
Sperm DNA fragmentation does not affect the clinical outcomes in the cumulative transfers of an ICSI cycle along with blastocyst transfers in couples with normozoospermic male patients
2022-06-11 08:33DeepthiRepalleSarithaShilpaBhandari
Deepthi Repalle, Saritha K.V., Shilpa Bhandari
1Department of Reproductive Medicine and Surgery, Sri Aurobindo Institute of Medical Sciences, Indore, Madhya Pradesh, India
2Department of Biotechnology, Sri Venkateswara University, Tirupati, Andhra Pradesh, India
ABSTRACT
Objective: To know whether sperm DNA fragmentation (SDF)affects the clinical outcomes in the cumulative transfers of an intracytoplasmic sperm injection (ICSI) cycle along with blastocyst transfers in couples with normozoospermic males.
Methods: The study included 252 couples who underwent their first ICSI cycles along with blastocyst transfer and whose male partner semen samples were normozoospermic according to the World Health Organization 2010 criteria. All the couples were classified into two groups based on the SDF: the low SDF group (SDF≤30%,n=162) and the high SDF group (SDF>30%, n=90). Clinical as well as laboratory outcomes were correlated between the two groups.Sperm DNA fragmentation was assessed on the post-wash semen samples by acridine orange test. The main outcome measures were the live birth rate and miscarriage rate.
Results: A significant decrease in the live birth rates was observed in the high SDF group compared to the low SDF group in fresh embryo transfer cycles (P<0.05). However, no significant difference was observed in the clinical outcomes either in the frozen embryo transfer cycles or in the overall cumulative transfer cycles (P>0.05).No significant difference was observed in the laboratory outcomes between the two SDF groups. A remarkable decrease in sperm motility was observed in the high SDF group compared to the low SDF group (P<0.05).
Conclusions: Sperm DNA fragmentation does not affect the clinical outcomes in the cumulative transfers of an ICSI cycle along with blastocyst transfers in couples with normozoospermic males.
KEYWORDS: Sperm DNA fragmentation; Intracytoplasmic sperm injection; ICSI; Live birth rates; Blastocyst transfer;Cumulative transfers
Significance
Various studies have shown the negative effect of sperm DNA fragmentation (SDF) on clinical outcomes. Most studies correlated SDF with clinical outcomes in fresh embryo transfer cycles. Meanwhile, the success of artificial reproductive technology depends on the cumulative cycles where both fresh and frozen embryo transfer cycles are included. In this study,we showed that SDF did not affect the clinical outcomes in the cumulative transfers of an ICSI cycle along with blastocyst transfers in couples with normozoospermic male patients.
1. Introduction
Infertility affects around 15% of couples of reproductive age[1].Male factor infertility is estimated to be 40%-50% of infertility cases around the globe, defined by the alteration of at least one of the standard semen parameters recognized by the World Health Organization (WHO)[2]. However, standard semen parameters may not predict the fertility potential of males as around 15% of the infertile men have normal semen parameters according to the WHO reference ranges. Traditional semen analysis cannot predict sperm abnormalities at the DNA level, which may be the reason for the male factor infertility[2].
Newer techniques have been developed to know the sperm at the molecular level. Sperm DNA fragmentation (SDF) assessment by acridine orange test is one of the tests that assess the integrity of the sperm DNA based on the susceptibility of the DNA to denaturation[3]. The acridine orange stain differentiates the sperm with normal double-stranded DNA (green fluorescence)and abnormal denatured or single-stranded DNA (orange-red fluorescence) with the help of metachromatic shift properties of the stain[4,5]. Acridine orange test is a simple and affordable test for the assessment of DNA integrity in infertile men[4,5]. Clinical assessments of SDF need to be performed on the total motile fraction of sperm rather than raw ejaculate sperm by acridine orange test, as the raw semen carries a huge number of degenerated and dead sperm with damaged DNA[6].
The mature spermatozoa does not possess the capacity to repair their DNA as transcription and translation are halted. However,oocytes can repair SDF to some extent depending on the oocyte quality[7,8]. Age swaps the gene expression patterns in cumulus cells which are essential for oocyte quality[9]. In mature human oocytes, genes involved in cell cycle regulation, oxidative stress,and DNA repair are all affected by female age[10]. Hence, female age is one of the crucial factors affecting oocyte quality[11]. The study is mainly aimed to know whether SDF affects the clinical outcomes in the cumulative transfers of an intracytoplasmic sperm injection (ICSI) cycle along with blastocyst transfers in couples with normozoospermic males.
