
Progress of intravoxel incoherent motion diffusion-weighted imaging in liver diseases
2020-09-10 02:57YunYunTaoYiZhouRanWangXueQinGongJingZhengCuiYangLinYangXiaoMingZhang
World Journal of Clinical Cases 2020年15期
Yun-Yun Tao, Yi Zhou, Ran Wang, Xue-Qin Gong, Jing Zheng, Cui Yang, Lin Yang, Xiao-Ming Zhang
Yun-Yun Tao, Yi Zhou, Ran Wang, Xue-Qin Gong, Jing Zheng, Cui Yang, Lin Yang, Xiao-Ming Zhang, Sichuan Key Laboratory of Medical Imaging, Department of Radiology and Medical Research Center of Affiliated Hospital of North Sichuan Medical College, Nanchong 637000,Sichuan Province, China
Abstract
Key words:Magnetic resonance imaging;Diffusion magnetic resonance imaging;Liver diseases;Liver cirrhosis;Carcinoma;Cholangiocarcinoma
INTRODUCTION
Magnetic resonance diffusion-weighted imaging (MR-DWI) uses a single exponential model to obtain the apparent diffusion coefficient (ADC) to quantitatively reflect the diffusion motion of water molecules in tissues[1].However, voxels also contain diffusion information other than the diffusion motion of pure water molecules,namely, the microcirculatory perfusion of the capillary network in tissues[1-4].The ADC values obtained by traditional DWI contain two types of information:Water molecule diffusion and microcirculatory perfusion.The intravoxel incoherent motion (IVIM)-DWI theory was initially proposed by Le Bihanet al[4,5]in the 1980s;IVIM-DWI can obtain quantitative information on pure water molecule diffusion and microcirculatory perfusion-related diffusion and thus compensate for the shortcomings of traditional DWI.This modality can also more accurately and truly reflect the characteristics of tissue structure and pathological changes.Since 1999, when Yamadaet al[6]for the first time applied IVIM-DWI technology to the liver, the research on liver IVIM-DWI has gradually increased and has made great progress.This study reviews the basic principles of IVIM-DWI and related research progress in the diagnosis and treatment of hepatic diseases.
BASIC PRINCIPLES OF IVIM-DWI
IVIM-DWI originated from diffusion-weighted magnetic resonance imaging (MRI).MR-DWI can noninvasively detect the diffusion motion of water molecules (water molecules in fluid exhibit microscopic erratic random movement, known as Brownian motion), which reflects the biological characteristics of the tissue.When the signal derives from biological tissues, some factors attenuate the diffusion motion according to different diffusion coefficients, representing the ADC, which is the sum of the contributions of all motion-related diffusion coefficients.The MR signal can be expressed by a single exponential equation:
Sb/S0=exp(-b×ADC).
Where b is the diffusion-sensitive gradient with a unit of s/mm2;Sb represents the signal obtained at a particular b value;and S0 represents a signal that does not apply a diffusion gradient[7].
IVIM-DWI uses multiple b values and a double-exponential model for image acquisition and analysis, and simultaneously obtains information regarding pure water molecular diffusion and microcirculatory perfusion-related diffusion.IVIMDWI measures perfusion based on the following assumption:The effects of incoherent motion and blood movement can be separated from other incoherent effects.The IVIM-DWI model assumes that other sources of incoherent signals (water exchange between blood and tissue) are negligible compared with blood flow.In the IVIM-DWI model, the relationship between the degree of local signal attenuation in the tissue and the b value can be expressed by the following formula[8]:
Sb/S0=(1-f) ×exp(-b×D) +f×exp(-b×D*).
Where D is the simple diffusion coefficient, also known as slow the apparent diffusion coefficient (Dslow), which reflects the diffusion motion of pure water molecules in the tissue of interest;D* is the pseudo-diffusion coefficient, also known as the fast apparent diffusion coefficient (Dfast), which reflects the microcirculatory perfusion in the capillary network in the area of interest;and f is the fraction of the fast apparent diffusion coefficient, which represents the volume ratio of the correlation effect of the local microcirculatory perfusion to the total diffusion effect and can be used to determine the blood volume in the area of interest.According to the formula,since D* is obviously higher than D, the information obtained from a low b value (<200 s/mm2) mainly reflects the microcirculatory perfusion effect, while the signal attenuation obtained by a high b value (≥ 200 s/mm2) mainly reflects the diffusion effect[5,9].Some researchers[10]believe that f × D* should be used as a new cyclic parameter and that its potential pathophysiological effects should be further elaborated in future studies.
