
Edible mushrooms as a potent therapeutics of subclinical thyroid dysfunction among adults, especially in obese individuals: a prospective cohort study
2023-01-22 09:45JunjunZhngSbinRymjhiAmrishThpGeMengQingZhngLiLiuHongmeiWuYeqingGuShunmingZhngTingjingZhngXuenWngZhixiCoJunDongXioxiZhengXuZhngXinrongDongXingWngShomeiSunMingZhouQiyuJiKunSongKijunNiu
食品科学与人类健康(英文) 2023年1期
Junjun Zhng, Sbin Rymjhi, Amrish Thp, Ge Meng,b, Qing Zhng, Li Liu,Hongmei Wu, Yeqing Gu, Shunming Zhng, Tingjing Zhng, Xuen Wng,Zhixi Co, Jun Dong, Xioxi Zheng, Xu Zhng, Xinrong Dong,Xing Wng, Shomei Sun, Ming Zhou, Qiyu Ji, Kun Song, Kijun Niu,,,e,f,*
a Nutritional Epidemiology Institute and School of Public Health, Tianjin Medical University, Tianjin 300070, China
b Department of Toxicology and Sanitary Chemistry, School of Public Health, Tianjin Medical University, Tianjin 300070, China
c Health Management Centre, Tianjin Medical University General Hospital, Tianjin 300070, China
d Nutrition and Radiation Epidemiology Research Center, Institute of Radiation Medicine, Chinese Academy of Medical Sciences & Peking Union Medical College, Tianjin 300192, China
e Tianjin Key Laboratory of Environment, Nutrition and Public Health, Tianjin 300070, China
f Center for International Collaborative Research on Environment, Nutrition and Public Health, Tianjin 300070, China
Keywords:Edible mushrooms Subclinical thyroid dysfunction Obese individuals Cohort study
A B S T R A C T
1. Introduction
Subclinical thyroid dysfunction (SCTD) is characterized by abnormal serum thyroid-stimulating hormone (TSH) levels and normal free thyroxine (FT4) and free triiodothyronine (FT3) levels [1].Although only a small proportion of patients with SCTD have symptoms, the prevalence of SCTD is higher than overt thyroid disease [2], and the risk of progression of SCTD to overt thyroid disease is approximately 2% to 6% per year [3]. SCTD can have repercussions on the cardiovascular system and bone, as well as on other organs and systems [4]. Thus, prevention and treatment of SCTD has become an important public health concern. Moreover,though a number of synthetic drugs are available for managing this condition, their long-term use is associated with many side effects. Study showed levothyroxine therapy may be associated with iatrogenic thyrotoxicosis, especially in elderly patients, and there is no evidence that it is beneficial in persons aged 65 years or older [5].Therefore, this has shifted the research in SCTD towards medicinal plants and herbs which are considered to be comparatively safe.
Edible mushrooms have been widely used as health foods, because of their various bioactive constituents such as polysaccharides,proteins, vitamins, minerals, and dietary fiber [6]. Mushrooms have the potential to be the only non-animal, unfortified food source of vitamin D that can provide a substantial amount of vitamin D2in a single serve [7]. There are two forms of vitamin D, vitamin D3(or cholecalciferol) and vitamin D2(or ergocalciferol). Both forms of vitamin D are transported to the liver where they are converted to 25-hydroxyvitamin D, which is the major circulating and stored form of vitamin D [8,9]. Several clinical studies [10,11] have reported low vitamin D levels [(25(OH)D level] in people with autoimmune thyroid diseases, indicating an association between vitamin D deficiency and thyroid autoimmunity. Moreover, mushrooms flavonols can inhibit the activities of enzymes antithyroperoxidase and liver deiodinase as the key enzyme in the biosynthesis of thyroid hormones , bringing about changes in thyroid functions [12]. Thus, we speculated that due to its abundant nutrients edible mushrooms might have a beneficial effect on the prevention of SCTD.
