
Warm needling moxibustion plus PKP for vertebral compression fracture due to kidney deficiency and blood stasis: a randomized controlled trial
2021-04-23 09:07ChenXu陈旭
关键词:陈旭
Chen Xu (陈旭)
Ningbo Hospital of Traditional Chinese Medicine, Zhejiang Province, Ningbo 315000, China
Abstract
Objective: To explore the efficacy and mechanism of warm needling moxibustion plus percutaneous kyphoplasty (PKP)for osteoporotic vertebral compression fracture (OVCF) due to kidney deficiency and blood stasis.
Methods: A total of 70 OVCF patients were randomized into a control group and an observation group, with 35 cases in each group. The control group was given PKP treatment, and the observation group was treated with warm needling moxibustion on the basis of the treatment in the control group. The visual analog scale (VAS) and Oswestry disability index (ODI) were scored and the Cobb angle of fractured vertebrae was measured before and after treatment. The refracture rate of the adjacent vertebrae was recorded at 1-year follow-up. The serum levels of transforming growth factor(TGF)-β1 and omentin-1 were measured before and after treatment.
Results: After treatment, the VAS and ODI scores in both groups decreased (all P<0.05), and all the scores in the observation group were lower than those in the control group (both P<0.05). After treatment, the Cobb angle of fractured vertebrae in both groups decreased (both P<0.05), and the Cobb angle in the observation group was smaller than that in the control group (P<0.05). At 1-year follow-up, the re-fracture rate of the adjacent vertebrae in the observation group was lower than that in the control group (P<0.05). After treatment, the serum levels of TGF-β1 and omentin-1 in both groups increased significantly (all P<0.05), and the serum levels of TGF-β1 and omentin-1 in the observation group were higher than those in the control group (both P<0.05).
Conclusion: The treatment of warm needling moxibustion plus PKP can relieve pain, improve dysfunction, promote healing of the injured vertebrae, and reduce the re-fracture rate of the adjacent vertebrae in patients with OVCF due to kidney deficiency and blood stasis, which may be related to the increase of serum TGF-β 1 and omentin-1 levels.
Keywords: Acupuncture Therapy; Warm Needling Therapy; Percutaneous Kyphoplasty; Osteoporotic Fractures; Fractures,Compression; Randomized Controlled Trial
Osteoporotic vertebral compression fracture (OVCF) is the most common clinical complication of osteoporosis,which is more common in the elderly. It can be induced without external force or by slight external force. The main manifestations are loss of vertebral longitudinal height and pain[1]. Thoracolumbar vertebrae are the most common sites of OVCF due to the anatomical and biomechanical characteristics[2]. Percutaneous kyphoplasty (PKP) has been widely used in the clinical treatment of OVCF. It has advantages of early relief of pain and restoring vertebral longitudinal height as much as possible. However, some patients may have residual back pain after surgery and secondary adjacent vertebral fractures[3]. Therefore, how to promote the postoperative rehabilitation of OVCF patients and prevent secondary vertebral fractures is the current research hotspot. Acupuncture has the effects of unblocking meridians and collaterals, and regulating Zang-fu organs, widely being applied in the orthopedic postoperative rehabilitation[4]. Moreover, it has achieved satisfactory effect in the treatment of osteoporosis[5].Therefore, in this study, we used warm needling moxibustion plus PKP to treat OVCF due to kidney deficiency and blood stasis, observed the efficacy, and the effects on serum transforming growth factor-β1(TGF-β1) and omentin-1.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria in Western medicine[6]
Those who had typical manifestations such as low back pain, restricted mobility, and kyphosis; who had a confirmed diagnosis of osteoporosis by bone mineral density (BMD) test; and a confirmed diagnosis of vertebral compression fracture by X-ray, CT or MRI examination.
1.1.2 Criteria for syndrome differentiation of traditional Chinese medicine (TCM)[7]
Those met the criteria of syndrome of kidney deficiency and blood stasis. Primary manifestations: pain in the back and low back, with soreness and weakness.Secondary manifestations: hard to walk, difficult to turn back, bend over or stretch backward; dizziness; a dark tongue or petechial on the tongue, sunken and stagnant pulse.
1.2 Inclusion criteria
Those who met the above diagnostic criteria of OVCF in Western medicine and the syndrome of kidney deficiency and blood stasis for syndrome differentiation of TCM; aged 50 to 70 years old; fresh fracture indicated by image examination, and the compression fractures affecting 1-3 vertebrae; PKP treatment was required;patients and their families agreed to participate in this trial and signed informed consent.
