单相抑郁与双相抑郁患者T淋巴细胞亚群特征
2021-11-30 15:01杨胜良黄龙武戴红钱敏才洪秀娟沈仲夏
中国现代医生 2021年18期
杨胜良 黄龙武 戴红 钱敏才 洪秀娟 沈仲夏

[關键词] 单相抑郁;双相抑郁;CD4+;CD8+
[中图分类号] R749.42 [文献标识码] A [文章编号] 1673-9701(2021)18-0023-04
Characteristics of T lymphocyte subsets in patients with unipolar depression and bipolar depression
YANG Shengliang1 HUANG Longwu2 DAI Hong1 QIAN Mincai1 HONG Xiujuan3 SHEN Zhongxia1
1.Department of Psychosomatics, Huzhou Third People′s Hospital in Zhejiang Province, Huzhou 313000, China; 2.Department of Pathology, Huzhou Third People′s Hospital in Zhejiang Province, Huzhou 313000, China; 3.Key Laboratory of Psychiatry, Huzhou Third People′s Hospital in Zhejiang Province, Huzhou 313000, China
[Abstract] Objective To compare the characteristics of peripheral blood T lymphocyte subsets in patients with unipolar depression and bipolar depression, to find immunological differential diagnosis indicators for unipolar and bipolar depression. Methods A prospective research method was used to select patients hospitalized in the Department of Psychosomatics in our hospital from June 2018 to October 2019. There were 600 patients in the unipolar depression group and 60 patients in the bipolar depression group. A total of 30 healthy people in the hospital were selected as the healthy control group. Blood samples were collected from the three groups. The counts of CD3+, CD4+, CD8+ and CD4+/CD8+ cell substes in peripheral blood were detected using CD series cell detection slides, and related analysis was performed. Results There were statistically significant differences in the counts of CD3+, CD4+ and CD8+ in peripheral blood among the unipolar depression group, the bipolar depression group and the healthy control group (P<0.001). The counts of CD3+, CD4+ and CD8+ in the unipolar depression group were lower than those in the bipolar depression group and the healthy control group, with statistically significant differences(P<0.01). The counts of CD3+ and CD8+ in the bipolar depression group were lower than those in the healthy control group, with statistically