2. Materials and methods
2.1. Study population
A total of 252 couples whose male partners’ semen samples were normozoospermic according to WHO 2010 criteria, undergoing their first ICSI cycles along with blastocyst transfers between February 2017 and December 2019 were included in this study. Patients with altered semen parameters on the day of oocyte pickup, patients with life-threatening diseases, ICSI with vitrified/thawed oocytes, donor oocytes, preimplantation genetic testing, cryopreserved sperm, were excluded from this study.
The causes of infertility were an ovarian factor in 48, tubal factor in 46, endometriosis in 23, polycystic ovary syndrome in 25,unexplained in 45, and mixed in 65 patients. All the patients of ICSI cycles were categorized into two groups based on the SDF rates[3]:1) the low SDF group (SDF ≤30%, n=162) and 2) the high SDF group (SDF >30%, n=90). Clinical as well as laboratory outcomes were correlated between the two groups.
2.2. Controlled ovarian stimulation
In all patients, controlled ovarian stimulation was attained by recombinant follicle-stimulating hormone (r-FSH) (Recagon, MSD;Gonal-F, Merck) or human menopausal gonadotropin (HMG)(Gynogen, Sanzyme; Materna HMG, Emcure) starting from day 3 of the cycle. The pituitary function was suppressed either by gonadotrophin-releasing hormone (GnRH) agonists (Luprorin, Intas)in long stimulation protocol or GnRH antagonists (Cetrorelix Acetate, Emcure) in antagonist stimulation protocol. Recombinant human chorionic gonadotropin (r-HCG) (Ovidrel, Merck) was administered when three or more follicles reached a diameter of≥17 mm, and appropriate serum estradiol values were detected.Transvaginal oocyte retrieval was performed 35 h post trigger with HCG (Figure 1).
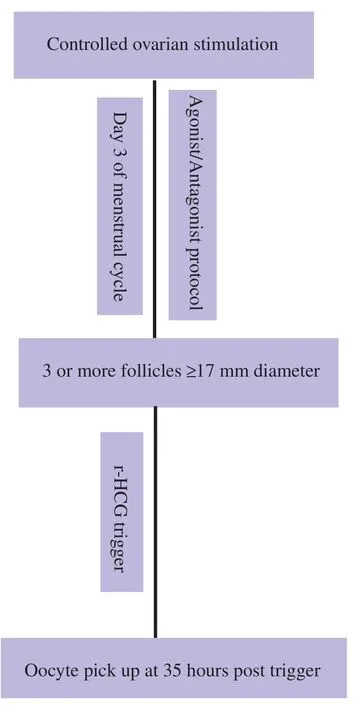
Figure 1. Flowchart of controlled ovarian stimulation procedure.
2.3. Embryo transfers
In patients for fresh embryo transfer, after oocyte retrieval micronized progesterone was administered daily vaginally (Crinone 8% gel, Merck.) and intramuscularly (Hald 100 mg, Intas) on alternate days till the pregnancy test was confirmed negative or continued for another 3 months if the pregnancy test was positive.Patients with optimum endometrial lining and thickness (>7 mm)on the day of ovulation trigger underwent fresh embryo transfer,otherwise transfers were canceled.
In patients for frozen embryo transfer, oral estradiol valerate(Evadiol, Intas) was used in a step-by-step increasing dose pattern for the preparation of endometrium. Endometrial lining and thickness were observed regularly prior to embryo transfer. Patients with optimum endometrial lining and thickness (>7 mm) underwent embryo transfer, otherwise transfers were canceled. Micronised progesterone (Crinone 8% gel, Merck) was administered daily vaginally and intramuscularly (Hald 100 mg, Intas) on alternate days and continued till the pregnancy test was confirmed negative or continued for another 3 months if the pregnancy test was positive.
2.4. Semen analysis and processing
Patients were advised to collect semen samples in sterile, non-toxic containers by masturbation after sexual abstinence of 2-3 days. After 30 min of liquefaction, samples were evaluated for count, motility,and morphology according to WHO 2010 criteria[2]. Semen samples were prepared by two-layer density gradient (Ⅴ-Grad 80%-40%,Vitromed, Germany) centrifugation for ICSI. The post-wash sample was used for SDF evaluation by acridine orange test.
