
Retrospective review of total neoadjuvant therapy
2019-10-23 05:36LailaBabarVeliBakalovStephenAbelObaidAshrafGeneGrantFinleyMosesRajKristinaLundeenDulabhMongaAlexanderKirichenkoRodneyWegner
Laila Babar,Veli Bakalov,Stephen Abel,Obaid Ashraf,Gene Grant Finley,Moses S Raj,Kristina Lundeen,Dulabh K Monga,Alexander V Kirichenko,Rodney E Wegner
Laila Babar,Veli Bakalov,Obaid Ashraf,Department of Internal Medicine,Allegheny General Hospital,Pittsburgh,PA 15212,United States
Stephen Abel,Alexander V Kirichenko,Rodney E Wegner,Department of Radiation Oncology,Allegheny General Hospital,Pittsburgh,PA 15212,United States
Gene Grant Finley,Moses S Raj,Kristina Lundeen,Dulabh K Monga,Department of Medical Oncology,Allegheny General Hospital,Pittsburgh,PA 15212,United States
Abstract
Key words: Total neoadjuvant therapy; Neoadjuvant chemoradiation; Multi-agent chemotherapy; Locally advanced rectal cancer; National cancer database; Colorectal cancer; Retrospective review; Gastrointestinal oncology; Temporal trends; Surgical excision
INTRODUCTION
Over the past several years,there have been several advances in the medical and surgical treatment of locally advanced,stage II and III rectal cancer.With the advent of total mesorectal excision as well as anal laparoscopic surgeries,treatment options continue to improve and result in lower rates of local disease recurrence in these patients.There has also been an ongoing paradigm shift in the approach to chemoradiation administration.The standard of care for rectal cancer is neoadjuvant chemoradiotherapy (nCRT) followed by surgery and then postoperative multiagent chemotherapy based on several randomized trials[1,2].A novel approach called total neoadjuvant therapy (TNT) has recently gained favor whereby patients are given both nCRT as well as multiagent chemotherapy prior to surgery.TNT use has been associated with better compliance,decrease in toxicities,and higher rates of anal sphincter preservation[3-9].
This change in approach has been based on increasing evidence that there is better quality of life with improved functionality,decreased toxicity,and lower rates of recurrence with preoperative treatment[4-9].Patients receiving adjuvant chemotherapy have delays in the administration of treatment secondary to long postoperative recovery time and inability to regain their prior functional status.Compliance is an issue in these patients,and they often do not receive their scheduled chemotherapy or it is delayed[3].Additionally,with the use of TNT,carefully selected patients who have a clinical complete response can in some instances avoid surgery altogether and instead be followed with close observation (i.e.“watch and wait approach”)[10].
With local disease recurrence rates falling due to the use of total mesorectal excision,which is a close dissection of the rectum and para rectal lymph nodes within the mesorectal envelope[11],there is still an increased concern for distant metastases.Over 35% of patients treated with the standard therapy for locally advanced rectal cancer (LARC) have distant recurrence of disease[12].One reason for this is the presence of micrometastases.As surgery only addresses local disease and potentially delays the administration of chemotherapy,these micrometastases can result in distant metastasis.The administration of TNT helps tackle this problem by providing total systemic treatment prior to surgical resection.It also gives clinicians the ability to detect patients who do not respond to the treatment in a timely manner[13].
As such,we queried the National Cancer Database (NCDB) to analyze the trends in treatment approach towards locally advanced rectal carcinoma and to determine if there has been a rise in TNT use in recent years.Additionally,we identified the factors affecting the rate of utilization of TNT and how they correlate with patients from different socioeconomic strata.
MATERIALS AND METHODS
The aim of this study was to use the NCDB to evaluate the trends in treatment options for LARC,specifically with regards to TNT utilization.The NCDB is a national database cataloguing approximately 70% of all cancer cases within the United States[14].This information is collected from over 1500 cancer treatment centers.This database details information about patients’ demographics,disease,treatment,and mutations for several cancer subtypes.The data that are submitted to this database must meet established quality standards and is managed by the Commission on Cancer of the American College of Surgeons and the American Cancer Society.We used data extracted from a de-identified NCDB record.This study was exempt from review by the internal revenue board due to its deidentified and retrospective nature.