significant differences (P<0.01). The counts of CD4+ in the bipolar depression group were lower than those in the healthy control group, but without statistically significant differences (P>0.05). Conclusion Patients with unipolar depression and bipolar depression have abnormal distribution of T lymphocyte subsets. T lymphocyte subsets can be used to differentiate between unipolar depression and bipolar depression.
[Key words] Unipolar depression; Bipolar depression; CD4+; CD8+
抑郁症是一种临床上常见的慢性精神疾病,与抑郁症相比,双相障碍治疗更困难,自杀风险更大,1/3以上抑郁症患者在10年后才被修正诊断为双相障碍[1]。人体免疫系统与中枢神经系统具有密切联系[2-3],情绪障碍和应激事件可以影响免疫功能,而免疫功能的改变也可能成为抑郁障碍的病因[4-5]。调节性T细胞在双相障碍患者中存在明显的下降[6],免疫功能失调可能是双相情感障碍发病的重要机制之一[7]。T淋巴细胞计数及其亚群的改变可在很大程度上反映免疫水平的改变[8],抑郁症(单相抑郁)与双相情感障碍抑郁发作(双相抑郁)两者之间T淋巴细胞亚群分布特征还不清楚。本研究通过T淋巴细胞(CD3+、CD4+、CD8+)计数的检测,探讨单相抑郁、双相抑郁与健康人群三者之间T淋巴细胞变化,从而寻找单、双相抑郁的免疫学鉴别诊断标志物,现报道如下。
1 对象与方法
1.1 研究对象
所有研究对象为2018年6月至2019年10月我院心身科住院患者。纳入标准:符合《国际疾病分类第十次修订本精神和行为障碍诊断标准》ICD-10抑郁发作和双相情感障碍抑郁发作诊断标准。排除标准:①类风湿性关节炎、系统性红斑狼疮等免疫系统疾病者;②近1年内未曾使用过免疫抑制剂者;③近半个月内无感染性疾病者[7];④严重躯体疾病、酒精或药物依赖者等。所有研究对象均被告知研究流程,同时签署书面知情同意书,共收集入组单相抑郁组共600例,男146例,女454例,平均年龄(42.02±10.38)岁;双相抑郁组共60例,男21例,女39例,平均年龄(41.27±11.89)岁;健康对照为来本院体检合格人员共30例,男10例,女20例,平均年龄(40.50±11.64)岁,排除既往/现患精神疾病及感染性疾病。三组年龄比较,差异无统计学意义(F=2.472,P>0.05),具有可比性。
1.2 方法
对研究对象和健康对照组人员抽取清晨空腹静脉血2 mL(以EDTA为抗凝剂),送湖州市第三人民医院病理科进行淋巴细胞亚群检测,包括CD3+、CD4+、CD8+T淋巴细胞,采用CD系列(CD3+/4+/8+)细胞检测玻片,所用玻片均购于上海汇中细胞生物科技有限公司。
采用CD系列细胞检测玻片进行检测,具体方法如下:加380 μL缓冲液于2 mL圆底管中并标记样本编号,加20 μL摇匀血样于缓冲液中,即刻混匀稀释血样,吸取5 μL稀释血样滴入玻片各抗体包被区中央,孵育40 min后,按序插入染色架,即刻放入缓冲液中旋转提拉至无色透明,立即放入过氧化物酶染色液中静置1 min,取出稍加沥干,放入新鲜过氧化氢工作溶液中,静置4 min。将染色架放入400 mL75%乙醇染液缸中,旋转提拉至无色透明,干燥仪下干燥6 min,将染色架放入血细胞分析用染色液,静置1 min,再转入500 mL纯水染液缸中,静置30 s,提拉3~5下,干燥后用显微镜自动计数。
1.3观察指标及评价标准
T淋巴细胞计数可反映免疫水平[8],本研究采用CD系列细胞检测玻片检测外周血中CD3+、CD4+、CD8+、CD4+/CD8+细胞亚群计数,CD3+、CD4+、CD8+正常值标准分别为(770~2860)个细胞/μL、(414~1440)个细胞/μL、(238~1250)个细胞/μL。
1.4 统计学方法
应用 SPSS 19.0统计学软件进行数据分析,计量资料以均数±标准差(x±s)表示,组间比较采用t检验;计数资料以[n(%)]表示,组间比较采用χ2检验,P<0.05为差异有统计学意义。
2 结果
2.1 三组CD3+、CD4+、CD8+数值及CD4+/CD8+比值比较
单相抑郁组、双相抑郁组与健康对照组三组CD3+、CD4+、CD8+数值比较,差异有统计学意义(P<0.001),三组CD4+/CD8+比值相比,差异有统计学意义(P<0.01)。见表1。