2.5. Acridine orange test
The SDF was assessed by the acridine orange test method[4].Smears with 10 μL of post-wash samples were prepared and airdried. Carnoy’s solution (methanol: Glacial acetic acid, 3:1 vol/vol)was used in fixing the slides overnight. The staining solution was prepared daily from the stock solution of acridine orange (1 g/L in distilled water, stored in dark at 4 ℃) in the mentioned ratio of 10 mL of stock solution, 40 mL of 0.1 M citric acid, and 2.5 mL of 0.3 M Na2HPO4.7H2O and pH adjusted to 2.5. Slides were stained with the above stain for 5 min and rinsed in distilled water and covered with coverslips.
SDF was assessed using a fluorescence microscope (Olympus C× 31, Japan) under oil at ×1 000. Sperms with green fluorescence indicate normal intact DNA, whereas orange indicates fragmented sperm[4,12]. At least 400 spermatozoa were assessed in each slide of the replicates to calculate the average SDF. Slides were fixed on the very same day of ICSI and SDF was evaluated on next day using the acridine orange test. One highly skilled and trained andrologist evaluated all the slides for consistency and to prevent interpersonal variability. Each stained slide was observed right away after staining to reduce the variation of fluorescence intensity.
烟草在制品的含水率和相对湿度的关系通常以等温吸湿性表示,即烟草在制品在一定温度条件下与各种不同的相对湿度的相应平衡含水率数值。因为烟草在制品与周围空气湿度达到平衡状态时,吸湿速率就变得极其缓慢,所以计算平衡含水率数值必须经过足够的时间后才能进行,然后将得出的结果绘成一条曲线,这条曲线就称为等温吸湿线。烟草在制品的含水率随空气相对湿度变化而变化,但这种变化不是按一定比例的。试验结果表明,当相对湿度在10%以下时,烟草在制品的平衡含水率变动很显著;10%~50%时,变化幅度较小;50%以上尤其在80%~100%时,变化则很大。
2.6. ICSI
Oocytes recovered were incubated in culture media (Onestep,Vitromed, Germany) for 1-2 h before denudation by hyaluronidase enzyme (Hyadase 80IU, Vitromed) at 37 ℃ with 6% CO₂, 5% O₂ and the rest N₂. All the ICSI procedures were performed by a highly-skilled embryologist according to Palermo et al[13]. A morphologically normal sperm was selected and immobilized in polyvinylpyrrolidone (7%, Vitromed). The immobilized sperm was aspirated tail-first into the injection pipette and injected into the oocyte by aspirating a little cytoplasm before releasing the sperm into the oocyte. 16-18 h post ICSI, the appearance of two pronuclei with a second polar body extrusion was noted to evaluate the fertilization. The obtained embryos were cultured till day 5 post-ICSI for embryo transfer or vitrification.
2.7. Embryo grading
Day 5 blastocysts were graded according to Gardner et al[14].Expansion of the blastocysts was graded as 3-6, and trophectoderm,and inner cell mass were graded as A, B, and C. Expansion of blastocyst was graded as follows: 3-full blastocyst, 4-expanded,5-hatching, and 6-hatched. Whereas for trophectoderm: grade A-trophectoderm with many cells forming a cohesive epithelium;grade B-trophectoderm with few cells forming a loose epithelium and grade C-trophectoderm with very few cells. Similarly, for inner cell mass, grade A-tightly packed inner cell mass with many cells;grade B-loosely grouped inner cell mass with many cells and grade C-inner cell mass with very few cells. A blastocyst with an expansion of more than grade 3 and trophectoderm and inner cell mass with grade A or B was considered a good quality blastocyst.
2.8. Clinical follow-up
On day 5, one or two embryos were transferred using a soft catheter(Cook, Australia). SerumβHCG was observed after 14 days of the transfer to confirm the pregnancy test positive. An intrauterine sac with the presence of a fetal heartbeat was considered a clinical pregnancy. Miscarriage was defined as a pregnancy loss after detection of an intrauterine pregnancy by ultrasound before 20 weeks. The live birth rate was calculated as the presence of a live birth (either single or multiple live births) after an embryo transfer cycle.