We queried the NCDB for patients diagnosed with rectal adenocarcinoma diagnosed between 2004 and 2014.Patients with stage II and III cancer were included and the data were analyzed to extract if the treatment modality was TNT or multiagent chemotherapy (maChT).TNT entails the administration of induction chemotherapy as well as chemoradiotherapy prior to surgery,while maChT is postoperative multiagent chemotherapy,which is given in the adjuvant setting and is the current standard of care,and is often combined with neoadjuvant chemoradiation preop[1].All patients who did not meet the inclusion criteria were excluded,leaving a total of 9066 patients (Figure1).We analyzed the patient demographics,clinical course,treatment modalities,and survival outcome among our patient population.The patient characteristics used for analysis were age,gender,insurance status,income,facility location and type,tumor stage,treatment modality,and nodal stage.
建立和完善高校政府采购内部控制管理制度,加强内部审计监督和管理制度,努力解决高校政府采购内部控制管理中存在的预算和采购方面的诸多问题,对提高我国高校政府采购内部控制具有重大的影响。
Overall survival (OS) was calculated using the date of diagnosis and the last contact or death.This data were then analyzed using Kaplan-Meier curves for cumulative probability of survival.Log rank statistics were employed to assess for statistical significance between the two groups.Multivariate cox regression was used to identify factors associated with OS.ThePvalue was set at < 0.005.
Multivariable cox regression was done for OS considering the treatment,stage,facility type,location,education status,age,gender,insurance type,race,comorbidity score,mean household income,age distribution,and year of diagnosis.The odds ratios (ORs) for the two groups,those who underwent TNT and those were treated with conventional neoadjuvant treatment,were reported with a 95% confidence interval (CI) along with the corresponding type 1 error (P-value).To account for any potential biases within the two treatment arms,propensity score analysis was used.
RESULTS
Using the eligibility criteria defined above,our final study population consisted of 9066 patients [5648 men (62%),3418 women (38%)].These patients were separated on the basis of the treatment they received:8812 patients received nCRT and 254 patients received TNT from 2004 to 2015.Of the cohort,3694 patients had stage II disease and 5372 had stage III disease with 2525 patients having > 1 node positive (Figure1).The majority of patients were less than age 65 and had private payer insurance.A summary of the clinical and demographics of our study population are in Table1.
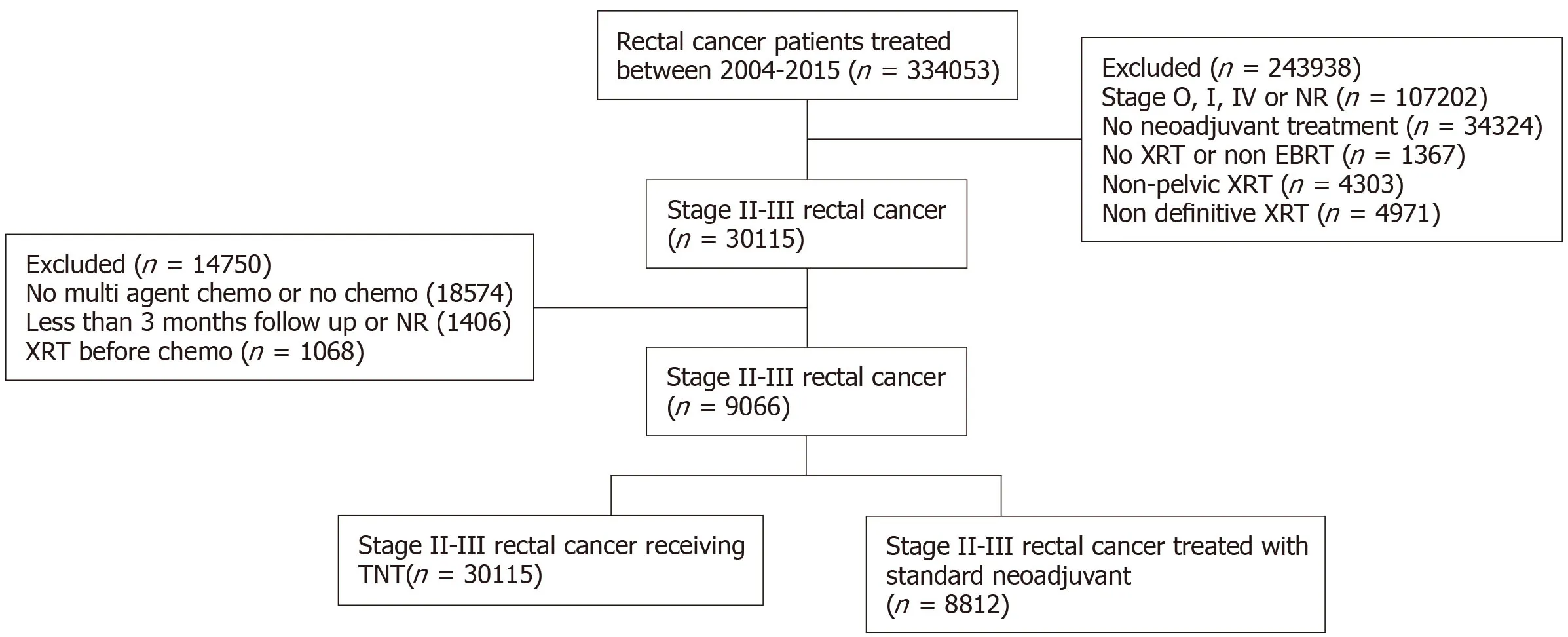
Figure1 Flow chart for filtering data.
