
A review of obstacles and facilitating factors of implementing Clinical Ladder Programs in nursing
2022-02-15 04:54SiQiXiongJieLiSiLiLiPingChenYuanTingYan
Nursing Communications 2022年13期
Si-Qi Xiong,Jie Li,Si Li,Li-Ping Chen,Yuan-Ting Yan
1 Department of Nursing,Yan’an Hospital of Kunming City,Kunming,650051,China.
Abstract Clinical Ladder Programs is to develop different training programs according to different levels of nurses’ management. The purpose is to improve nurses’ sense of professional identity, professional and technical capabilities, and determine salary levels, so as to fully mobilize nurses’ enthusiasm. This article reviews the current status of the application of Clinical Ladder Programs in clinical nursing around the world, and understands the obstacles and facilitating factors that affect the implementation of Clinical Ladder Programs,in order to provide a reference for establishing a perfect hierarchical nurse training model in China.
Keywords: Clinical Ladder Programs, Nursing management, Obstructive factors,Facilitating factors
Introduction
After entering the hospital, nurses still need to continue to receive on-the-job training, including clinical skills, management, scientific research, education and other contents, which is conducive to nurses to update relevant knowledge, improve their own career planning,and enhance their core competitiveness [1]. As the advancement of quality nursing services, nurse training methods have shifted to competency-based layered training [2]. Clinical Ladder Programs refer to the development of different training Programs according to different levels of nurses. The "Framework from novices to experts"proposed by Benner in 1984 is the basis of the Clinical Ladder Programs. A relatively complete Clinical Ladder Programs system has been established in the United States [3]. This program has also been widely applied by domestic and foreign researchers in the training of nurses in pediatrics, cardiothoracic surgery, ICU, orthopedics and other departments [4-6]. This program is conducive to improving the professional identity and skills of nurses. With the promotion of quality nursing services, the training method of nurses has also shifted to competency-based layered training [7]. However, studies have shown that clinical nurses are not satisfied with the current Clinical Ladder Programs and the participation rate is low. Clinical nurses believe that hospitals should provide more reasonable and clear ClinicalLadderProgramsmethodstopromotenurses'self-improvement [8, 9]. Therefore, this paper summarizes the current situation of the application of Clinical Ladder Programs in clinical nursing at home and abroad, to understand the obstacles and promoting factors affecting the implementation of Clinical Ladder Programs, in order to provide reference for the establishment of a perfect hierarchical nurse training model in China(Figure 1).
Overview of Clinical Ladder Programs
Clinical Ladder Programs are the basis of the position management of nursing staff, and the Clinical Ladder Programs of nursing staff is an inevitable requirement for the implementation of the position management of nurses. The establishment of the level system of nursing staff is an important measure to stabilize the nursing team and an important link to implement the long-term mechanism of high-quality nursing service [7]. Energy level promotion plan is defined as a nurse promotion plan which gives different vocational knowledge and training tasks according to the position of nursing staff, and promotes them to the next level after passing the assessment,and then carries on the new stage of training and learning.Clinical Ladder Programs (CLP) refers to the promotion method of clinical nurses designed by nursing leaders. The purpose is to improve the clinical skills and abilities of nurses while reducing the turnover rate of clinical nurses.In 1972, Zimmer [10] proposed that identifying and motivating nurses through clinical ladder would help reduce the turnover rate of nurses and improve their satisfaction. Since then,clinical ladder program has been used to promote the development of nursing profession. In 1984, Benner [11] proposed the framework of"from novice to expert" and believed that the clinical progression mode should go through five stages. For example, novice, advanced beginner, competent, proficient and expert, nurses gain corresponding knowledge and confidence at different stages through formal training to improve their professional skills. This framework has been used by many institutions as the basis for designing clinical ladder plans, not only to improve the clinical skills of nurses, but also to promote the scientific research ability of nurses [12].