2.2 三组间CD3+、CD4+、CD8+计数两两比较
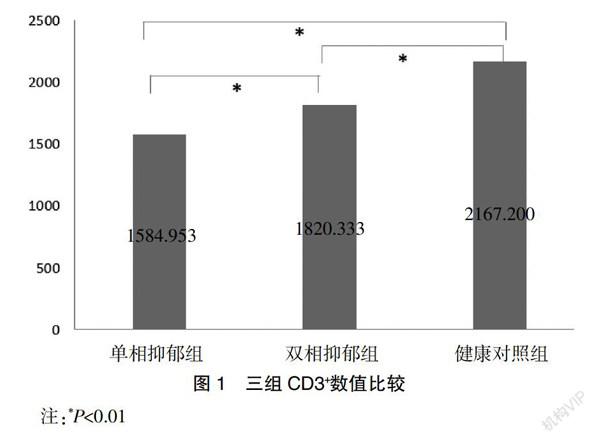
2.2.1 CD3+计数组间比较 单相抑郁组显著低于健康对照组,差异有统计学意义(P<0.01);双相抑郁组同样低于健康对照组,差异有统计学意义(P=0.01);单相抑郁组显著低于双相抑郁组,差异有统计学意义(P<0.01)。见图1。
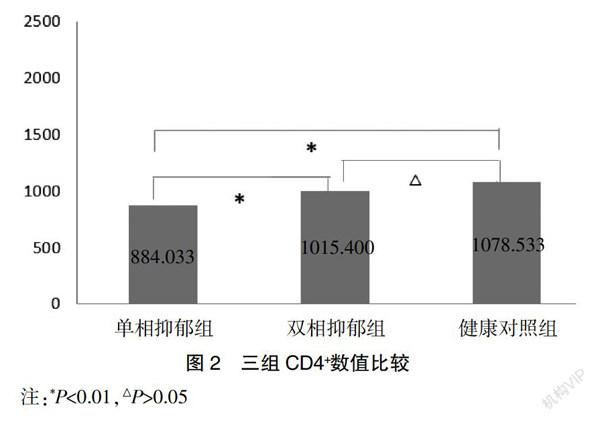
2.2.2 CD4+计数组间比较 单相抑郁组显著低于健康对照组,差异有统计学意义(P<0.01);但双相抑郁组与健康对照组比较,差异无统计学意义(P=0.324);单相抑郁组显著低于双相抑郁组,差异有统计学意义(P=0.001)。见图2。
2.2.3 CD8+计数组间比較 单相抑郁组显著低于健康对照组,差异有统计学意义(P<0.01);双相抑郁组同样低于健康对照组,差异有统计学意义(P<0.01);同时单相抑郁组显著低于双相抑郁组,差异有统计学意义(P=0.002)。见图3。
3 讨论
本研究通过比较抑郁症患者外周T细胞亚群特征性变化,结果显示单相抑郁组CD3+、CD4+和CD8+计数均显著低于健康对照组(P<0.01),而双相抑郁组CD3+和CD8+计数均显著低于健康对照组(P<0.01),单相抑郁组CD3+、CD4+、CD8+计数低于双相抑郁组(P<0.01);单相抑郁组和双相抑郁组CD4+/CD8+比值均高于健康对照组(P<0.01),但单相抑郁组和双相抑郁组CD4+/CD8+比值比较,差异无统计学意义(P>0.05)。
大量研究报告抑郁症存在T细胞缺陷[9],目前抑郁症与双相情感障碍生物学因素仍有待明确,发病机制可能涉及遗传、环境及社会心理等多种因素,传统的单胺功能异常假说受到越来越多的挑战,而以神经炎症为核心的神经免疫因素成为目前的研究热点[10-11],包括细胞因子、免疫细胞数量、比例的异常均可导致神经、内分泌和免疫系统紊乱[12-13]。T淋巴细胞可分为CD3+、CD4+和CD8+等亚群,CD3+代表总T淋巴细胞,其数量直接反映机体的免疫活性;CD4+为T辅助细胞,可促进B淋巴细胞分泌抗体;CD8+为T杀伤细胞,直接参与病毒清除过程[14]。CD3+、CD4+、CD8+是T细胞信号传导的主要分化群,在外周血免疫细胞循环功能中起到关键作用[15],CD4+、CD8+计数以及CD4+/CD8+比值可以一定程度反映中枢神经免疫功能状态和平衡。
目前临床缺乏有效的工具鉴别单相和双相抑郁,国外研究发现高达60%的双相障碍被误诊为单相抑郁[16],而国内相关研究结果显示,双相障碍及其亚型双相障碍Ⅰ型、Ⅱ型被误诊为抑郁症的比例分别为20.8%、7.9%和12.8%[17],单双相抑郁可能存在不同的免疫特征,目前直接比较单相抑郁和双相抑郁患者T细胞亚群计数的研究尚不多见。本研究结果显示,单相抑郁与双相抑郁患者T淋巴细胞亚群数量均较健康人群减少,三组CD3+、CD4+、CD8+数值比较,差异有统计学意义(P<0.001),单相抑郁比双相抑郁CD3+、CD4+、CD8+数值更低(P<0.01),提示单相抑郁和双相抑郁患者均存在一定的免疫失衡,单相抑郁T细胞的表达水平下降更严重。与马永能等[18]研究结果相似。抑郁症组 CD4+/CD8+比值低于健康对照组,抑郁症存在免疫功能紊乱。本研究结果显示,双相抑郁患者CD3+、CD8+数值均低于健康对照组(P<0.01),CD4+数值也低于健康对照组,但差异无统计学意义(P>0.05)。郑亚丽[19]研究显示,双相障碍抑郁组外周血细胞毒性T细胞(CD3+、CD8+)表达明显低于健康对照组,与本研究结果一致。Pietruczuk 等[20]研究发现,所有双相障碍患者CD3+/CD4+和CD3+/CD8+细胞百分率均低于正常人。Becking等[21]研究结果显示,抑郁症患者CD4T辅助细胞缺乏,而双相障碍患者CD4T辅助细胞水平正常甚至升高,也与本研究结果类似。进一步证实单、双相抑郁患者细胞免疫功能低下,致使神经-内分泌-免疫之间的协调性破坏,造成内环境失衡,单相抑郁T细胞数值更低,免疫失衡更严重。
综上所述,单相抑郁、双相抑郁患者均存在T淋巴细胞表达水平下降,且单、双相抑郁间的差异较明显,T淋巴细胞亚群可作为临床单、双相抑郁诊断的参考依据,可以尝试用于单、双相抑郁鉴别。抑郁症和双相障碍的病因复杂,神经-内分泌-免疫系统之间相互交错,各细胞因子间如何相互影响、如何发挥作用等,还有待进一步研究,同时本研究样本量不平衡,未能排除年龄等混杂因素进行分层研究,也是本研究的局限性所在。
[参考文献]
[1] 陆林.沈渔邨精神病学[M].6版.北京:人民卫生出版社,2018:344.