Multiple b values are required for IVIM-DWI to separate tissue diffusion information from perfusion information.Theoretically, more b values correspond to a more accurate data fit and thus better image quality.However, a longerdata collection time corresponds to more clinical application limitations.The number of b values used in published studies ranges from 4 to16, with many studies using approximately 10 b values[6,9,11,12].In terms of the distribution of b values, Cohenet al[13]studied the influence of low b values on D* and showed that at least two b values below 50 s/mm2are required to ensure that D* is not underestimated.Kohet al[14]proposed selecting fewer high b values and more low b values to focus data collection on the sensitive range of perfusion.At present, no consensus on the choice of b values is available, and optimization research on the number and distribution of b values is ongoing[11,15-17].For clinical research, the choice of b values should be based on the different tissues tested and the purpose of the evaluation.The factors influencing the measurement results of IVIM-DWI are complex.In addition to b values, scanner and field intensities[11], the diffusion gradient and respiratory mode[18,19], the DWI sequence[20,21], other physiological activities (such as glandular secretions and fluid flow in glandular canals)[22], motion artefacts, fitting technology and region of interest (ROI) settings[23-28]can all affect the IVIM-DWI image quality and repeatability of the data.These should also be considered in the clinical study design.
NONALCOHOLIC FATTY LIVER DISEASE
In recent years, the prevalence of fatty liver disease in China has gradually increased,and the onset of the disease is trending to involve youngerpatients.Approximately 20% of noninvasive nonalcoholic fatty liver disease (NAFLD) casesdevelop into nonalcoholic steatohepatitis, which can progress to hepatic fibrosis or even cirrhosis[29].Studies have shown that[30-33]the histological characteristics of nonalcoholic hepatic steatosis significantly affect the IVIM-DWI parameters.Parenteet al[31]used IVIM-DWI to study type II diabetic patients with or without NAFLD and found that both the D value and D* value of fatty livers were significantly lower than those of non-fatty livers.The decrease in the D* value reflects the decrease in hepatic perfusion caused by hepatic steatosis, whereas the decrease in the D value may be caused by hepatocytomegaly, the deposition of intracellular fat and the simultaneous restriction of water molecule diffusion intracellularly and extracellularly[33].The study by Jooet al[34]showed that the f value of NAFLD livers was significantly lower than that of normal livers, and this f value is associated with the severity of NAFLD.
HEPATIC FIBROSIS
Although percutaneous liver biopsy can determine the severity of hepatic fibrosis, this test is invasive, and its clinical application is limited.IVIM-DWI has important value in the evaluation of hepatic fibrosis[9,12,19,35-47].
Studies[12,44,45]have shown that the D, D* and f values of hepatic fibrosis patients were significantly lower than those in normal control groups.The IVIM-DWI parameters D, D* and f can be used to distinguish healthy people from patients with hepatic fibrosis, with the f value exhibiting the best diagnostic value[38].The study by Shiragaet al[36]showed that IVIM-DWI also identified a pre-fibrotic state of the liver in Fontan patients.The study included five consecutive Fontan patients and four agematched healthy volunteers.The results showed that in the five Fontan patients,laboratory tests and ultrasound showed almost normal liver conditions, and cardiac catheterization and MRI showed good Fontan circulation, but the D, D* and f values of Fontan patients were significantly lower than those of the control group.However,some studies[9,41,46]have shown that the D value was not significantly different between normal liver tissue and hepatic fibrosis tissue.Dyvorneet al[19]showed that D* values were not significantly different between normal volunteers and patients with hepatic fibrosis.