However, to date, the potential effects of habitual edible mushrooms consumption on SCTD have not been evaluated in population-based studies. Therefore, we conducted a large prospective cohort study to investigate whether edible mushrooms consumption were associated with SCTD in general adult population.
2. Materials and methods
2.1 Participants
This prospective cohort study used data from the Tianjin Chronic Low-grade Systemic Inflammation and Health (TCLSIH or TCLSI Health) Cohort Study,it is a multipurpose dynamic prospective cohort study that began in 2007, ranging from 2013 to 2019. The study recruited men and women aged 18 years and older from the general population living in Tianjin, a city which is located in the North China, east of Bohai Sea, where iodine intake is sufficient [13,14]. It is well known that iodine is closely associated with the occurrence of thyroid disease with abnormal synthesis of thyroid hormone [15],thus, our study is carried out in a general adult population living in Tianjin , China can well prevent iodine in the environment from affecting the association between edible mushrooms consumption and the risk of SCTD. The rationale and details of the study design have been reported in previous studies [16]. Briefly, participants who had received health examinations including abdominal ultrasound and blood draw and had completed questionnaires regarding their smoking and alcohol-consumption habits and disease history since January 2010. They completed a detailed lifestyle questionnaire survey(which included questions about their household income, occupation,educational level, physical activity, and dietary intake, etc.) since May 2013. This study conforms to the strengthening the reporting of observational studies in epidemiology (STROBE) guidelines for cohort studies, and written informed consent of participants.
For the current study, we analyzed the TCLSIH study database from May 2013 to December 2019. This analysis includes a total of 10 341 participants. Of these individuals, we excluded those with insufficient data (n= 56) and those with a history of thyroid disease(n= 208), overt hyperthyroidism (serum TSH < 0.55 mIU/L with elevated FT4) (n= 37), overt hypothyroidism (serum TSH > 4.78 mIU/L with low FT4) (n= 41), cardiovascular disease (CVD) (n= 522),cancer (n= 77) at baseline. We also excluded participants who were first enrolled into the cohort in 2019 (n= 2 769). For assessment the association between edible mushrooms consumption and the incidence of subclinical hypothyroidism, we excluded those with subclinical hypothyroidism at baseline (n= 480) and lost to follow-up (n= 1 041),the final follow-up analysis for subclinical hypothyroidism covered 5 110 participants (follow-up rate: 83.1%). For assessment the association between edible mushrooms consumption and the incidence of subclinical hyperthyroidism, we excluded those with subclinical hyperthyroidism at baseline (n= 148) and lost to follow-up(n= 881), the final follow-up analysis for subclinical hyperthyroidism covered 5 602 participants (follow-up rate: 86.4%). The participant selection process was described in Fig. 1.