Stratified training status of clinical nurses
Researchers at home and abroad have constructed a hierarchical training system for nurses based on the Clinical Ladder Programs to improve the practical skills of nurses, promote the promotion of nurses and reduce their attrition rate. There are differences in stratification, training content, promotion methods and years of nurses in different countries and regions, such as: Most American take 3-5 N layered management, hospital nurses after corresponding levels of training learning could satisfy the requirement of education,working years, will be able to apply for promotion to the hierarchical management committee, at the same time submit letters of recommendation, the self-assessment report, work plan, etc., after the promotion level promotion [13]. The national university of Singapore,according to the request of the ministry of health from Singapore will nurse nine grades are divided into three levels,and in accordance with the education, working years, and determine the nurse's promotion system training completion, from the lowest level (grade 2B low qualification registered nurse Ⅱ) promotion to 4B care experts,bachelor's degree in the shortest possible work eight years can be achieved, One year of work for master's and doctor's degree can lead to level 4B [14]. Nurses in Australia are divided into nurse assistant,enrolled nurse, junior registered nurse, registered nurse and practical nurse according to their educational background and work experience.Nurses at each level have clear educational requirements and responsibilities. They can achieve promotion by completing corresponding training and learning at each level. In Japan, nurses are divided into clinical nursing experts, specialist nurses and life nurses according to their educational background, nursing practice ability and work experience. Nurses at different levels can be promoted through regular training and assessment, and they can be promoted to specialist nurses in about 8 years [15].
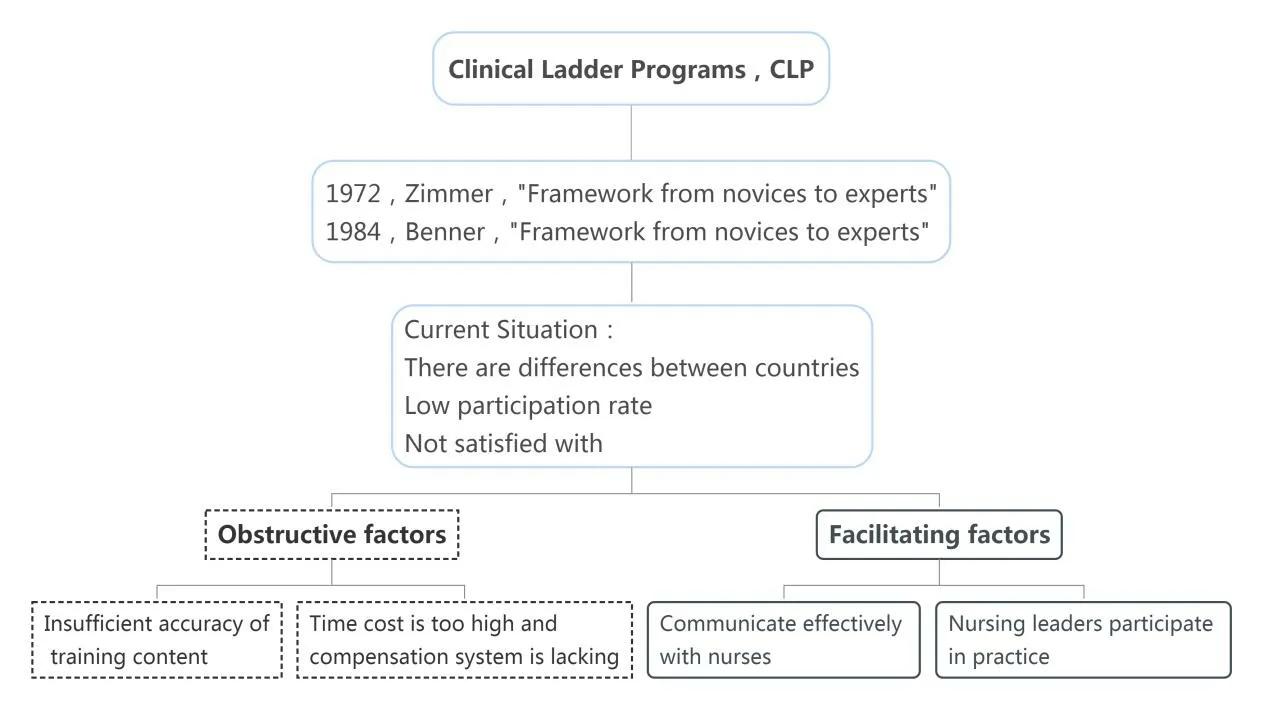
Figure 1 Overview of this research
Notice on Further Strengthening the Nursing Work of Medical Institutions from the National Health Commission of the People's Republic of China clearly requires that nursing post management should be implemented and a job-based employment evaluation,training and cultivation, professional title promotion, performance appraisal and salary distribution system should be established to stimulate the vitality of the nurse team [16]. Most hospitals, such as hospitals in Fujian Province and Jiangsu Province, will divide nurses into N0-N4 or N1-N5 levels according to their working years,educational background and professional title. The admission standards, training objectives and assessment standards of nurses at each level are formulated. Training manuals are prepared according to different departments and levels, and regular assessment is conducted.Promote the improvement of nurses' ability and complete the promotion among nurses' levels [5,17].