In addition, many studies have focused on the use of IVIM-DWI technology to determine the severity of hepatic fibrosis, but the conclusions are not completely consistent[12,37-45,47].Huet al[40,45]showed that IVIM-DWI-related parameters were negatively correlated with hepatic fibrosis stages, with the D, D* and f value decreasing with increases in the severity of hepatic fibrosis.Chenet al[45]used IVIMDWI to scan 25 patients with hepatic fibrosis and 25 healthy volunteers.The results showed that the ADC, D, D* and f values in the hepatic cirrhosis group were significantly lower than those in the control group.Additionally, significant differences were found in the parameters of hepatic fibrosis stages (the F0-1 group and F2-4 group and theF0-2 group and F3-4 group).However, further studies have shown that some parameters are not correlated with the hepatic fibrosis stage[37-39,41-44].For example, Chunget al[41-44]showed that a higher stage of hepatic fibrosis corresponded to lower D* and f values;however, no correlation was found between the D values and the stages of hepatic fibrosis.On the other hand, Huet al[39]observed a difference only in the D* values in different fibrosis groups.Other studies[48-51]have shown that IVIMDWI is not sufficient for staging hepatic fibrosis (Table 1).The different D and D*values in the same disease of the previous studies maybe due to the following reasons:(1) The number of patients with each stage of disease was different;(2) The number of b values or an uneven b value distribution may limit the fitting precision;(3) D* has high uncertainty and poor reproducibility;and (4) D values were influenced by steatosis and iron overload[19,45,50].
In summary, the IVIM-DWI parameters of hepatic fibrosis tissues show a decreasing trend compared with those of normal hepatic tissues, and IVIM-DWI can be used for the diagnosis of hepatic fibrosis;however, the value of applying IVIM-DWI for hepatic fibrosis staging still requires further exploration.
DIFFERENTIATION OF BENIGN AND MALIGNANT HEPATIC TUMORS
A large number of studies have discussed the application of IVIM-DWI in the diagnosis of hepatic tumors.Studies have shown that[6,52-58]IVIM-DWI can be used for the diagnosis and differentiation of benign and malignant hepatic tumours, and a consensus indicates that the ADC and D values have high efficacy for differential diagnosis.The D value is the only simple diffusion coefficient sensitive to water molecule diffusion.For malignant lesions characterized by diffusion restriction, the D value has higher diagnostic efficiency than the ADC[54-56].Louet al[54]performed IVIMDWI on 74 patients with hepatic tumors and showed that the ADC, D and f values in the malignant group were significantly lower than those in the benign group, with a larger area under the curve for the D value (0.968) and higher differentiation sensitivity (92.30%);however, no statistically significant difference in the D* value was foundbetween the two groups.Furthermore, conflicting results have been reported[53,57,59].The results of the study by Watanabeet al[57]showed that for the identification of benign and malignant hepatic tumors, the area under the receiver operating characteristic (ROC) curve of the ADC value was higher than that of the D value;and Doblaset al[59]suggested that compared with the ADC value, IVIM-DWI parameters could not improve the differentiation efficiency for hepatic focal lesions.
The use of the perfusion-related parameters D* and f for the differentiation of benign and malignant nodules is controversial[58,60].Penner AHet al[60]showed that compared with the traditional ADC, IVIM-DWI parameters were more significantly different between lesions and normal liver tissue.Ichikawaet al[58]studied 84 cases of focal benign and malignant hepatic lesions and found that the D and D* values of malignant hepatic lesions were significantly lower than those of benign hepatic lesions, while the f values showed no difference between benign and malignant hepatic lesions.These results suggested that the D* and D values were inhibited in malignant lesions.In contrast, some studies[52-54,61]have suggested that the D* and f values are meaningless for differentiating benign and malignant hepatic lesions.A possible reason is that the D* value may fluctuate in a large range due to different blood supply types in hepatic hemangiomas[52,61], while the magnitude of the f value depends on the time of echo (TE) (a longer TE corresponds to a greater f value).In addition, D* and f values are not uniquely specific to perfusion and may also be sensitive to other flow information, such as the excretion, direction or pattern of diffusion of a granule or gland[53,57,62](Figures 1 and 2, Table 2).