1.3 Exclusion criteria
Those with old vertebral compression fracture or pathological fracture; presenting with spinal cord compression and nerve injury symptoms such as urinary and fecal dysfunction; those who had severe diseases of heart, lung, liver or kidney; those who were unconscious and unable to complete the trial.
1.4 Elimination and dropout criteria
Those who dropped out during the treatment; with poor compliance and unable to cooperate during the treatment; those presenting with severe adverse reactions.
1.5 Statistical methods
All data were statistically analyzed by SPSS version 20.0 statistical software. Counting data were processed by Chi-square test. Measurement data were expressed as mean ± standard deviation (±s). The intra-group comparison was analyzed by pairedt-test, and the comparison between the groups was analyzed by groupt-test.P<0.05 was considered to indicate a statistically significant difference.
1.6 General data
A total of 70 OVCF patients were enrolled from Ningbo Hospital of Traditional Chinese Medicine, Zhejiang Province, between January 2016 and December 2017.The patients were randomly divided into a control group and an observation group by the random number table according to the visiting sequence, with 35 cases in each group. During the trial, there was no dropout case in the two groups. There were no significant differences in the data of gender, age and number of vertebral fractures between the two groups (allP>0.05), indicating that the two groups were comparable (Table 1).
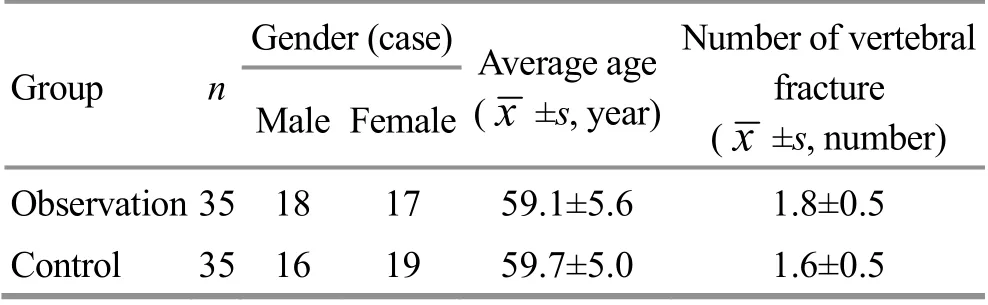
Table 1. Comparison of general data between the two groups
2 Treatment Methods
2.1 Control group
Patients in the control group were treated with PKP surgery.
The patient took a prone position. The physician confirmed the vertebral body to be operated under Carm fluoroscopy, and marked the corresponding puncture point. After disinfection and anesthesia, a 0.5 cm incision was made at the puncture point with a scalpel, and the puncture needle was inserted through the pedicle of the surgical vertebral arch and punctured to the anterior and middle 1/3 of the surgical vertebra.Then the physician inserted the guiding needle, changed the liner, placed the balloon and inflated it. After the injured vertebrae was supported to a satisfactory height,the balloon was removed and pre-formulated bone cement was installed. Under the monitoring of the C-arm machine, the bone cement was pushed into the vertebral body through the pedicle canal, and the infusion was stopped when the surgical vertebral body was filled with bone cement. The puncture needle was pulled out immediately after the bone cement was solidified. And the patient was escorted back to the ward after his condition was stable without discomfort[8]. The patient was supine for 6 h after surgery. And 24 h after the surgery, the patient could get out of bed.
2.2 Observation group
Patients in the observation group received the same PKP treatment as in the control group, and then they were treated with warm needling moxibustion 24 h after the PKP surgery.
Acupoints used during the first month after surgery:Guanyuan (CV 4) and bilateral Xuehai (SP 10). Acupoints used during the second month after surgery: bilateral Geshu (BL 17) and Shenshu (BL 23).
