
Physical activity and the prevention of chronic illness in the BRICS nations:Issues relating to gender equality
2019-11-21 01:18GregoreMielkeWendyBrown
Gregore I.Mielke,Wendy J.Brown*
Centre for Research on Exercise,Physical Activity and Health,School of Human Movement and Nutrition Sciences,The University of Queensland,Brisbane,QLD 4072,Australia Received 10 July 2019;revised 20 July 2019;accepted 21 July 2019 Available online 9 August 2019
1.Background
BRICS is an acronym for an international association of 5 countries(Brazil,Russia,India,China,and South Africa),which together represent the world's major emerging economies and almost one-half of the world's population.1,2In these countries,infectious diseases and injuries still account for much of the health burden,but 71%of all deaths are attributable to noncommunicable diseases(NCDs).1Deaths from NCDs are highest in Russia and China(both 86%)and lowest in South Africa(43%),which has the highest proportion of infectious diseases(Table 1).
Physical inactivity(defined as not meeting the lower end of the range of physical activity(PA)recommended for health benefit by the World Health Organization(WHO)3and by current U.S.4and Australian5guidelines(150 min of at least moderate-intensity activity per week,or 75 min of vigorous-intensity activity,or an equivalent combination,per week),is a modifiable risk factor for many of the NCDs that are highly prevalent in the BRICS countries,including cardiovascular diseases,type 2 diabetes,certain cancers,and mental health problems.Data from the WHO Global Health Observatory suggest that between 9%(Russia)and 47%(South Africa)of the adult populations of the BRICS nations do not meet current PA guidelines.6,7This heterogeneity means that up to 14%of all deaths in the BRICS countries are attributable to physical inactivity(Table 1).
2.PA in the BRICS nations
Estimates of PA levels in the BRICS nations(Table 1)are based on activities carried out in the occupational,domestic,transport,and leisure domains.Trends in domain-specific time use and energy expenditure over the past 20 years in Brazil,Russia,China,and India8,9show that the major contributions to overall activity estimates are from occupational and domestic activity.There have been marked decreases in activity in these 2 domains,particularly in China and Brazil.8Indeed,in China the average energy expended in occupational activity halved in the 15 years from 1991 to 2006.8Because all these countries are experiencing rapid economic and technological changes,occupational activity,which we estimate accounted at the turn of the century for about 65%of China's total activity,74%of Brazil's,and 84%of India's,is likely to continue to decline.8With time spent in domestic and transport activity projected to remain stable,it is time to advocate for higher levels of leisure time activity in the BRICS countries.However,with increased urbanization and more people working in sedentary high-tech or manufacturing industries,it is unlikely that even marked improvements in leisure-time activity will offset the energy losses from decreases in occupational activity.
3.Gender differences in PA
Economic and technological changes in the BRICS nations are likely to have significant effects on women's PA levels.At present,considering PA across all domains,men are more active than women in all the BRICS countries,except Russia,where levels of activity are slightly higher among women than among men.7However,when only leisure-time activity is considered,these gender differences are more marked,because women in the BRICS countries still spend much more time in domestic activities and have fewer opportunities for leisure activities than do men.As more women enter the paid workforce,especially if they move into sedentary occupations,they will become much more reliant on leisure-time activity for health benefits.
The recent Global Action Plan on Physical Activity(2018-2030)has set a target of a 10%reduction in physical inactivity levels by 2025 in all countries.3In 2016,we advocated that addressing the gender gap in PA could be a feasible way of achieving this WHO target.7,10Using data from 142 countries,we estimated that an overall improvement of 4.8%points in the median level of physical inactivity among women could achieve this 10%reduction overall,without changingthe distribution in men.7However,in some of the BRICS countries,where girls and women may have fewer opportunities for participation in leisure-time PA,achieving equity could be a major challenge.