DIFFERENTIATION OF HEPATIC MALIGNANCIES WITH DIFFERENT PATHOLOGICAL TYPES
Few studies have investigated IVIM-DWI for the differentiation of hepatic malignancies of different pathological types.Previous studies have suggested thatIVIM-DWI is beneficial for the differentiation of hepatocellular carcinoma(HCC)and intrahepatic cholangiocarcinoma (ICC)[63-66], but the differentiation of HCC and metastatic hepatic cancer requires further study[52].Shaoet al[64]discussed the role of IVIM-DWI in differentiating hepatitis B virus (HBV)-related ICC from HCC and found that the ADC and D values of ICC were significantly higher than those of HCC, while the f value of ICC was significantly lower than that of HCC, and the areas under the ROC curves of the ADC, D and f values were 0.724, 0.753 and 0.741, respectively.Weiet al[63]showed that the ADC and D value could differentiate ICC from HCC.However,the D* and f values showed no difference in the ICC and HCC groups.Choiet al[65]studied 161 cases of focal hepatic lesions using IVIM-DWI.The results showed no significant difference in the ADC value in any malignant tumor.The Dslowvalue of HCC was significantly lower than that of ICC, and the f value was significantly higher than those of ICC and metastatic carcinoma.A meta-analysis conducted by Wuet al[52](six papers meeting the requirements) showed that the ADC, D, D* and f values were not significantly different between metastatic liver cancer and HCC.The reason for this finding may be that these