[2] Osimo EF,Pillinger T,Rodriguez IM,et al. Inflammatory markers in depression:A meta-analysis of mean differences and variability in 5,166 patients and 5,083 controls[J].Brain Behavior and Immunity,2020,87:901-909.
[3] Benedetti M,Anyonucci D,Pascali SAD,et al.Crosstalk between endocannabinoid and immune systems:A potential dysregulation in depression?[J].Psychopharmacology,2016,233(9):1-14.
[4] 邓亚洁,刘雨佳,何漪,等. 抑郁癥患者Th17免疫调节相关炎性细胞因子与抑郁严重程度的相关性[J]. 中华行为医学与脑科学杂志,2021,30(5):420-425.
[5] Russo S. Individual differences in immune-brain interface promotes stress vulnerability:Implications for the study of depression[J]. Biological Psychiatry,2020,87(9):S2-S3.
[6] Ashari NSM,Sanusi SNFM,Yasin MAM,et al. Major depressive disorder patients on antidepressant treatments display higher number of regulatory T cells[J]. The Malaysian Journal of Pathology,2019,41(2):169-176.
[7] Lee Y,Mansur RB,Brietzke E,et al. Peripheral inflammatory biomarkers define biotypes of bipolar depression[J].Molecular Psychiatry,2021,89(9):S156.
[8] Ko FY,Tsai SJ,Yang AC,et al.Association of CD8 T cells with depression and anxiety in patients with liver cirrhosis[J].International Journal of Psychiatry in Medicine,2013,45(1):15-29.
[9] Patas K,Willing A,Demiralay C,et al. T cell phenotype and T cell receptor repertoire in patients with major depressive disorder[J].Front Immunol,2018(9):291.
[10] Uintl,Bastos GM,Thurow HS,et al. Increased levels of plasma IL-1b and BDNF can predict resistant depression patients[J].Rev Assoc Med Bras,2019,65(3):361-369.
[11] 錢晓娟,陈国强,周新明,等.双相障碍患者治疗前后血清白介素6(IL-6)等细胞因子水平的变化[J].国际精神病学杂志,2017,44(3):401-403.
[12] Filiano AJ,Xu Y,Tustison NJ,et al. Unexpected role of interferon- γ in regulating neuronal connectivity and social behaviour[J].Nature,2016,535(7612): 425-429.
[13] 卜琴芳,陈方斌,张李婉,等. 氟西汀对抑郁症患者血清CD3、CD4和CD8细胞水平和糖脂代谢的影响[J].西部医学,2017,29(11):1520-1523.
[14] Lynall ME,Turner L,Bhatti J,et al. Peripheral blood cell-stratified subgroups of inflamed depression[J]. Biological Psychiatry,2020,88(2):185-196.
[15] 赵剑华,张静霞,彭晓明,等. 改良中医情绪疗法联合帕罗西汀在抑郁症患者中的疗效观察及对外周血T淋巴细胞亚群的影响研究[J]. 中国免疫学杂志,2019, 35(11):1314-1319.
[16] Fears SC,Reus VI,Dunn W.Bipolar disorder[M]. Rosenberg′s Molecular and Genetic Basis of Neurological and Psychiatric Disease (Sixth Edition),2020:633-652.
[17] 方贻儒,汪作为,陈俊. 中国双相障碍的研究现状与展望[J]. 中华精神科杂志,2015,48(3):141-146.
[18] 马永能,何芳,张洁,等. 抑郁症患者淋巴细胞亚群免疫表型分析[J]. 四川精神卫生,2018,31(4):339-343.
[19] 郑亚丽.双相障碍抑郁相患者T细胞免疫功能的研究[D].杭州:浙江大学医学院,2017.
[20] Pietruczuk K,Lisowska KA,Grabowski K,et al. Peripheral blood lymphocyte subpopulations in patients with bipolar disorder type Ⅱ[J]. Scientific Reports,2019,9 (1):5869.
[21] Becking Karlijn,Haarman Bartholomeus CM,Grosse Laura,et al. The circulating levels of CD4 t helper cells are higher in bipolar disorder as compared to major depressive disorder[J]. Journal of Neuroimmunology,2018,319:28-36.
(收稿日期:2021-03-19)