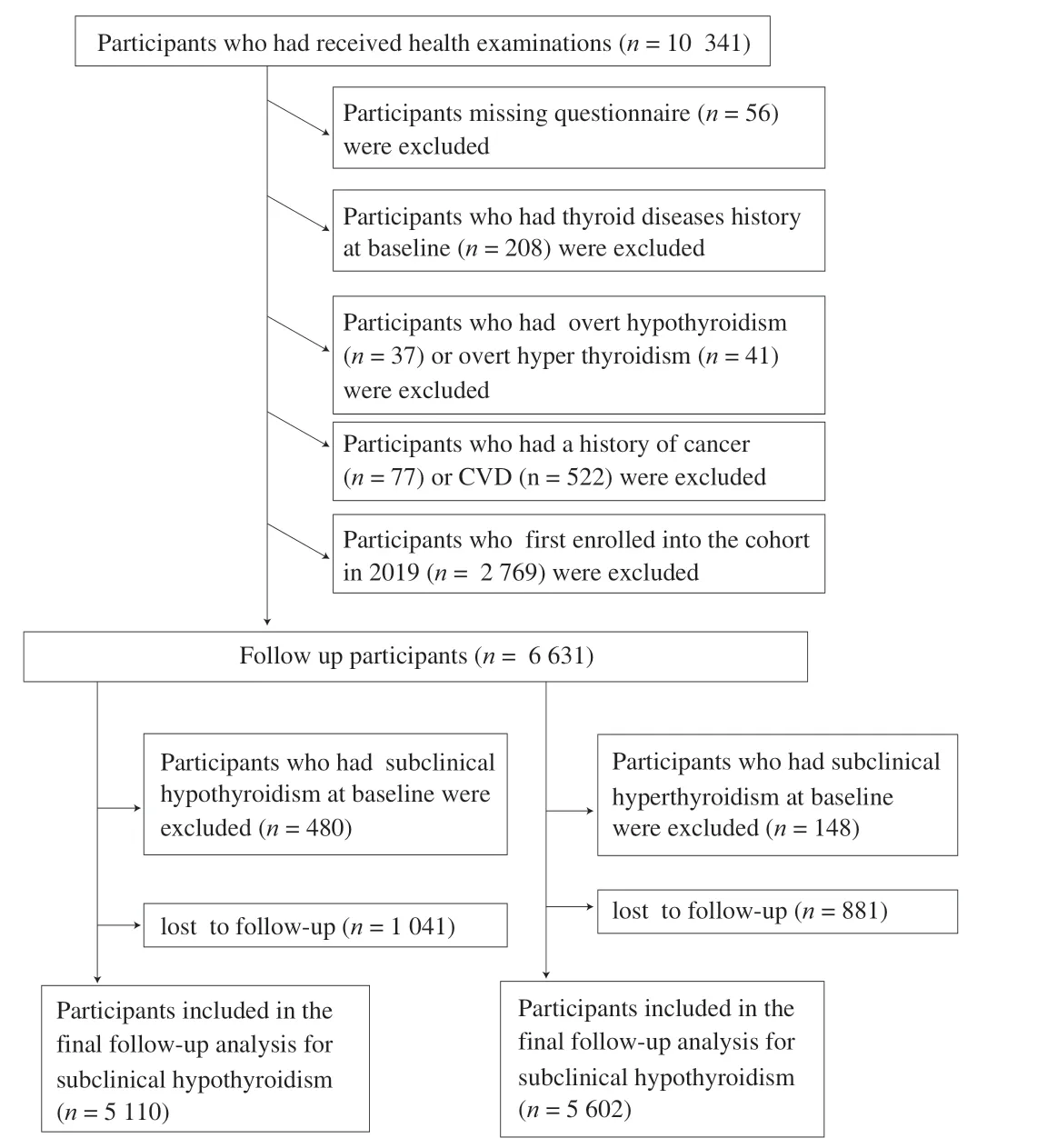
Fig. 1 Flow diagram showing the selection of the study population.
2.2 Diagnosis of SCTD
Chemiluminescence immunoassay was used to measure serum FT3, FT4, and TSH levels, using the ADVIA Centaur FT3, FT4,and TSH3-Ultra analyzer (Siemens Healthcare Diagnostics, New York, NY). The ranges of measurement for FT3, FT4, and TSH were 0.3-30.8 pmol/L, 1.3-155 pmol/L, and 0.001-150 mIU/L, respectively.Based on the previous reports and national guidelines [17,18],euthyroidism was defined with TSH values of between 0.55-4.78 mIU/L and FT4 between 11.5-22.7 pmol/L. Subclinical hypothyroidism was diagnosed with TSH > 4.78 IU/mL and normal FT4 levels;Subclinical hyperthyroidism was diagnosed with TSH < 0.55 IU/mL and normal FT4 levels. Overt hypothyroidism was considered when there were high TSH and low FT4 values (< 11.50 pmol/L) and overt hyperthyroidism was diagnosed with TSH < 0.55 mIU/L with elevated FT4 values (> 22.7 pmol/L).