metastases originated from some primary tumors such as lesions in the gastrointestinal tract, lung, breast or urogenital system, which may have caused some changes in cell density and microcirculation.In addition, different HCC histological classifications and compositions used in different studies may have also caused certain effects.
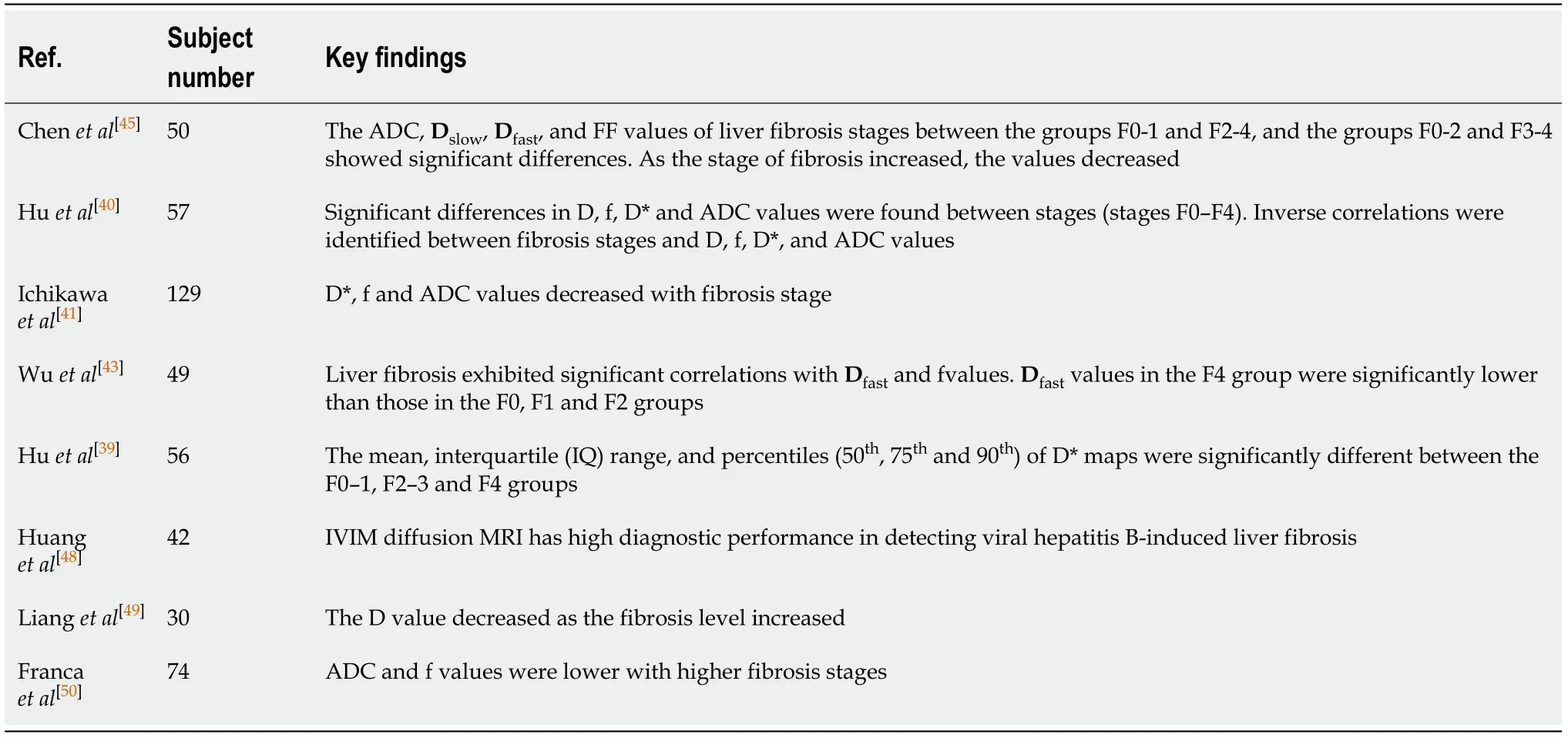
Table 1 Summary of hepatic fibrosis intravoxel incoherent motion diffusion-weighted imaging studies
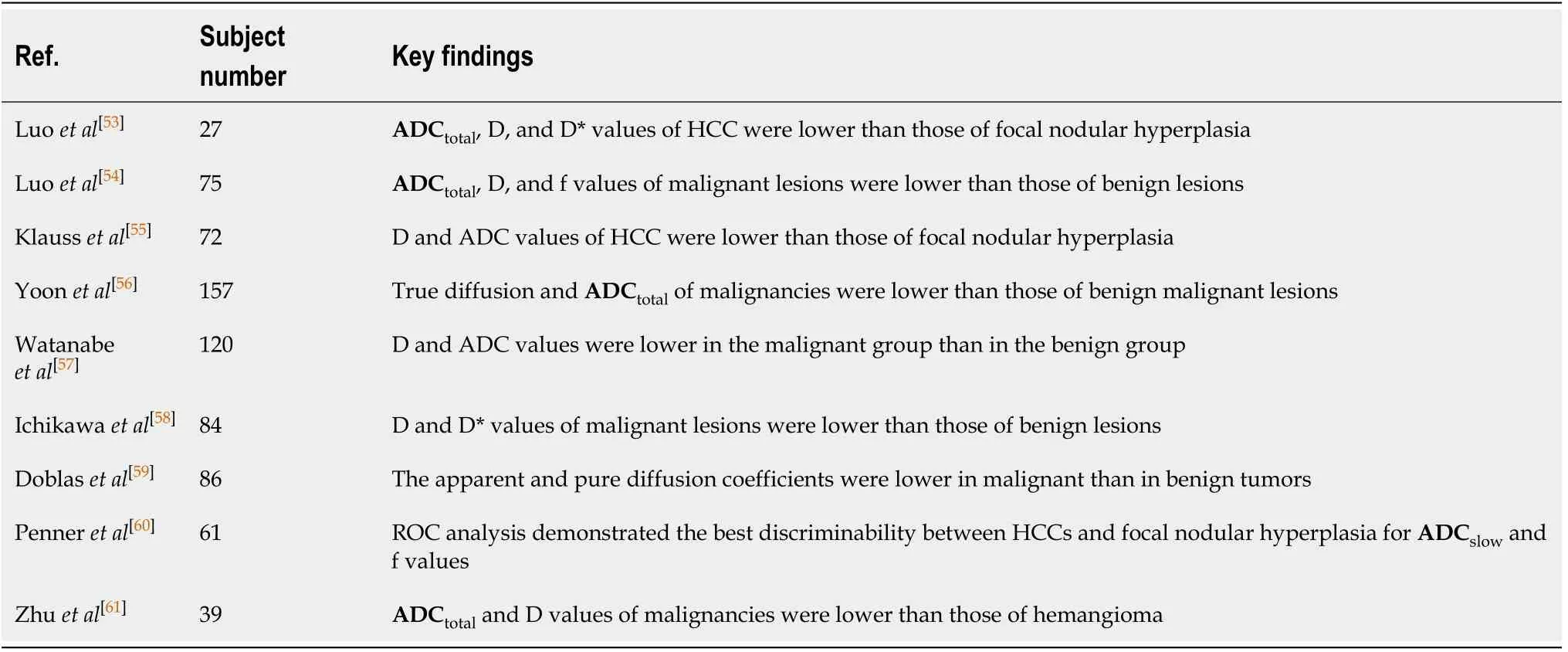
Table 2 Summary of hepatic nodules intravoxel incoherent motion diffusion-weighted imaging studies
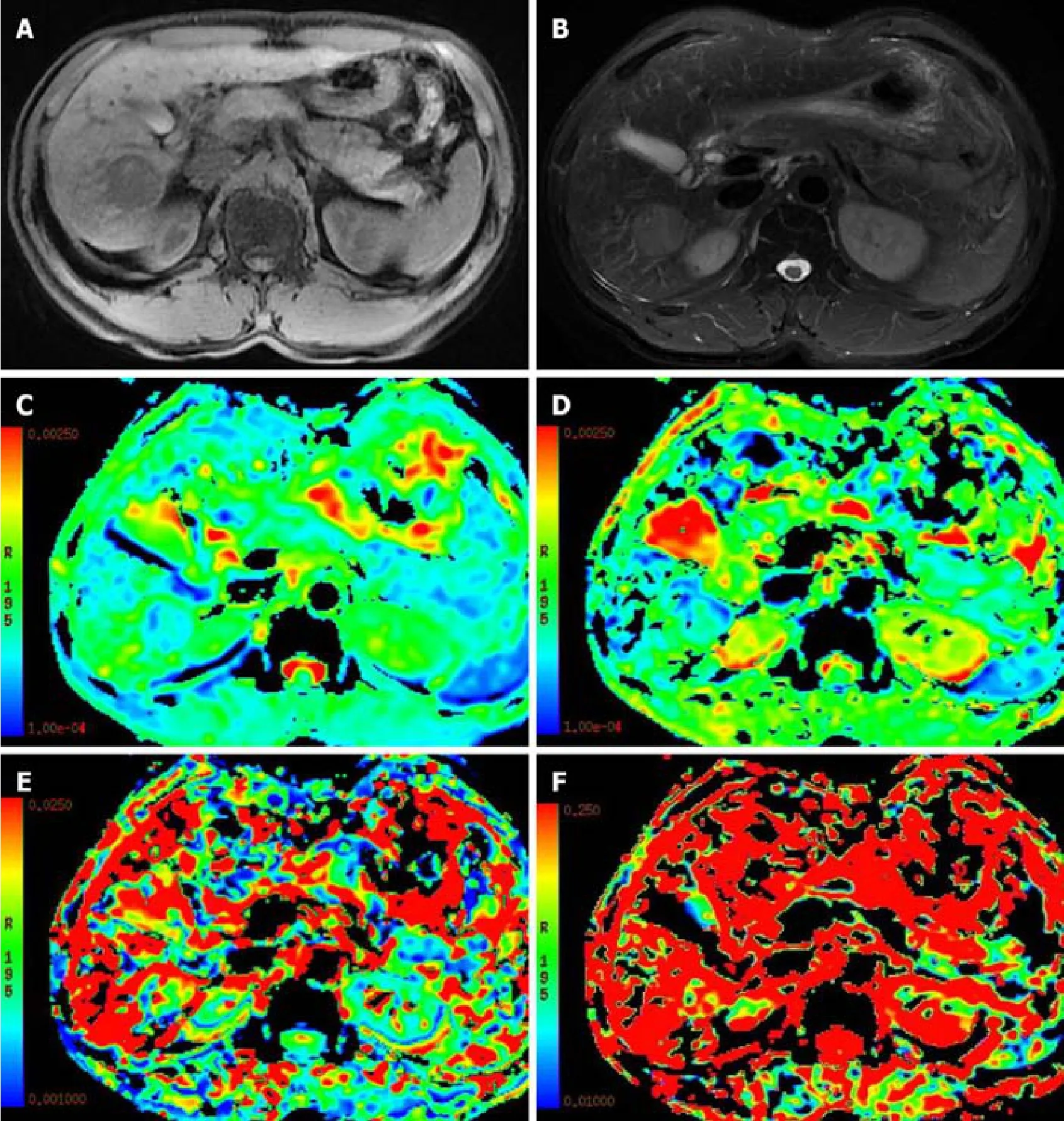
Figure 1 A 51-year-old male patient with hepatocellular carcinoma in the right lobe of the liver.
