
Emotional intelligence and its impacts on the clinical performance of nurses in general public hospitals
2021-12-29 11:16DeldarMoradAdulahRasoulSariPiroYousifAliYaseen
Frontiers of Nursing 2021年4期
Deldar Morad Adulah*, Rasoul Sari Piro, Yousif Ali Yaseen
aCommunity Health Unit, College of Nursing, University of Duhok, Duhok, Duhok 42001, Iraq
bPsychiatric Nursing Unit, College of Nursing, University of Duhok, Duhok, Duhok 42001, Iraq
cInternal Medicine Department, College of Medicine, University of Duhok, Duhok, Duhok 42001, Iraq
Abstract: Objectives: The nursing profession is considered to be at a high risk of workplace stress, workload, and burnout due to the high job demands. The nurses require the appropriate and prompt coping mechanisms to relieve the effects of stress. The nurses have to be emotionally intelligent to overcome the work-related stress to meet the clinical-based duties. But there is a paucity of the effect of emotional intelligence (EI) on the clinical performance of nurses in the literature. Therefore, the role of dimensions of EI in the improvement of clinical performance of nurses was explored in this study.
Keywords: emotional intelligence • clinical performance • communication
1. Introduction
The function of nurses is considered to be a crucial part of health care teams. The reasons for this importance can be attributed to the role of nurses in establishing coordination for health care services and facilitating effective communication between staff, patients, and families. The nursing profession is considered to be at a high risk of workplace stress, workload, and burnout due to the high job demands. The job demands are workloads and health risks linked to direct contact with patients along with a bulk of administrative duties.1In this regard, nurses need to cope with high job- associated stress along with a high clinical burden. These stresses may cause harm and impact nurses’ well-being and their abilities to cope with job assignments. More than 40% of the nurses have moderate to severe levels of workplace stress.2A study conducted in this region reported that 83.60% and 4.50% of nurses have moderate and high stress levels, respectively.3
Given to inherence of the nursing profession, the nurses require the appropriate and prompt coping mechanisms to relieve the effects of stress. The nurses’responses to stressful events in terms of coping mechanisms are different based on individual varieties and organizational factors. Therefore, nurses have to be emotionally intelligent to overcome the work-related stress in order to accomplish the clinical-based duties.4
According to the APA Dictionary of Psychology, emotional intelligence (EI) assists a person in processing and using emotional information in reasoning and other cognitive actions. Based on Mayer and Salovey’s 1997 model, EI includes 4 abilities: identifying and evaluating emotions accurately; accessing and arousing emotions in facilitating cognition; understanding and using emotional language and information; and regulating one’s own and others’ emotions to promote growth and well-being.5
EI has received special attention in the nursing profession because it helps nurses to improve their well-being and impacts patients and families.6EI skills assist nurses in coping with the emotional demands of the health care environment. Emotional labor is widely accepted as a part of nursing work because nurses empathize highest quality of care for patients and show their humanity. Nurses need to manage their emotions to offer appropriate help and support. Emotions are important in creating and maintaining an appropriate environment to care for patients.7The ability to create a rapport with patients, manage their emotions, and better focus on the patients’ needs is essential to provide quality care.8Interestingly, a substantial relationship between social skills and clinical competence has been found among nurses.9
The existing literature has focused considerably on the relationship between EI and academic performance among nursing students. Academic performance, however, is quite different from job performance.10–12There is a paucity in the literature on the effect of EI on the clinical performance of nurses. A recent study conducted in this region has reported that nurses have a low level of EI.3In this regard, we aimed to examine the relationship between 5 dimensions of EI and clinical performance of nurses in this study.
We hypothesized that the levels of problem solving and interpersonal communication are regulated by appraisal of other nurses’ emotions and utilization of emotions in facing obstacles in clinical settings.
2. Methods
2.1. Study design and sampling
Nurses who were working in different hospitals across Duhok city were invited to participate in this crosssectional study. The nurses were invited from different hospital types, clinical departments, and working shifts.The sites were multi-specialty and comprehensive, and they included 1 general, 1 pediatric, 1 maternity, 1 emergency public hospital, and 1 cardiac center. The clinical settings were medical, surgical wards, and out-patient clinics; intensive care units (ICUs); cardiac care units(CCUs); operation rooms; and anesthesia settings of hospitals. The data collection was performed between November 2017 and January 2018.