At present, a relatively perfect management mode of nurse Clinical Ladder Programs has been established at home and abroad, but some nurses are not satisfied with the current Clinical Ladder Programs,and the participation rate is low [8]. Therefore, summarizing the factors hindering the implementation of Clinical Ladder Programs and exploring its promotion factors is one of the key issues of research attention.
Obstacles to the application of Clinical Ladder Programs
The content of layered training is not accurate enough
Nurses of different levels have different requirements for training content, so training emphases for nurses of different levels are different [18]. There are, however, investigation shows that clinical nurses and nursing leaders have differences in cognitive Clinical Ladder Programs: only 28.6% of the nurses agreed Clinical Ladder Programs to improve their ability of nursing practice, and more than half (55%) of nursing leaders believe in Clinical Ladder Programs did raise the level of the practice of clinical nurses[9].As a result,nursing leaders are not careful enough to take into account the needs of nurses at different levels when developing the hierarchical training content based on the Clinical Ladder Programs. If the hierarchical training content is not refined enough, the enthusiasm of nurses with strong ability to participate in the training will be reduced, and nurses with weak ability will fall behind the progress of the training [7]. Carrier proposed that the job satisfaction of nurses can be effectively improved and the career promotion of nurses can be promoted if the energy Clinical Ladder Programs can be formulated based on the actual needs of clinical nurses [19]. The researchers found that although a large number of hospitals are implementing Clinical Ladder Programs, the promotion of nursing staff reduces their turnover rate. However, most of the research content is formulated on the basis of the lowest level of evidence, which cannot provide evidence to guide the best implementation practices. The content of nurses' hierarchical training cannot meet their actual needs, and it is difficult to achieve the purpose of improving the practical ability of clinical nurses, and the participation rate of the Clinical Ladder Programs is also not up to expectations [20]. Moreover, Geri-Anne et al. proposed that the Clinical Ladder Programs should be a process of continuous improvement, and managers should constantly improve the Clinical Ladder Programs system based on clinical practice and in combination with evidence and research [21].
High time cost and lack of compensation system
A number of studies have shown that clinical nursing workers believe that excessive time investment is the main obstacle to the implementation of Clinical Ladder Programs [8, 20, 22]. Zehler et al.,by using the method of focus group interview to 35 registered nurses,found that clinical nurses believe that participating in the energy-level advancement program requires a lot of training and learning, and frequent meetings, occupying clinical work time, resulting in decreased patient satisfaction [8]. As patients' acuity becomes more and more complex, although the intensity of clinical nursing is also increasing, nurses are rarely able to carry out training and learning during normal working hours, which generally occupy the time of nurses' daily rest [23]. However, after nurses spend a lot of time to complete the training of Clinical Ladder Programs, the hospital only provides low salary compensation [8]. Although some studies suggest that the degree of compensation will change with the progress of the project, many participants believe that the compensation is not proportional to the amount of work required for the progress of the project [12, 22]. Korean researchers investigated the expectation level of nursing staff in small and medium-sized hospitals on Clinical Ladder Programs, and found that nurses at different levels had inconsistent expectations on salary, suggesting that appropriate salary compensation system should be established to compensate nurses for the time and energy they spent in Clinical Ladder Programs [24].