HCC HISTOLOGICAL CLASSIFICATION
Studies have shown that the IVIM-DWI parameters of HCC are correlated with histological classification[19,67-75].Liet al[73]performed an IVIM-DWI analysis on a rat model of hepatic cancer and showed that the ADC and D values of higher-grade lesions were lower than those of lower-grade lesions, and the ADC and D values were negatively correlated with the tumor’s histological classification.The D* and f values of higher-grade lesions were higher than those of lower-grade lesions, and the D* and f values were positively correlated with the tumor histological classification.During tumorigenesis, as the degree of tumor differentiation becomes increasingly poor, the cellularity and nuclear-to-cytoplasmic ratio increase, and as the extracellular space decreases, water diffusion is restricted, resulting in reduced ADC and D values in poorly differentiated HCC[68,69].
Regarding the role of D* and f values in the histological classification of HCC, the results of available studies are not completely consistent.Sokmenet al[71]showed that the ADC and D values were negatively correlated with the histological classification of HCC, the f value was positively correlated with the histological classification of HCC tissue, and no differences in the D* value in different histological classifications of HCC were observed.Granataet al[74,75]observed the role of the ADC, D and f values in differentiating the histological classifications of HCC but did not observe any significance of the D* value for differentiation.Other studies showed only the roles of the ADC and D value in the differentiation of the histological classifications of HCC,and the roles of D* and f values in differentiation were not observed[19,67-69], which may be explained by differences in b-value groupings and patient populations as well as consequent variation in tumor grade distributions[67,75].
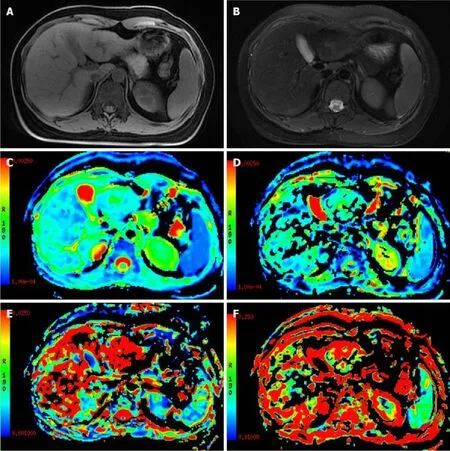
Figure 2 A 28-year-old female patient with focal nodular hyperplasia in the left lobe of the liver.
EVALUATION OF THE HCC TREATMENT RESPONSE
Studies have shown that IVIM-DWI has important application value in the treatment and follow-up of HCC.
Zhanget al[76]conducted IVIM-DWI on 157 patients with HBV-related HCC who underwent surgical resection.The results showed 47 cases of tumor recurrence, and a D value <0.985 × 10-3mm2/s was found to be a risk factor for recurrence.The D value of the IVIM-DWI model has been suggested as a potential biomarker for preoperative prediction of hepatic cancer recurrence[77-79].Zhaoet al[78]reported that D is an independent predictor of microvascular invasion(MVI);when the cut-off D value was 1.16 × 10-3mm2/s, the sensitivity and specificity for predicting MVI were 66.7% and 88.9, respectively.
IVIM-DWI parameters can distinguish the survival area, the fibrous area and the necrotic area of malignant hepatic tumors[80].A study[81]including 15 patients undergoing resection of hepatic metastases of colorectal cancer found that the ADC and D values were associated with the degree of necrosis of metastatic hepatic tumors,suggesting that the specificity of free molecular proliferation of metastatic colorectal cancer increased after systemic chemotherapy.