The purposes of the study were explained to the subjects before filling out the questionnaire, personally or in small groups that included 2 or 3 persons. The data collection was performed in a calm and appropriate environment inside the hospital to avoid staff interruption. The total time required to fill out the questionnaire was only 15 min.
2.2. Eligibility criteria
The subjects met the eligibility criteria for the present investigation if they were men or women and if they were aged 18 years and older, regardless of sociodemographic aspects, education levels, and job rank.
The nurses who had an experience of <6 months were not included in the study because nurses have a rotating working schedule among different hospitals and clinical departments for the first 6 months of employment in this region. We excluded these nurses from the study due to the lack of stability during this time. Nurses with chronic medical conditions or any mental disorder were also excluded from the study. Therefore, of the 221 subjects invited, 19 nurses did not agree to participate and 8 nurses had >20% missing information. Finally,194 nurses were included in this study (response rate:87.78%).
2.3. Measurement criteria
The Brief Emotional Intelligence Scale (BEIS-10) was used to measure EI. It has been created based on the longer 33-item EI Scale (EIS). The BEIS-10 has 10 items that assess 5 distinct categories of EI. The categories include the appraisal of their own emotions, appraisal of others’ emotions, regulation of their own emotions,regulation of others’ emotions, and utilization of emotions. The items are rated on a 5-point Likert scale anchored based on the following scores: 1 = “strongly agree,” 2 = “agree,” 3 = “neutral,” 4 = “disagree,” and 5 = “strongly disagree.” The agreement score proportion for the items was from 89.20% to 96.40% within a ±1 range.13 The Cronbach’s alpha value of the 10 items for internal consistency was 0.753 in this study.
The clinical performance of the nurses was measured by an objective structured clinical examination(OSCE) scale.14It assesses clinical competence in a planned or structured way. This scale was used previously by Ross et al.15to measure clinical skill performance among nurses. Various components are measured by the OSCE, including obtaining clinical data (history taking and physical assessment), analyzing clinical data (problem identification and nursing diagnoses), and using clinical data (decision making and supportive, educative, or therapeutic nursing interventions). Each component is an objective of one of the OSCE stations. In this study, the nurses were asked to rate each item in terms of the extent to which it was important in their particular work environment on a 7-point scale: from 1 = “never required” to 7 = “critical.”The Cronbach’s alpha value of the 38 items for internal consistency was 0.945.
The Perceived Stress Scale (PSS) measured the perceived degree of stress experienced by a nurse.The tool has 10 items to determine how unpredictable,uncontrollable, and overloaded responders find their lives. The items ask the nurses about their feelings and thoughts over the last month. The PSS measures a special way that a person feels. Items are rated on a 5-point Likert scale anchored based on the following scores:0 = “never,” 1 = “almost never,” 2 = “sometimes,” 3 = “fairly often,” and 4 = “very often.” The scores for questions 4, 5,7, and 8 must be reversed as 0 = 4, 1 = 3, 2 = 2, 3 = 1, and 4 = 0, respectively. Subsequently, the scores of the items are summed to obtain a total score between 0 and 40.Higher scores indicate higher perceived stress. Scores ranging from 0–13, 14–26, and 27–40 are perceived as low stress, moderate stress, and high stress, respectively16. The Cronbach’s alpha value of the 10 items for internal consistency was 0.628 in this study.
The sociodemographic aspects of the nurses,including age, gender, residency, education level, and lifestyle, were collected through the self-report method.
2.4. Statistical analysis
The general characteristics of the nurses were presented in terms of means (standard deviation) or numbers (percentages). The levels of EI and dimensions of clinical performance were determined by using means (standard deviation). The prevalence of stress was determined by numbers (percentages). The role of the EI dimensions in regulating the clinical performance of the nurses was examined in a multivariate analysis model. In the multivariate analysis model, the dimensions of clinical performance were considered as dependent variables, and the dimensions of EI as independent variables. In the multivariate analysis model, the adjustment was made for age, gender, marital status, residency, smoking, physical activity, sleeping hours, family size, and stress score.