2.9. Statistical analysis
The statistical analysis was executed in the Statistical Package for the Social Sciences (SPSS, IBM) for windows version 26.0.Categorical variables like clinical outcomes between groups were shown as proportions and scrutinized using Chi-square test. Characteristics of patients between groups were shown as continuous variables which were represented as mean±standard deviation (mean±SD) and scrutinized using the unpaired t-test.Multivariable analysis was performed using logistic regression for clinical outcomes to predict the effect of SDF on clinical outcomes in ICSI cycles of couples whose male partners’ semen samples were normozoospermic. Statistical significance was set at P<0.05.
2.10. Ethics approval statement
This study was approved by the Institutional Ethics Committee (No.SAIMS/IEC/2017/02/03). Written consent was obtained from all the couples.
3. Results
3.1. Female patient characteristics between the low and high SDF groups
No significant difference was observed in the female age, number of oocytes retrieved, number of mature metaphaseⅡ oocytes, total FSH administered and peak estradiol levels at ovulation trigger between the low and high SDF groups except for the female body mass index (BMI) (Table 1).

Table 1. Female patient characteristics between the low and high SDF groups.
3.2. Embryological outcomes between the low and high SDF groups
Similarly, no significant difference was observed in the embryological outcomes like fertilization rates, cleavage rates,blastocyst rates, good quality blastocyst rates, and the number of embryo transfer cycles between the two SDF groups (Table 2).

Table 2. Embryological outcomes between the low and high SDF groups.
3.3. Male patient characteristics and semen parameters between the low and high SDF groups
No significant difference was observed in the male age and semen parameters like volume, count, and morphology between the two SDF groups. A significant difference was observed in the sperm motility (P<0.05) and SDF (P<0.001) rates between the two SDF groups (Table 3).

Table 3. Male patient characteristics and semen parameters between the low and high SDF groups.
3.4. Clinical outcomes between the low-SDF and high-SDF groups in the ICSI cycles of normozoospermic male patients
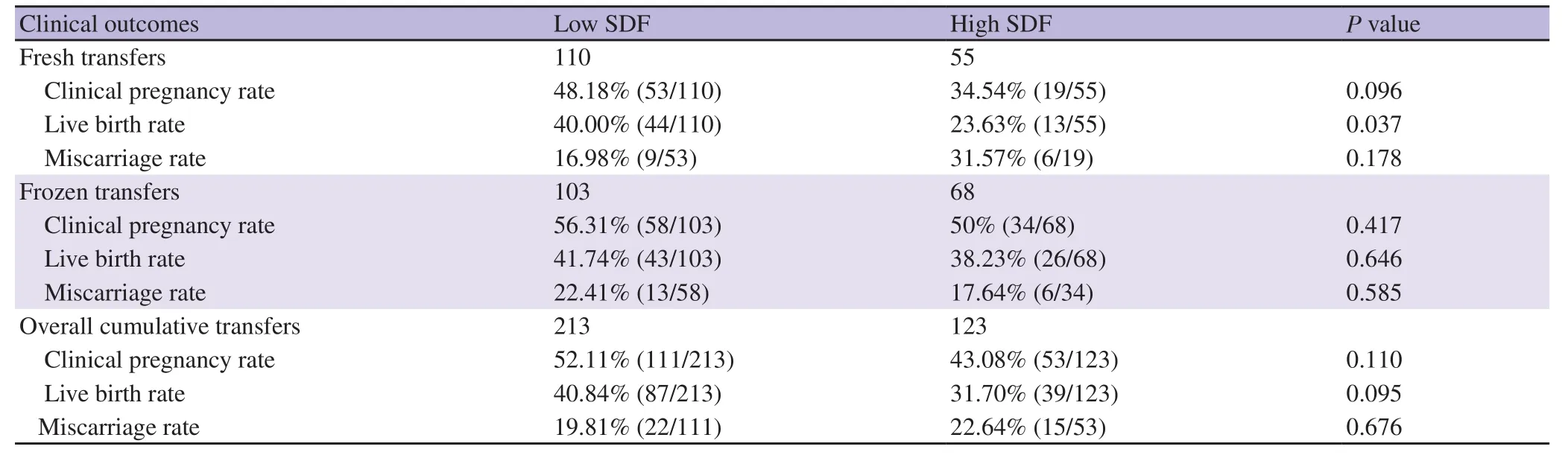
Table 4. Clinical outcomes between the low and high SDF groups in the ICSI cycles of normozoospermic male patients.