Promoting factors for the application of Clinical Ladder Programs
Communicate effectively with nurses
Communicating with caregivers about the changes to the Clinical Ladder Programs program is a key factor in the successful implementation of the Clinical Ladder Programs program. Effective information transmission and communication can improve employees'confidence, enthusiasm and dedication, and help reduce the incidence of resignation, leave and absenteeism [25]. Research and experience show that clinical nurses have their own views and opinions on existing or potential problems in clinical work, but they may reserve their own views for various reasons,resulting in organizational silence[26]. Organizational silence can avoid direct conflict between organizations and individuals to a certain extent, but it will have a negative impact on organizational learning and innovation behavior,so that leaders cannot get real feedback [27]. Susan et al. [28] found that when the hospital implemented a hierarchical training system for nurses based on the Clinical Ladder Programs for a long time, the system was not well applied due to the lack of effective participation and follow-up investigation and maintenance. Therefore, the research team revised the hospital's Clinical Ladder Programs: Established a shared governance committee and MAPP club; Held an information collection meeting to understand nurses’ opinions on stratification;Actively communicated with clinical nurses; Announced the plan revisions on the hospital's intranet and canteens. These methods have increased the participation rate and core competence of the nurses'Clinical Ladder Programs, and at the same time promoted the progress of the Clinical Ladder Programs of specialist nurses. Knoche et al. [9]revised the original Clinical Ladder Programs and invited more than 115 clinical nurses for thematic discussion through focus group interview, which promoted the further improvement of Clinical Ladder Programs and built nursing literacy tools for clinical implementation.
Participation of nursing leaders in practice
The leadership behavior of nursing leaders is related to nursing culture and nurse work involvement [29]. Head nurses' participation in clinical practice can promote clinical nurses' understanding of Clinical Ladder Programs, better grasp the assignment of each part of Clinical Ladder Programs, and promote the effective implementation of Clinical Ladder Programs in clinical practice[9].The study of Liu et al.[30] showed that the head nurse patiently listening to the problems and needs of clinical nurses in nurse-patient communication and occupational positioning can not only improve the level of mental resilience of nurses, but also improve the organizational climate of pediatric nurses and reduce the occurrence of hidden absenteeism. In addition, Mensik et al. [31] found through the importance of nursing leaders' active participation in practice that both nursing leaders and clinical nurses should clearly understand the advantages of the energy level advancement plan that can promote the professional development of clinical nurses. The responsibilities and work of clinical nurses should be considered when formulating the goals of the energy level advancement plan, so as to promote the promotion of nurses.
Summary
The implementation of Clinical Ladder Programs in clinical practice can effectively improve the clinical practice ability of nurses, and provide motivation and direction for the promotion of clinical nurses.However, the implementation of Clinical Ladder Programs in clinical practice still faces some problems, such as insufficient precision of layered training content, high time cost and lack of compensation system. In the future, researchers should focus on these problems,strengthen the communication between nursing managers and nursing staff, continuously improve the level of intensive care, seek for the level of practical plan to promote the progress and development of nursing management.
 Nursing Communications2022年13期
Nursing Communications2022年13期
- Nursing Communications的其它文章
- Delphi and Analytic hierarchy process for the construction of a risk assessment index system for post-stroke shoulder-hand syndrome
- Spiritual health, empathy ability and their relationships with spiritual care perceptions among nursing students in China:A cross-sectional correlational study
- Qualitative study on influencing factors of refusal of gastric tube placement in stroke patients with dysphagia
- The influence of professional identity and ageism on turnover intention in nursing homes: a cross-sectional study from suzhou, China
- The relationship of family separation and nutrition status among under-five children: a cross-sectional study in Panti Public Health Center, Jember Regency of East Java, Indonesia
- Nursing cooperation related to thoracoscopic surgery in children