The comparison of teamwork scores between nurses with different educational levels and smoking status was examined with an independentt-test. In this study, the institute and bachelor certificates meant completing 2 years and 4 years at university, respectively.The correlation of the dimensions of EI with clinical performance and stress was examined in a bivariate regression analysis. The analyses in the regression were adjusted for age, gender, marital status,residency, smoking, physical activity, sleeping hours,family size, and stress score. A level of <0.05 was considered a statistically significant difference. The Statistical Package for the Social Sciences (SPSS), version 25.00, (IBM SPSS Statistics for Windows, version 25.0;IBM Corp., Armonk, NY, USA) was used for the data analysis.
3. Results
The mean age of the nurses was 29.44 years(SD= 4.01 years), with ages ranging between 23 years and 36 years. The mean family size was 6.81 (SD= 3.08).More than half of the nurses were men (56.70%), married (53.10%), living in urban areas (77.30%), nonsmokers (86.10%), physically active (55.70%), and irregular physically active (63.90%). The study revealed that 52.10% of them were normal sleepers (defined as 6–8 h of sleeping/24 h), followed by 31.40% of short sleepers (defined as <6 h of sleep) and 16.50% of long sleepers (>8 h of sleep), see Table 1. The nurses had no chronic diseases or psychiatric disorders, as indicated through a self-report technique.
The mean score of EI in the nurses was 2.56 of 5.0. The nurses appraised their own emotions (mean[M] = 1.95), but they were unable to appraise the emotions of other nurses (M= 3.20). They enabled to regulate their emotions (M= 2.33), but they were unable to regulate the emotions of other nurses (M= 2.59).Further, the nurses did not think that they could utilize their emotions in clinical settings (M= 2.72). Most of the nurses had a moderate level of stress (77.80%),followed by those with a low level (14.90%) and a high level (7.20%; see Table 2) of stress.
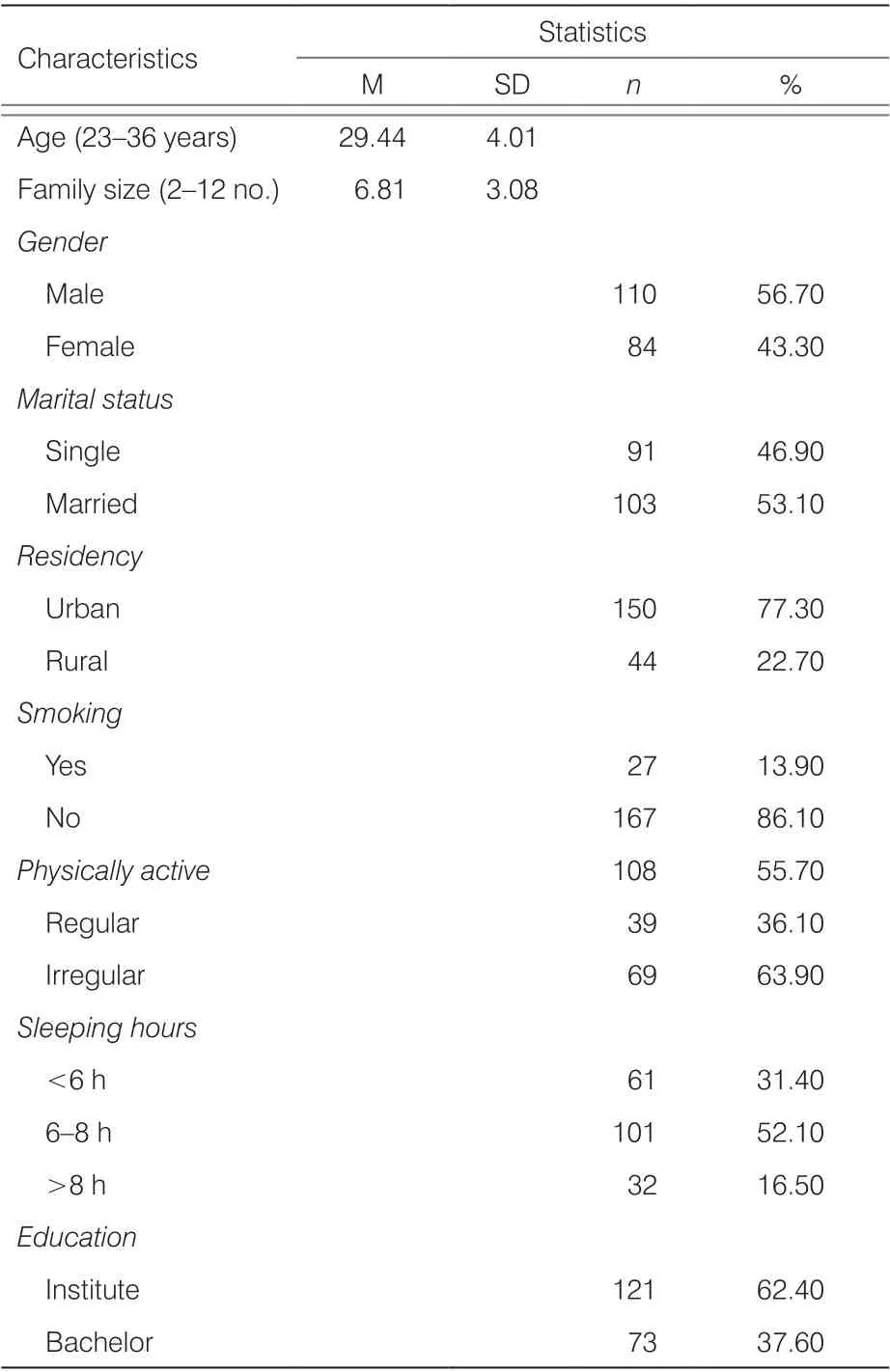
Table 1. General characteristics of nurses (n = 194).