There was greater use of TNT with more advanced stage,specifically > 1 node involved (OR = 2.88,95%CI:2.11-3.93,P< 0.01) and stage III disease (OR = 2.88,95%CI:2.11-3.93,P< 0.01).From 2010 to 2012,the use of TNT increased (OR = 2.41,95%CI:1.27-4.56,P< 0.01) with a greater increase from 2013 to 2015 (OR = 6.62,95%CI:3.57-12.25,P< 0.01) (Table1).The 5-year survival for both treatment arms was similar at 76% and 78%,respectively.Multivariable analysis found age > 58,higher income,urban location,academic treatment facility,and lower co-morbidity score as predictors for worse OS.Propensity score matching demonstrated increased age,higher comorbidity score,higher tumor grade,African American race,and gender as predictive of worse OS.
DISCUSSION
Colorectal cancer is the fourth highest occurring cancer in the United States and is the second leading cause of cancer-related deaths as per the Surveillance,Epidemiology,and End Results data[15].Patients with locally advanced rectal carcinoma,which includes patients with T2 or T3 disease with or without nodal involvement,benefit from a multidisciplinary treatment approach.These patients are treated with multiagent chemotherapy,radiation,and surgery to decrease the incidence of local and systemic recurrence.The German Rectal Cancer Study compared neoadjuvant and adjuvant chemotherapy and found improved outcomes with neoadjuvant chemotherapy[1].This can be done in the form of a long course of chemoradiotherapy,a short course radiotherapy or TNT.
When TNT adjuvant chemotherapy is moved to the neoadjuvant setting and given preoperatively,it improves compliance,decreases treatment-associated toxicity,and results in tumor down staging leading to better sphincter preservation[16,17].Randomized clinical trials have demonstrated that there is no benefit to adjuvant chemotherapy in LARC and its use does not improve outcomes in patients with stage II and III disease who receive chemoradiation in the neoadjuvant setting[7-9].The EORTC 22921 trial was conducted to evaluate the utility of adjuvant chemotherapy in patients with T3-T4 tumors,and it found that there was no additional benefit of giving adjuvant chemotherapy to patients who had been treated with neoadjuvant chemoradiation[6].Patients who underwent adjuvant chemotherapy showed poor compliance with only 43%-73.6% of them receiving the planned doses and an overall delay of over 18 wk in receiving systemic therapy[3].They also had higher incidence of chemotherapy related toxicity and poor surgical outcomes[4-9].Prior studies have shown that over 10%-25% of patients receiving neoadjuvant chemotherapy have complete pathological response,which is an established predictor of improved survival[18-23](Table2).
