablation(NSRFA)and multi-electrode applications had been developed,aiming to create a large ablative zone[17].Our previous experiments showed that infusing diluted HCl instead of normal saline during RFA could enlarge the diameter of ablation zone from a mean(SD)of 3.52 cm(0.07)to 6.85 cm(0.32)at 30 W-30 min[18].This is because the conductivity of HCl is about three times higher than that of saline,greatly increasing the conductivity around the RF electrode[19].Inin vivoexperiments,HRFA also exhibited a larger ablative zone with favorable safety[21-22].Based on these studies,we have reported performing HRFA on a patient with spontaneously ruptured HCC,which successfully controlled bleeding and achieved complete necrosis after ablation without any complications[19].In a word,HRFA,a technique that can create a large ablation volume by using a monopolar electrode,is promising in treating large caudate lobe HCCs.In the present study,all three patients had unresectable large caudate lobe HCC.One patient underwent two sessions of HRFA and the other two patients underwent one session each.After HRFA and followed complementary COOL-TIP RFA,all the three caudate lobe tumors showed complete necrosis.

Figure2 A well-defined active caudate lobe tumor adjacent to the right hepatic vein in a 69-year-old man with a history of tongue cancer after two sessions of TACE.
Among four sessions of HRFA,three were performed through an anterior approach and the remaining one was through a lateral approach(case 1,the 2ndsession)in order to protect peripheral vessels and the biliary system.HRFA also avoids repeated punctures because one session of HRFA is sufficient to achieve complete necrosis.Besides,the electrode in HRFA could be placed at the center of the lesion whereas in other RFA techniques,it must reach the tumor margin,which would induce damage to the structure nearby.There was no major complication and asymptomatic bile duct dilatation as a minor complication occurred in patient 1 18 mo after HRFA.It was hypothesized that the non-active lesion,which had shrunk from 7 cm to less than 3 cm,stretched its peripheral liver tissue and induced bile duct dilatation.
CONCLUSION
HRFA can be an efficacious and safe choice for patients with a large caudate lobe HCC.However,further research is necessary to determine the appropriate role of HRFA in treating caudate lobe HCCs.Combination of HRFA with TACE or other systemic therapies is expected to further improve the prognosis of patients.

Table1 The summary of all three patients

Figure3 Preoperative computed tomography and magnetic resonance imaging images of a 73-year-old male showing a large intrahepatic tumor in the caudate lobe.
猜你喜欢
材料与冶金学报(2022年2期)2022-08-10
作文通讯·高中版(2022年4期)2022-05-10
能源工程(2022年1期)2022-03-29
中华诗词(2019年2期)2019-11-15
中华诗词(2019年1期)2019-08-23
图书馆界(2017年3期)2017-09-13
黑龙江教育·高校研究与评估(2017年6期)2017-06-16
世纪桥(2017年3期)2017-04-24
科技与创新(2015年12期)2015-07-21
黑龙江史志(2013年7期)2013-08-15
 World Journal of Clinical Cases2019年4期
World Journal of Clinical Cases2019年4期
- World Journal of Clinical Cases的其它文章
- Immune checkpoint inhibitor-induced colitis:A comprehensive review
- Formalin fixation on HER-2 and PD-L1 expression in gastric cancer:A pilot analysis using the same surgical specimens with different fixation times
- Nested case-control study of multiple serological indexes and Brighton pediatric early warming score in predicting death of children with sepsis
- Intestinal endometriosis:Diagnostic ambiguities and surgical outcomes
- Efficacy of 1.2 L polyethylene glycol plus ascorbic acid for bowel preparations
- Congenital analbuminemia in a patient affected by hypercholesterolemia:A case report