Generally, the nurses reported that a little clinical performance is required (M= 3.42). They neither agreed nor disagreed with the contextual behaviors (M= 3.71).The nurses reported that professional and clinical skills were rarely required (M= 1.57 and 1.98, respectively). The following categories required a little clinical performance, including interpersonal communication(M= 3.65), problem solving (M= 4.06), professional ethics (M= 4.10), teamwork (M= 3.91), and leadership(M= 3.76) in clinical settings (Table 2).
In the multivariate analysis model, the dimensions of clinical performance were considered as dependent variables, and the dimensions of EI as independent variables. The study showed that teamwork was affected by education level (P= 0.006). In other words, the nurses with a bachelor’s level of education had a significantly greater mean score for teamwork compared to the nurses with an institute level (4.43 vs. 3.61;P< 0.001).A commitment to professional ethics was associated with smoking status (P= 0.016). In other words, nonsmoking nurses had a significantly higher mean score for professional ethics compared to smokers (4.16 vs.3.73;P= 0.013) (Tables 3 and 4).

Table 2. Emotional intelligence and perceived stress in nurses(n = 194).
Interpersonal communication and problem solving were correlated with an appraisal of one’s own emotions. Moreover, teamwork was associated with the regulation of others’ emotions, and problem solving was associated with utilization and stress scores (Table 3).The levels of interpersonal communication and problem solving were significantly improved with an increasing level of appraisal of one’s own emotions (r= −0.263,P< 0.001 andr= −0.241,P= 0.001, respectively).The mean scores of interpersonal communication and teamwork were improved with increasing levels of regulation of others’ emotions (r= −0.591,P< 0.001 andr= −0.527,P< 0.001, respectively). Moreover, the level of problem solving improved with greater utilization of emotion in clinical settings (r= −0.358,P< 0.001). The stress level of the nurses increased with a decreasing level of utilization of emotions (r= 0.368,P< 0.001;Table 5).

Table 3. Role of emotional intelligence dimensions on the clinical performance of nurses (n = 194).