In light of these findings,the use of alternate treatment strategies such as TNT is gaining favor and its use is becoming increasingly common.Our data showed an increase in recent years in the use of TNT,which coincided with the initiation of several clinical trials evaluating the outcomes of using TNT over traditional CRT.The number of patients treated with TNT was small in our dataset,however,this was to be expected as it was compiled over 10 years from 2004 to 2015,and TNT use is a rather recent phenomenon.Our data showed a rising trend in TNT use,with patients diagnosed from 2013 to 2015 having the highest frequency of use.We expect this use to further increase as more data about benefits of TNT over traditional treatment comes to light.
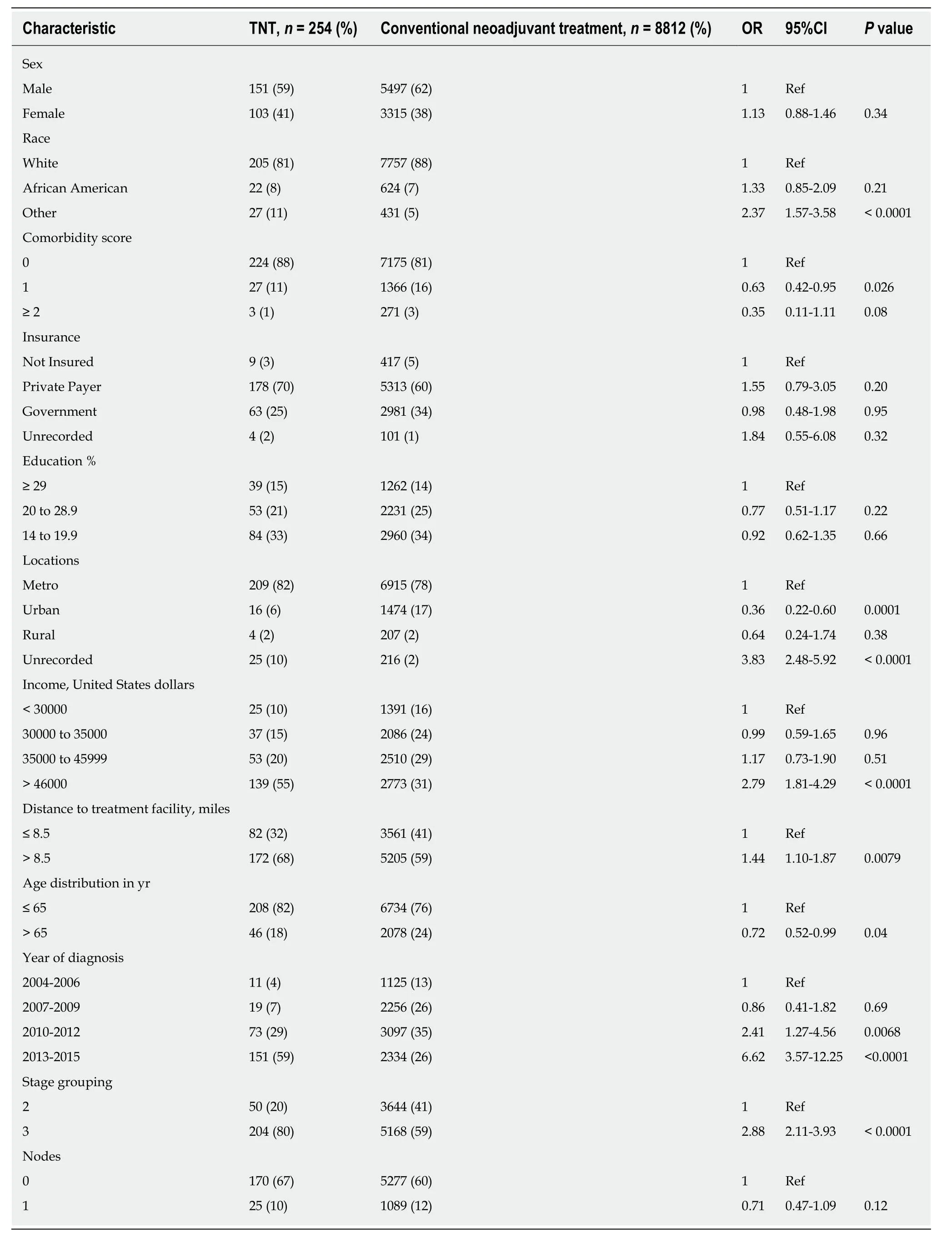
Table1 Comparative use of total neoadjuvant treatment vs conventional neoadjuvant treatment approach by baseline characteristics in patients receiving treatment for rectal adenocarcinoma
Our study was a large analysis of multi-institutional data to compare the use of conventional chemoradiation with TNT.Due to the large sample size in this database,we were afforded the statistical power to conduct retrospective analyses of different treatment strategies.Our analysis of the NCDB database showed that there has been an increase in TNT use and this trend has been increasing in recent years.This trend was most apparent in patients with stage III disease (Figure2).