2.3 Assessment of dietary intake
Dietary intake over the previous month was assessed using an 81-item food frequency questionnaire (FFQ) since May 2013 [19].Participants were asked how often on average over the past month they had consumed specific foods with standard serving sizes. The FFQ inquired about the mean consumption frequency of selected food items during the previous month using 7 frequency categories ranging from‘almost never eat’ to ‘twice or more per day’ for foods and 8 frequency categories ranging from ‘almost never drink’ to ‘four or more times per day’ for beverages (see Supplemental Table 1). Then, a common unit or portion size derived from the validation study of the FFQ was specified for each food and beverage item [20]. Nutrients and total energy intake were calculated using the data from the FFQ combined with the 2009 version of Chinese Food Composition Tables [21], which is relevant to the data collected from 2013 to 2019. In a random subsample of 150 participants from the TCLSIH study, the reproducibility and validity of the FFQ were examined by comparing the data from two FFQs administered approximately three months apart and four 4-day weighed diet records (WDRs). The Spearman’s rank correlation coefficients comparing the FFQ to WDRs were 0.49 for total energy,0.35-0.54 for nutrients (n-3 fatty acid, fat and carbohydrate), and 0.69 for mushrooms. The Spearman correlation coefficients between two FFQs were 0.68 for total energy, 0.62-0.79 for food items (fruits,vegetables, sweet foods, and beverages), and 0.75 for mushrooms.Energy and nutrient intakes were calculated by using an ad hoc computer program developed to analyze the FFQ.
Mushrooms consumption was assessed through one specific question. The question considered the consumption of edible mushrooms, includingLentinulaedodes,Auriculariaauriculajudae,Pleurotusostreatus,Flammulinavelutipes,Agaricus bisporus. Participants indicated the consumption frequency of edible mushrooms over the previous 1 month in terms of the specified serving size by selecting one of the 7 frequency categories: almost never, < 1 time/week, 1 time/week, 2-3 times/week, 4-6 times/week,1 time/day, and ≥ 2 times/day. In our study, a standard portion size(represented the 50th percentile of the weighed diet records) of edible mushroom was 50 g and 30 g for men and women, respectively.Because most of the variation in intake of any food is explained by the frequency of its use [20], edible mushrooms consumption frequency(rather than amount) was used as the main exposure variable in this study. We summarized the categories of edible mushrooms into three groups: almost never, 1–3 times/week and ≥ 4 times/week.
2.4 Assessment of covariates
Levels of fasting blood glucose (FBG) were measured by glucose oxidase method. As for lipids, triglycerides (TG) and total cholesterol(TC) were measured by enzymatic methods. Low-density lipoprotein(LDL) was measured by the polyvinyl sulfuric acid precipitation method, and high-density lipoprotein (HDL) was measured by the chemical precipitation method using appropriate kits on a Cobas 8000 analyzer (Roche, Mannheim, Germany). Blood pressure (BP)was measured twice from the upper right arm using an automatic device (Andon, Tianjin, China) after 5 min of rest in a seated position.Metabolic syndrome (MetS) was defined according to the 2009 American Heart Association scientific criteria [22].
Data on demographics (age, sex, education level, occupation,monthly household income), smoking status, alcohol drinking status, and personal and family history of diseases were collected using self-administered questionnaires. The anthropometric variables including height, body weight, and waist circumference(WC) were recorded by using a standard protocol. Height and body weight were measured by trained staff following a standard protocol. Body mass index (BMI) was calculated as the body weight (kg) divided by the height squared (m2). WC was assessed at the level of the umbilicus with participants standing and breathing normally. Physical activity (PA) was evaluated using the short form of the validated seven-day International Physical Activity Questionnaire (IPAQ) [23]. Total physical activity was expressed as metabolic equivalent hours per week (MET-h/week).