Methods:The physician punctured the acupoints using Hwato brand sterile acupuncture needles of 0.25 mm in diameter and 40 mm in length (Suzhou Medical Supplies Factory Co., Ltd., China). The patient took a supine or prone position, with the skin of acupoint area exposed. After disinfection with 75% alcohol cotton balls, the physician applied fingernail-pressure needle insertion method. All the acupoints were perpendicularly punctured by 0.8-1.0 cun in depth, with lifting-thrusting and twirling manipulations. After the arrival of qi, even reinforcing-reducing manipulation was applied. Then the physician inserted a piece of moxa stick of 1 cm in diameter and 1.5 cm in length onto each needle handle, and placed a thick cardboard between the moxa and the skin, then ignited the moxa from the bottom. The needles were retained for 30 min, then the moxa ash was removed and the needles were withdrawn.The warm needling moxibustion was performed every other day for 2 months in total.
3 Observation of Curative Efficacy
3.1 Observation items
3.1.1 Visual analog scale (VAS) score
VAS was used to evaluate the pain degree of the fracture area before and after treatment. The VAS score ranged from 0 to 10 points. The higher the VAS score, the severer the pain[9].
3.1.2 Oswestry disability index (ODI) score
ODI questionnaire was completed before and after treatment by the patient independently, to evaluate the influence of low back pain on the daily life. The higher the score, the worse the dysfunction[10].
3.1.3 Cobb angle of the fractured vertebrae
The Cobb angle of fractured vertebrae was measured before and after treatment by lateral X-ray film. Cobb angle can reflect the healing progress of vertebral fractures[11]. The larger the Cobb angle, the worse the stability of the vertebral body.
3.1.4 Re-fracture rate of the adjacent vertebrae
Patients were followed up for 1 year after treatment,and the re-fracture rate of the adjacent vertebrae was compared between the two groups.
3.1.5 Serum TGF-β1 and omentin-1 levels
The fasting venous blood was collected in early morning before and after treatment. The serum TGF-β1 and omentin-1 levels were measured by enzyme-linked immunosorbent assay.
3.2 Results
3.2.1 Comparison of VAS and ODI scores
Before treatment, there were no statistically significant differences in the VAS and ODI scores between the two groups (bothP>0.05), indicating that the two groups were comparable. After treatment, the VAS and ODI scores in both groups decreased (allP<0.05).The VAS and ODI scores in the observation group were lower than those in the control group (bothP<0.05),(Table 2).
3.2.2 Comparison of the Cobb angle of fractured vertebrae
Before treatment, there was no statistically significant difference in the Cobb angle of fractured vertebrae between the two groups (P>0.05). After treatment, the Cobb angle of fractured vertebrae in both groups decreased (bothP<0.05). The Cobb angle of fractured vertebrae in the observation group were smaller than that in the control group (P<0.05), (Table 3).
3.2.3 Comparison of re-fracture rate of the adjacent vertebrae
At the one-year follow-up, there were 8 cases of refracture of the adjacent vertebrae in the control group,and the re-fracture rate was 22.9%. There was one case of re-fracture of the adjacent vertebrae in the observation group and the re-fracture rate was 2.9%. The re-fracture rate of the adjacent vertebrae in the observation group was lower than that in the control group (P<0.05).
Table 2. Comparison of VAS and ODI scores between the two groups ( ±s, point)

Table 2. Comparison of VAS and ODI scores between the two groups ( ±s, point)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n VAS ODI Before treatment After treatment Before treatment After treatment Observation 35 5.59±0.89 1.51±0.301)2) 48.46±4.56 24.51±3.021)2)Control 35 5.37±0.87 1.96±0.571) 47.08±4.43 29.71±3.061)
Table 3. Comparison of the Cobb angle of fractured vertebrae between the two groups ( ±s, °)
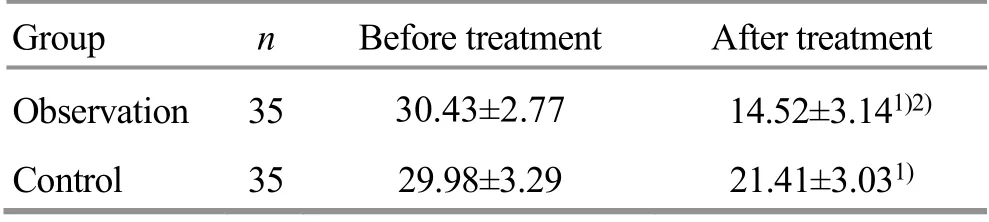
Table 3. Comparison of the Cobb angle of fractured vertebrae between the two groups ( ±s, °)
Note: Compared with the same group before treatment, 1) P<0.05;compared with the control group after treatment, 2) P<0.05
Group n Before treatment After treatment Observation 35 30.43±2.77 14.52±3.141)2)Control 35 29.98±3.29 21.41±3.031)
3.2.4 Comparison of serum TGF-β1 and omentin-1 levels
Before treatment, there were no statistically significant differences in the serum levels of TGF-β1 and omentin-1 between the two groups (bothP>0.05). After treatment, the serum levels of TGF-β1 and omentin-1 in both groups increased significantly (allP<0.05), and the serum levels of TGF-β1 and omentin-1 in the observation group were higher than those in the control group (bothP<0.05), (Table 4).