Table2 Different surgery/chemoradiation protocols used per standard guidelines
The total number of patients who received TNT is comparatively much lower than the number of patients undergoing CRT,which was a possible limitation of our study.However as prospective data matures,we will see a greater number of patients being treated with TNT.There were limitations to our study,as the data collected by NCDB is retrospective; thus selection biases certainly existed.To counteract this possible bias,propensity score adjustment was performed.Second,as NCDB is coded,there is potential for incomplete coded or miscoded variables,which may have impacted our results and some statistics.One such variable is the incidence of colorectal cancer divided by gender.Per the Surveillance,Epidemiology,and End Results data,men have a slightly increased lifetime risk of developing colorectal cancer (4.5%) compared to women (4.15%).This difference in risk may explain why as per the NCDB database,roughly 60% of our population was male compared to approximately 40% women.It is imperative to note that although the NCDB accounts for cancer treatment all over the United States,only about 70% of the patients treated for cancer are entered into the database; this may also explain why our population had a higher percentage of male patients.
In conclusion,this study was significant,despite its limitations,as it was a largescale analysis of treatment selection for more than 70% of patients diagnosed with rectal cancer from 2004 to 2015 in the United States.It showed an increase in the use of TNT,concordant with current research demonstrating its benefits over the use of conventional neoadjuvant chemoradiation.The rate of use of TNT has been steadily increasing and is most prevalent in patients diagnosed with LARC in recent years.As clinical trials studying the use of TNT near completion,the benefits of this approach are becoming more widely accepted and the use of TNT is increasing.
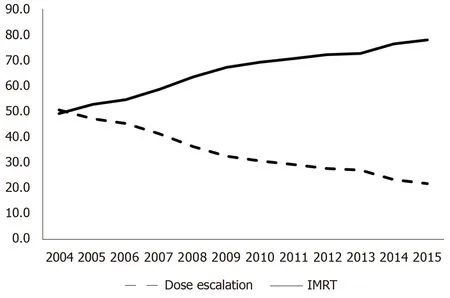
Figure2 Line graph comparing use of total neoadjuvant therapy and neoadjuvant radiation from 2004 to 2014.
ARTICLE HIGHLIGHTS
Research background
Locally advanced rectal cancer (LARC) treatment has been evolving for several years,specifically to improve standard of living after treatment.Total neoadjuvant treatment (TNT) has been gaining favor in recent years as it allows for better sphincter preservation and an overall improved quality of life.Our study analyzes the use of TNT over a 10-year period and compares the overall survival (OS) to that of patients treated with traditional neoadjuvant chemoradiation.
Research motivation
The focus of our study was to evaluate the OS in patients with LARC when treated with either TNT or traditional chemoradiation.It compared the two modes of treatment,which will help clinicians decide between the two modalities.It also sets up the stage for ongoing and future clinical trials that aim to study the benefit of using one modality over the other.