Table 5. Clinical outcomes (calculated per patient) between the low and high SDF groups.
3.5. Multivariate logistic regression analysis to predict the effect of SDF on the clinical outcomes in ICSI cycles of normozoospermic male patients
In the multivariate analysis using logistic regression, SDF was a significant predictor of live birth rate and clinical pregnancy rate in the fresh embryo transfer cycles, however, not an independent predictor of clinical outcomes in the overall cumulative transfer cycles and frozen transfer cycles when adjusted for possible confounding factors (Table 6).
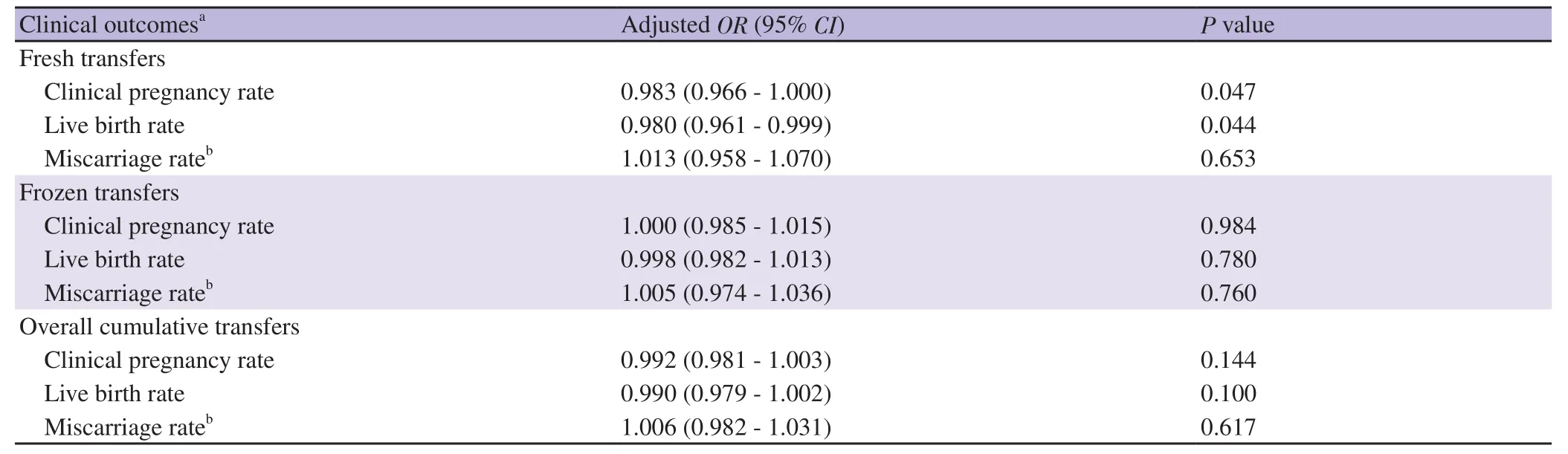
Table 6. Multivariate logistic regression analysis to predict the effect of SDF on the clinical outcomes in ICSI cycles of normozoospermic male patients.
4. Discussion
Routine semen analysis has a salient role in the infertility evaluation of men. But, when it comes to sperm abnormalities at the DNA level it has a meager role. SDF is unfettered by normal semen analysis and has good diagnostic and prognostic capabilities for non-fertile men labeled as idiopathic men based on routine semen parameters[15-17].
In this study, the clinical and laboratory outcomes were correlated between the low and high SDF groups of ICSI cycles of normozoospermic male patients. The clinical outcomes like live birth rate were significantly decreased in the high SDF group of fresh embryo transfer cycles. However, the difference in the clinical outcomes was not observed in the frozen embryo transfer cycles and overall embryo transfer cycles. Various studies in the literature showed the negative effect of SDF on the clinical outcomes in the fresh embryo transfer cycles only[3,18,19]. A particular study showed the negative effect of SDF on the clinical outcomes in non-male factor infertility patients but those findings were also confined to fresh embryo transfers only[3]. Frozen embryo transfers were most preferred in recent times where clinics are opting for the freeze-all policies as they have comparable results with the fresh embryo transfers[20]. Cumulative transfers provide accurate success of the assisted reproductive techniques cycles as they include both fresh and frozen embryo transfers. The effect of SDF on the clinical outcomes should be correlated in cumulative transfers/overall transfers[21].