Table 4. Comparison of serum TGF-β1 and omentin-1 levels between the two groups ( ±s, ng/mL)

Table 4. Comparison of serum TGF-β1 and omentin-1 levels between the two groups ( ±s, ng/mL)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n TGF-β1 Omentin-1 Before treatment After treatment Before treatment After treatment Observation 35 4.03±0.57 7.54±1.581)2) 30.31±2.91 42.27±4.921)2)Control 35 4.14±0.65 5.43±0.791) 30.18±2.97 35.98±3.691)
4 Discussion
OVCF belongs to bone Bi-impediment syndrome and bone wither in TCM. The location of the disease is in bone and is closely related to kidney, liver and spleen.Kidney deficiency is the basic cause of OVCF, and internal blockade of static blood is the key pathogenesis[12]. The growth and development of bones are closely related to kidney qi. If the essence of the kidney is sufficient, the bones will be strong; if the essence of the kidney is deficient, the bone marrow will lose its nourishment and the bones will be brittle. Qi deficiency causes poor blood circulation, leading to blood stasis. Exogenous pathogen invasion causes blockage of meridians and impediment of blood circulation, which can also lead to blood stasis.The disease duration of osteoporosis is long and lingering,and the chronic disease invading collaterals can also cause blood stasis. Therefore, kidney deficiency and blood stasis should be the key pathogenesis of OVCF, and it is a common clinical syndrome. Thus, invigorating kidney and promoting blood circulation should be the main treatment principle for this disease[13].
Warm needling moxibustion is a TCM treatment that combines acupuncture and moxibustion. It is suitable for diseases that require both needle retention and moxibustion, so as to achieve the effects of warming and unblocking the meridians, and promoting qi movement and blood circulation[14]. In this study, Guanyuan (CV 4)and Xuehai (SP 10) were selected during the first month after surgery, and Geshu (BL 17) and Shenshu (BL 23)were selected during the second month after surgery.Guanyuan (CV 4) is where the Yuan-Primordial qi stays,with the effects of invigorating and reinforcing Yuan-Primordial qi, warming spleen and benefiting kidney.Xuehai (SP 10) is the key point for all kinds of blood syndromes, since it can nourish blood and activate blood flow, and combine unblocking with tonifying. The combination of these two acupoints has effects of warming kidney and consolidating essence, activating blood flow and nourishing blood. Geshu (BL 17) is one of the Eight Influential points (blood). It can nourish blood and harmonize nutrient-blood, regulate qi flow and relieve chest, activate blood flow and unblock collaterals.Shenshu (BL 23) is the Back-Shu point of kidney, the key point for kidney diseases. It can invigorate kidney and reinforce yang, and warm kidney for better control of respiration. The combination of Geshu (BL 17) and Shenshu (BL 23) can warm and unblock blood vessels,and warmly invigorate kidney qi. The wound was basically healed in the second month after surgery, so Geshu (BL 17) and Shenshu (BL 23) were selected to enhance the therapeutic effects. In this study, the results suggested that the VAS and ODI scores in both groups significantly decreased after treatment (allP<0.05), and the VAS and ODI scores in the observation group were lower than those in the control group (bothP<0.05).After treatment, the Cobb angle of fractured vertebrae in both groups decreased (bothP<0.05), and the Cobb angle of fractured vertebrae in the observation group were smaller than that in the control group (P<0.05). The re-fracture rate of adjacent vertebrae in the observation group was lower than that in the control group at oneyear follow-up (P<0.05). These results indicated that warm needling moxibustion plus PKP could obviously relieve pain, improve dysfunction, promote the healing of injured vertebrae, and reduce the re-fracture rate of adjacent vertebrae in patients with OVCF.