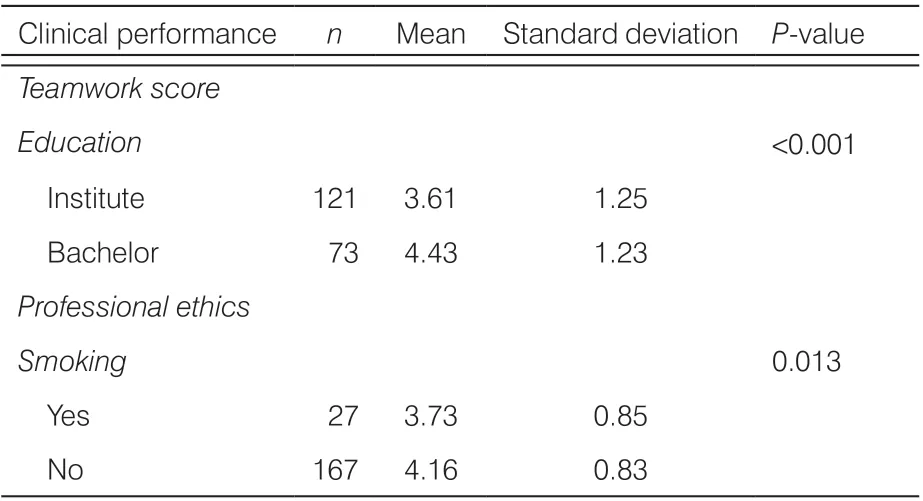
Table 4. Comparison of teamwork score between nurses with different educational levels and smoking status (n = 194).
4. Discussion
We hypothesized that the levels of problem solving and interpersonal communication are regulated by appraisal of other nurses’ emotions and utilization of emotions in facing obstacles in clinical settings. The results of this study did not approve our first hypothesis. This is because the study has indicated that the interpersonal communication and problem-solving abilities of the nurses were enhanced with an increasing level of appraisal of their own emotions. However,the study approved our second hypothesis as the level of problem solving was improved with the greater utilization of emotion. The stress level of the nurses also increased with a decreasing level of utilization of emotion.
4.1. First hypothesis: appraisal of one’s own and others’ emotions in relation to communication skills
A cross-sectional study was conducted in 2 populations comprising patients admitted to 3 hospitals. The study showed that nurses’ job satisfaction and communication skills have a mediating role in EI and service quality.17In other words, nurses with a high capacity of intelligence were expected to deliver more qualified health care and health-related services. In agreement with this study,we showed that interpersonal communication, including expressions of enthusiasm for nursing work, cooperating with the supervisor nurse, and behaving in a friendly manner, was improved with an appraisal of one’s own emotions. In addition, the problem-solving abilities of the nurses, including identifying sudden changes related to the patient’s condition, quickly solving clinical problems,and taking the initiative to solve a work-related problem,improved with the enhanced appraisal of their own emotions. It seems that when the nurses critique their own emotions and those of others, they establish a basis of understanding to identify those styles that are more suitable in communicating with other nurses or their supervisors.18
We did not examine the mediating role of communication skills in the relation between EI and service quality since service quality was not measured in this study. However, EI is important to nurses owing to its effect on communication skills. Importantly, the perceptions of patients toward their health care highly depend on the quality of their interactions with theirhealth care providers, including nurses, doctors,and the medical team.19,20Furthermore, the connection that a patient feels with a clinician can ultimately enhance their health status by promoting participation in their care, adherence to therapy, and patient self-management.20–23

Table 5. Correlation of dimensions of emotional intelligence with clinical performance and stress.
Derived from Gardner’s24idea of multiple intelligences, EI involves an individual’s ability to “monitor their own and others’ emotions, to discriminate among them,and to use the information to guide thinking and actions.”Hence, we can understand from the nurses who participated in this study that they appraised their own and others’ abilities to appropriately communicate with other nurses, patients, and supervisors. But we hypothesized that appraising others’ emotions has a role in regulating interpersonal communication with patients and nursing supervisors. The relationship between EI and clinical skills has been reported elsewhere.25Stratton et al.25have indicated that the “attention to feeling” subscale of EI and the “perspective-taking” and “empathic concern”subscales of empathy were associated with communication skills among clinical students. In this case, the“attention to feelings” subscale assessed the extent to which the student adhered to the verbal and nonverbal appraisal and expression of emotions. Accordingly, an improvement in clinical skills could result in enhanced teamwork in nurses.
Self-awareness provides a road map for a person to adjust the job, motivate oneself and others, and assess the feelings of others to effectively lead and motivate others.26People with the abilities of self-awareness and appraisal of others’ emotions can recognize and identify what their emotions are and how to apply these emotions to improve their relationships with other individuals.27
We showed in this study that communication skills can be managed through enhancing the skills of nurses in appraising their own emotions. But this kind of relationship was not found for the appraising of others’emotions. We refer to this as a weakness of the nurses because the nurses who participated in this study were unable to appraise the emotions of other nurses.