In the early stages of local or targeted therapy for tumors, changes in tumor volume are often not detected by traditional imaging, and functional imaging is of great value in this field[82,83].IVIM-DWI parameters can be used as biomarkers for early response evaluation[84-88].Studies have shown that IVIM-DWI has important value in the evaluation of transarterial chemoembolization (TACE) treatment responses and the prediction of therapeutic effects in HCC[84,89-93].The study by Penget al[91]showed that after TACE treatment for HCC, the ADC and D values in tumor tissues significantly increased, the D* value decreased significantly, and the f value did not change significantly.The reason for the inconsistent changes in these two perfusion-related parameters may be that the D* and f values represent different aspects of perfusion,the former is mainly related to the capillary velocity of local tissues, while the latter is related to the blood volume of local tissues.The study by Parket al[89]showed that the D* value could reflect the blood supply of HCC and predict the deposition effect of iodide oil after TACE surgery;the D* value and arterial enhancement ratio (AER) of preoperative lesions in the group with better iodized oil deposition were significantly higher than those in the group with poor iodized oil deposition.Wuet al[92]believed that the ADC maybe the best independent predictor of TACE treatment responses.
The IVIM-DWI perfusion parameter f is significantly correlated with microvascular dysplasia (MVD) in HCC[88].IVIM-DWI can be used to evaluate the anti-angiogenic effect of sorafenib on HCC[87,88,94-96].Yanget al[95]established 35 nude mouse models of HCC and conducted IVIM-DWI at baseline and 7, 14 and 21 dafter sorafenib treatment.The results revealed that compared with the control group, the ADC and D values in the treatment group at each time point were significantly increased, while the f value was significantly decreased at 7 d and significantly increased at 21 d.In the treatment group, both the ADC and D values were significantly higher than the baseline values on days 7, 14 and 21, while the f value decreased significantly on the 7thday and increased significantly on the 21stday.In the treatment group, the ADC, D and f values were significantly correlated with the necrotic fraction (NF).These results suggested that IVIM-DWI parameters can be used as biomarkers to evaluate the therapeutic efficacy of sorafenib therapy for HCC.Shirotaet al[87]conducted IVIM-DWI on nine patients with HCC treated with sorafenib, and the results showed that the baseline D value in the responsive group was significantly higher than that in the nonresponsive group.The sensitivity and specificity of the differential therapeutic responses were 100% and 67%, respectively, and the other parameters showed no difference between the two groups, suggesting that the D value can be used to predict the therapeutic response of HCC to sorafenib.
OTHER DISEASES
The application of IVIM-DWI in hepatic ischemia-reperfusion injury (IRI)[97-99], hepatic alveolar echinococcosis[100], hepatic dysfunction[101], hepatic sinus obstruction syndrome[102]and other diseases is also gradually developing.For example, studies have found that IVIM-DWI-related parameters are significantly reduced after liver IRI[99].
CONCLUSION
In conclusion, IVIM-DWI seems to accurately reflect information related to the diffusion of simple water molecules and microcirculatory perfusion in tissues and it could have important application value in the diagnosis of hepatic fibrosis, the differentiation of benign and malignant hepatic lesions, the histological classification of HCC, the evaluation of local and targeted therapeutic response and the prediction of therapeutic efficacy.However, the value of IVIM-DWI in assisting in the histological classification of hepatic fibrosis and in differentiating malignant hepatic tumors with different pathological characteristics still requires further investigation.The standardization of IVIM-DWI scanning technology (such as the optimization and standardization of the number and distribution of b values) is an important topic,which warrants further study.In addition, the characteristics and diagnostic value of the D* and f values still require further exploration.With continuous innovation in IVIM-DWI technology and in-depth clinical research, IVIM-DWI will play a more important role in the diagnosis and treatment of hepatic diseases in the future.
 World Journal of Clinical Cases2020年15期
World Journal of Clinical Cases2020年15期
- World Journal of Clinical Cases的其它文章
- Impacts and challenges of United States medical students during the COVID-19 pandemic
- Recent advances in the management of gastrointestinal stromal tumor
- Medical research during the COVID-19 pandemic
- Typical and atypical COVID-19 computed tomography findings
- Review of possible psychological impacts of COVID-19 on frontline medical staff and reduction strategies
- Overexpression of AMPD2 indicates poor prognosis in colorectal cancer patients via the Notch3 signaling pathway