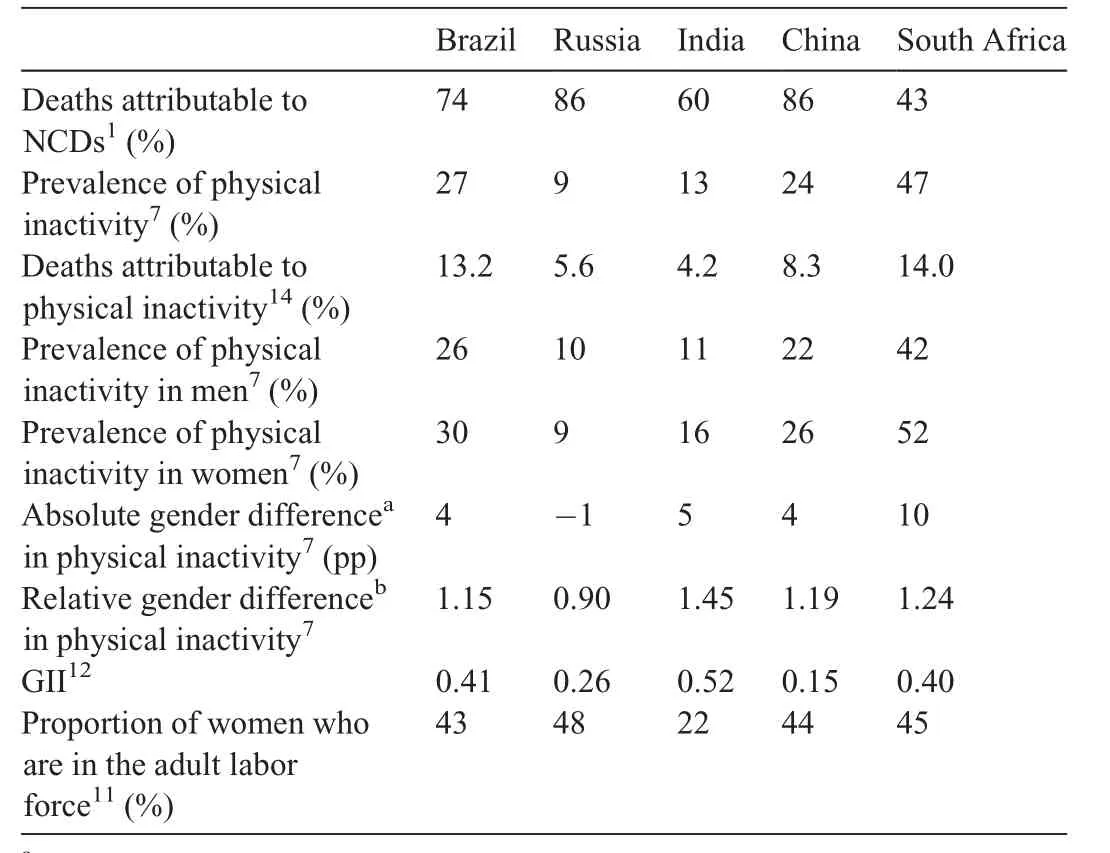
Table 1 Deaths due to NCDs and indicators related to physical inactivity in the BRICS countries.
For example,in India,where levels of inactivity are low,women are 45%more likely than men to not achieve the current recommendations for PA(relative gender difference in physical inactivity of 1.45).At present,only 22%of women in India are in the adult labor force11(Table 1).With increasing economic development in India,more women will move into paid employment,and inactivity levels are sure to increase,reflecting the sedentary nature of work,as well as barriers to safe,affordable,and accessible PA options.Similarly,in South Africa,where communicable diseases still cause more than one-quarter of deaths,1the prevalence of inactivity is high,with a 10%point gender gap7(Table 1).It is difficult to see how this gender gap will be addressed without considerable political will and policy change relating to women's participation in leisure-time PA.
The marked gender differences in PA in 4 of the 5 BRICS nations(Table 1)largely reflect the overall gender inequalities in these countries,as indicated by the UN Development Programme's Gender Inequality Index(GII).12The GII was developed to better depict differences in the distribution of achievements in women and men;the higher the GII value,the more disparities between women and men.Of the BRICS nations,India has the highest GII and is also the BRICS country with the highest relative gender difference in inactivity prevalence(Table 1).
Those leading the efforts to increase population levels of PA in the BRICS countries should consider the facts that both PA and health are underpinned by social factors,that individual behaviors are strongly modelled by society's values and structures,and that inequities will always exist if we remain ignorant of their significance.13Therefore,a first step to closing the gender gap would include an equity agenda that(1)recognizes the needs of groups who systematically face social disadvantage and(2)considers allocation of budgets for both PA promotion and for research to improve our understanding of gender disparities in PA.The bottom line is that we need to empower women and create opportunities for them to be more physically active,especially during their leisure time.Intervention strategies that focus on individual factors(e.g.,motivation),social factors(providing opportunities and support),and environmental factors(e.g.,facilitating access to safe places to be active)will be required to successfully close the gender gap in PA and thereby decrease the proportion of NCD deaths attributable to physical inactivity.
Competing interests
Both authors declare that they have no competing interests.
 Journal of Sport and Health Science2019年6期
Journal of Sport and Health Science2019年6期
- Journal of Sport and Health Science的其它文章
- The impact of health expenditures on public health in BRICS nations
- If you are physically fit,you will live a longer and healthier life:An interview with Dr.Steven N.Blair
- Variability:Human nature and its impact on measurement and statistical analysis
- Differences in transportation and leisure physical activity by neighborhood design controlling for residential choice
- Gender differences in nonlinear motor performance following concussion
- Age-related changes in proprioception of the ankle complex across the lifespan