4.2. Second hypothesis: regulation of others’emotions in relation to teamwork
We found that teamwork in nurses was improved through the regulation of others’ emotions in agreement with our hypothesis. The teamwork in this study included cooperating with the other members of the team, engaging responsibly in meetings and group activities, giving feedback to colleagues in a constructive way, and engaging in and contributing to research-based practices. Cadman and Brewer28have determined the key EI competencies required for nurses to succeed in health settings. These competencies are the ability to work collaboratively with interdisciplinary teams,the ability to recognize and respond to one’s own and others’ emotions (self-awareness), and the ability to motivate other nurses in clinical aspects.28Emotional competencies have been defined as critical for the future success of nurses in health settings. Strickland29determined the following emotional competencies as essential for the nursing profession: “self-awareness,self-management and emotional self-control, [and] relationship management competencies such as empathy and teamwork.” These competencies lead to increased profitability, patient satisfaction, motivation, and cooperation of co-workers.29
4.3. Emotion appraisal and utilization in relation to problem solving
The present study found that competence in problem solving improved with improvements in the abilities of nurses to appraise and utilize their own emotions. The problem solving items were assessing their ability to identify sudden changes related to the patient’s condition, solving speedy clinical issues, and taking the initiative to solve a work-related problem. Rao30reported that accurate appraisal and discernment of patient emotions have a positive effect on the quality and accuracy of history taking and diagnosis. When medical practitioners can better understand the emotional reactions of patients and make recommendations for therapeutic plans and lifestyle modifications, they can understand why some interventions are more or less suitable for patients and make a suitable intervention plan. The effectiveness of emotion appraisal and its utilization in problem solving, especially for patients with medical conditions, could be due to its effect on burnout.31
Akerjordet and Severinsson32reported that EI in nurses is associated with more positive attitudes, greater adaptability, and improvement in the relationship between nursing staff and their patients. EI correlates with problem solving in nurses because higher EI is associated with higher improved overall cognitive-based performance that is essential for problem solving.33Also, higher EI competence is associated with decreasing stress levels34, as also shown in this study.
EI dimensions were not correlated with leadership skills in this study. The leadership skills include motivating other nurses, coaching others in duties, having supervisor attributes, and helping beginning-level nurses with their entry to practice. The possible reason is the nurses who were included in this study had similar levels of EI3since they were hesitant about assessing leadership in terms of clinical performance (M= 3.76;SD= 0.82). Another study has shown that nurse supervisors with high EI scores can adapt their leadership style to meet the needs of the staff.35Other similar investigations on nursing leadership and EI have reported that EI is positively associated with staff adaptation in terms of change and the improvement of interdisciplinary links and patient satisfaction.36,37
Conclusions
The present investigation showed that the appraisal of one’s own emotions improves interpersonal communication and problem-solving skills in nurses.The appraisal of others’ emotions improves interpersonal communication and teamwork. Besides, the utilization of emotions enhances nurses’ problem-solving abilities concerning medical issues.
Recommendations
We suggest that nurses be educated on how to regulate others’ emotions and positively utilize these emotions to face obstacles in medical settings. But we need to take into consideration the limitation that EI cannot be quickly developed exclusively through interpersonal skill training. Therefore, it is required that nurse educators develop assessment strategies to identify EI in the recruitment process.28In other words, nurses need to know how to regulate others’ emotions and positively utilize these emotions to make a positive communication in medical settings.
Ethical approval
The ethical approval of the present study was obtained from the local health ethics committee in Duhok with the following registered reference number: 12072017-5(on July 12, 2017). The authors obtained a written consent form from all nurses. The nurses’ right to refuse participation was protected in this study. A guarantee of confidentiality of the obtained information was given to nurses at the time of publication.
Conflicts of interest
All authors have nothing to disclose.
- Frontiers of Nursing的其它文章
- Predictors of nurse’s happiness:a systematic review
- Redefining the concept of professionalism in nursing: an integrative review
- Clinical nursing competency assessment:a scoping review
- Moderating effect of psychological resilience on the perceived social support and loneliness in the left-behind elderly in rural areas†
- Effects of progressive muscular relaxation and stretching exercises combination on blood pressure among farmers in rural areas of Indonesia: a randomized study†
- Visualization analysis of research“hot spots”: self-management in breast cancer patients†