Research objectives
The main objective of our research was to analyze differences in OS in patients treated with TNT or traditional chemoradiation.We did not find a statistically significant difference in OS between the two modalities.An equivocal OS allows researchers to further design clinical trials comparing both treatment options prospectively and establish stronger guidelines that will further help clinicians decide what treatment will benefit their patients most.
Research methods
This was a retrospective review of data extracted from the national cancer database.We queried the National Cancer Data Base to find patients with LARC,stages II and III,who were treated with either TNT or traditional chemoradiotherapy.The standard of care,currently,utilizes a combination of adjuvant chemoradiation and surgery,followed by postoperative multi-agent chemotherapy.We analyzed the differences in OS between the two arms as our primary goal.For our secondary goal,we established what patient characteristics were likely to be associated with TNT use.These characteristics included age,race,gender and comorbidity score.
Research results
Using univariate and multivariate cox regressions,we analyzed our data for both primary and secondary goals.There was no statistically significant difference in OS between the two arms.We also found that patients with stage III disease,higher nodal involvement or treatment within recent years were more likely to have been treated with TNT.Patients in both arms had poor OS with higher comorbidity score,older age,African American race and female gender.Our results further solidify the theory that TNT is non inferior to traditional chemoradiotherapy,and thus must be studied in more detail with prospective trials.
Research conclusions
OS is similar in patients treated with either TNT or traditional chemoradiation.TNT has been associated with better quality of life.As OS is similar to that of neoadjuvant chemoradiation,using TNT may be preferable,to allow for a better standard of living.The 5-year OS is similar for both TNT and traditional chemoradiation.First,in patients with LARC,TNT and neoadjuvant chemoradiation have similar rates of OS.Second,TNT use may be linked to a better quality of life however more studies are needed in this area.There were no new methods as this was a retrospective review of a national database.There was no new phenomenon found as this was a retrospective analysis of an existing database.We queried the database to establish differences in OS for patients treated with two different chemoradiation protocols.Our retrospective analysis showed that the rate of OS was equivocal in patients treated with either TNT or traditional chemoradiation.It will allow clinicians and researchers to further compare the two modalities and may increase the treatment options available to patients suffering from LARC.
Research perspectives
New techniques that allow for radiation treatment to be completed prior to surgery,such as TNT,have yielded non- inferior results and therefore must be studied in greater detail.Future research should aim to conduct prospective clinical trials comparing TNT to traditional chemoradiation.This will help clinicians better decide what treatment is best suited to their patient population.Clinical trials exploring the survival,quality of life and toxicities associated with both TNT and neoadjuvant chemoradiation will help further the research in this field and provide concrete answers to many of the questions raised.
猜你喜欢
艺术生活-福州大学厦门工艺美术学院学报(2022年1期)2022-08-31
大众投资指南(2021年23期)2021-12-06
人大建设(2020年4期)2020-09-21
大众投资指南(2020年10期)2020-07-24
支部建设(2019年36期)2019-02-20
人大建设(2017年2期)2017-07-21
人大建设(2017年9期)2017-02-03
专用汽车(2016年1期)2016-03-01
浙江人大(2014年6期)2014-03-20
浙江人大(2014年4期)2014-03-20
 World Journal of Gastrointestinal Oncology2019年10期
World Journal of Gastrointestinal Oncology2019年10期
- World Journal of Gastrointestinal Oncology的其它文章
- Acylcarnitine:Useful biomarker for early diagnosis of hepatocellular carcinoma in non-steatohepatitis patients
- Evaluation of the safety and effectiveness of direct oral anticoagulants and low molecular weight heparin in gastrointestinal cancer-associated venous thromboembolism
- MicroRNA-320a suppresses tumor progression by targeting PBX3 in gastric cancer and is downregulated by DNA methylation
- Targeted agents for second-line treatment of advanced hepatocellular carcinoma
- Gastric submucosa-invasive carcinoma associated with Epstein-Barr virus and endoscopic submucosal dissection:A case report
- Abnormally expressed circular RNAs as novel non-invasive biomarkers for hepatocellular carcinoma:A meta-analysis