Some other studies showed that SDF has no effect on clinical outcomes[22-24]. The contentious effect of SDF on the clinical outcomes is possibly due to the female factor. Female factor plays a major role in determining the effect of SDF on the clinical and laboratory outcomes, especially female age. As age decides the quality of oocytes, it has been observed that young females with good quality oocytes can reduce the negative effect of SDF on clinical outcomes[25,26]. In this study, even though female patients included were between the ages of 21-42 years, the average age of females was 30 years; this may possibly be the reason for the no effect of SDF on the clinical outcomes in the overall transfers.Larger studies are needed to know the effect of SDF on clinical outcomes in cumulative transfers. Some other studies noted no significant difference in the clinical outcomes in the frozen embryo transfer cycles of the SDF groups, which is in corroboration with this study[27].
SDF was negatively correlated with sperm motility which is already mentioned in the literature[28]. Other parameters like sperm volume,count, and morphology were similar between the SDF groups.Female BMI was significantly higher in the high SDF group but that does not impact the clinical outcomes in this study. Many studies showed the effect of SDF on the miscarriage rate, but we did not find any difference in the miscarriage rates in any type of transfers either fresh or frozen and overall cumulative transfers maybe due to the younger female patient group[29]. A recent study concludes that SDF in the sample used for fertilization was not associated with embryological and clinical outcomes which are in corroboration with this study[28].
The strengths of the present study are its prospective nature,the clinical and embryological outcomes were evaluated on the actual sperm used in the ICSI, unlike other studies where the SDF assessment was done on the semen samples prior to the ICSI cycles and correlation to the clinical outcome were done at a later time.All the samples were fixed on the same day of ICSI and assessed for SDF on the consecutive day, which is also an important step as in many studies they used to freeze the semen sample and assess SDF later. Freezing and thawing procedures may also impart a certain amount of DNA fragmentation in the semen samples[30].Acridine orange test is a simple method that can be performed inhouse without any extra financial burden to the couples. We have minimized the confounding effect of type of transfer (fresh or frozen) by calculating the clinical outcomes separately for fresh,frozen, and overall cumulative transfers. Other possible confounding factors were also adjusted for the clinical outcomes in multivariate analysis.
The limitations of this study are a smaller sample size due to the inclusion of only ICSI cycles with normozoospermic samples and patients who underwent only day 5 blastocyst transfers. The acridine orange test method may not be robust like the sperm chromatin structure assay (SCSA) method but as mentioned earlier acridine orange test is a simple method and SDF can be evaluated technically similar to the SCSA method.
In conclusion, SDF does not affect the clinical outcomes in the cumulative transfers of an ICSI cycle along with blastocyst transfers in couples with normozoospermic males.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The study received no extramural funding.
Authors’ contributions
Deepthi Repalle conceptualized and planned the design of the study, acquired the data, and drafted the manuscript. Saritha K.V.and Shilpa Bhandari assisted in writing the manuscript and refined the manuscript critically. All authors read and approved the final manuscript.
猜你喜欢
农业工程学报(2022年13期)2022-10-09
科技与创新(2022年4期)2022-03-09
物联网技术(2021年6期)2021-07-01
建材发展导向(2021年23期)2021-03-08
人民长江(2019年7期)2019-09-10
现代农业科技(2009年19期)2009-03-20
中学生数理化·八年级数学华师大版(2008年3期)2008-08-26
中国新闻周刊(2004年11期)2004-04-07
祝您健康(1986年3期)1986-12-31
 Asian Pacific Journal of Reproduction2022年3期
Asian Pacific Journal of Reproduction2022年3期
- Asian Pacific Journal of Reproduction的其它文章
- Oxidative stress and female reproductive disorder: A review
- Investigation of FOXP3 (rs3761548) polymorphism with the risk of preeclampsia and recurrent spontaneous abortion: A systemic review and meta-analysis
- Placental pathologies and fetal outcome in pregnant women with COVID-19: A retrospective study
- Antioxidant potential of pentoxifylline on spermatozoa of small ruminants
- Effect of cholesterol-loaded cyclodextrin enriched extenders on the quality of prefrozen and frozen buffalo semen