In this study, we also observed the change of serum levels of TGF-β1 and omentin-1 of the patients in both groups. TGF-β1 is more abundantly expressed in bone tissue. TGF-β1 is released from platelets degranulation.It stimulates and repairs cell proliferation, and initiates the repair process. In cartilage bone stage, TGF-β1 is synthesized and released into the bone matrix by chondrocytes, and osteoclasts absorb TGF-β1 from the bone matrix and act on osteoblasts to stimulate intramembranous ossification and inhibit osteoclast formation[15-16]. Clinical study confirmed that serum TGFβ1 expression in OVCF patients was low, and it was negatively correlated with bone transformation indicators[17]. Omentin-1 mainly comes from omental adipose tissue and is a protective adipocytokine.Omentin-1 can reduce osteoclast generation and inhibit osteoblast differentiation by stimulating the osteoprotegerin production and inhibiting the expression of nuclear factor-κB receptor activator ligands,so as to affect BMD and bone strength[18-19]. Clinical study suggested that the serum omentin-1 level in premenopausal women could be used as an independent predictor of BMD, which was negatively correlated with bone alkaline phosphatase. And their serum omentin-1 level was positively correlated with the BMD of femoral neck and total hip joint, and osteocalcin[20]. Therefore, serum TGF-β1 and omentin-1 play an important role in the pathogenesis and prognosis of OVCF. In this study, the serum TGF-β1 and omentin-1 levels in both groups increased significantly after treatment (allP<0.05), and the serum TGF-β1 and omentin-1 levels in the observation group were higher than those in the control group (bothP<0.05). These results indicated that warm needling moxibustion could obviously increase the serum TGF-β1 and omentin-1 levels of the patients, which might be related to the mechanism of warm needling moxibustion plus PKP for OVCF due to kidney deficiency and blood stasis.
In summary, warm needling moxibustion plus PKP can relieve pain, improve dysfunction, promote the healing of injured vertebrae, and reduce the re-fracture rate of adjacent vertebrae in patients with OVCF due to kidney deficiency and blood stasis, which may be related to the increase of serum TGF-β 1 and omentin-1 levels.However, due to limited conditions, this study still had the following shortcomings. First, the sample size was small and the sample source was relatively single, which would affect the reliability of the conclusion to some extent. Second, the relevant stimulating parameters of warm needling moxibustion were not studied. The manipulation, frequency, treatment course and number of moxibustion cone would affect clinical efficacy. Third,the possible differences in the efficacy between two different pairs of acupoints for nourishing kidney and activating blood flow, Guanyuan (CV 4) and Xuehai (SP 10)versus Geshu (BL 17) and Shenshu (BL 23), had not been observed. Fourth, the BMD of the patients had not been measured. Osteoporosis is the basis of the pathogenesis of OVCF, and it is important to monitor the changes of BMD before and after treatment. Therefore, largesample, multi-center randomized clinical trials, with
more subjective indicators included should be designed in the future. Moreover, comparison of the relevant stimulating parameters of warm needling moxibustion and acupoints should be studied, in order to enhance the reliability of the study results.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 23 February 2020/Accepted: 9 June 2020
猜你喜欢
上海故事(2022年8期)2022-11-09
电影文学(2022年8期)2022-05-24
Plasma Science and Technology(2022年1期)2022-02-15
艺术品鉴(2021年30期)2021-11-26
留学(2021年4期)2021-03-03
考试与评价·八年级版(2020年2期)2020-10-29
考试与评价·八年级版(2020年1期)2020-10-26
北京广播电视报(2017年31期)2018-02-26
当代工人(2017年20期)2017-12-06
蓝盾(2017年9期)2017-11-15
 Journal of Acupuncture and Tuina Science2021年2期
Journal of Acupuncture and Tuina Science2021年2期
- Journal of Acupuncture and Tuina Science的其它文章
- Review of systematic reviews of acupuncture for diabetic peripheral neuropathy
- Clinical observation on spleen-invigorating and qibenefiting pediatric massage for treating recurrent respiratory tract infection in children with cerebral palsy due to qi deficiency of spleen and lung
- Acupoint catgut-embedding therapy as promising treatment for non-alcoholic fatty liver disease
- Clinical observation of electroacupuncture with different frequencies for migraine without aura
- Evaluation of the prevention and treatment effects of acupuncture-moxibustion for Alzheimer disease based on various mouse models
- Effects of moxibustion on the P2X7R/STAT3/VEGF pathway in rats with colitis-associated colon cancer