2.5 Statistical analysis
All statistical analyses were performed in 2019 using SAS, version 9.4 for Windows (SAS, Inc.). Distributions of continuous variables were assessed for normality using the Kolmogorove Smirnov(n> 2 000) or Shapiroe Wilk (n< 2 000) test. Baseline characteristics of the study participants were presented as the mean (95% confidence interval, CI) for continuous variables and percentages for categorical variables. Follow-up time was calculated from the date of completing the baseline FFQ survey to the date of the first diagnosis of SCTD, the end of follow-up (31 December 2019), or loss to follow-up, whichever was earliest. Cox proportional hazards regression models were used to assess the association between edible mushroom consumption and risk of subclinical hypothyroidism and subclinical hyperthyroidism.The incidence of subclinical hyperthyroidism and subclinical hypothyroidism was used as dependent variable, and edible mushrooms consumption was used as independent variables. The proportional hazard assumption was tested using Schoenfeld residuals and no violation was found. Five models were developed. The hazard ratios (HRs) and corresponding 95% CI were calculated using almost never group as the reference. Model 1 was crude model. In model 2,we adjusted for age (continuous: years), sex (men or women), and BMI (continuous: kg/m2). In model 3, we further adjusted for smoking status (current, former, or never), alcohol drinking status (everyday drinker, sometime drinker, ex-drinker, or non-drinker), education level (college graduate or not), occupation (managers, professionals,or other), monthly household income (≤ or > 10 000 Yuan), physical activity (continuous: MET-hour/week), family history of disease(including CVD, hypertension, hyperlipidemia, and diabetes [each yes or no]). In model 4, we additionally adjusted for dietary patterns.Dietary patterns were derived by using factor analysis with principal component based on the original 100 foods/food groups listed in the FFQ and to determine factor loadings for each food item (gram).Varimax rotation was applied to enhance interpretability. Three factors (sweet pattern, healthy pattern, and animal food pattern) were identified through combining criteria of the eigenvalues (greater than 1.0), scree plot test, and interpretability [24]. Study showed total iodine intake in food accounted for 42.7% of the population’s iodine intake in Tianjin [14], therefore, in a final model, we further adjusted total iodine intake in food. Linear trend tests across quartile categories of mushrooms consumption were calculated by using the categories of mushrooms consumption (almost never: 1; 1–3 times/week:2 and ≥ 4 times/week: 3) as an ordinal variable. Stratified analyses were performed to explore whether the association between edible mushrooms consumption and prevalence of subclinical hypothyroidism differ by sex and obesity status [BMI (kg/m2) of < 24 or ≥ 24].
We evaluated the interactions between edible mushrooms consumption and all covariates for through the addition of the crossproduct terms in fully adjusted model. The likelihood ratio test was used to assess the significance of interaction terms.
To examine the robustness of our results, we conducted the sensitivity analyses: 1) repeated our analysis after excluding participants who consumed nutritional supplements/health products at baseline; 2) repeated the fully adjusted model by adjusting for waist circumference instead of BMI. All statistical tests were two-sided,and statistical power 1 -β= 0.8,αP< 0.05 was considered to be statistically significant.
3. Results
3.1 Baseline characteristics of participants
The baseline characteristics of the study population are shown in Table 1. Between May 2013 and December 2019, a total of 5 110participants included in the final follow-up analysis for subclinical hypothyroidism, 138 subclinical hypothyroidism new cases were identified (median follow-up of 3.0 years),the incidence rate of subclinical hypothyroidism was 8.9/1 000 person-years. During follow-up period, the incidence rate of subclinical hyperthyroidism was 7.2/1 000 person-years, 5 602 participants included in the final follow-up analysis for subclinical hyperthyroidism, 124 subclinical hyperthyroidism cases were identified (median follow-up of 3.1 years). The geometric mean age (95% CI) was 45.0 (44.7, 45.3), and the proportion of men was 55.1%.
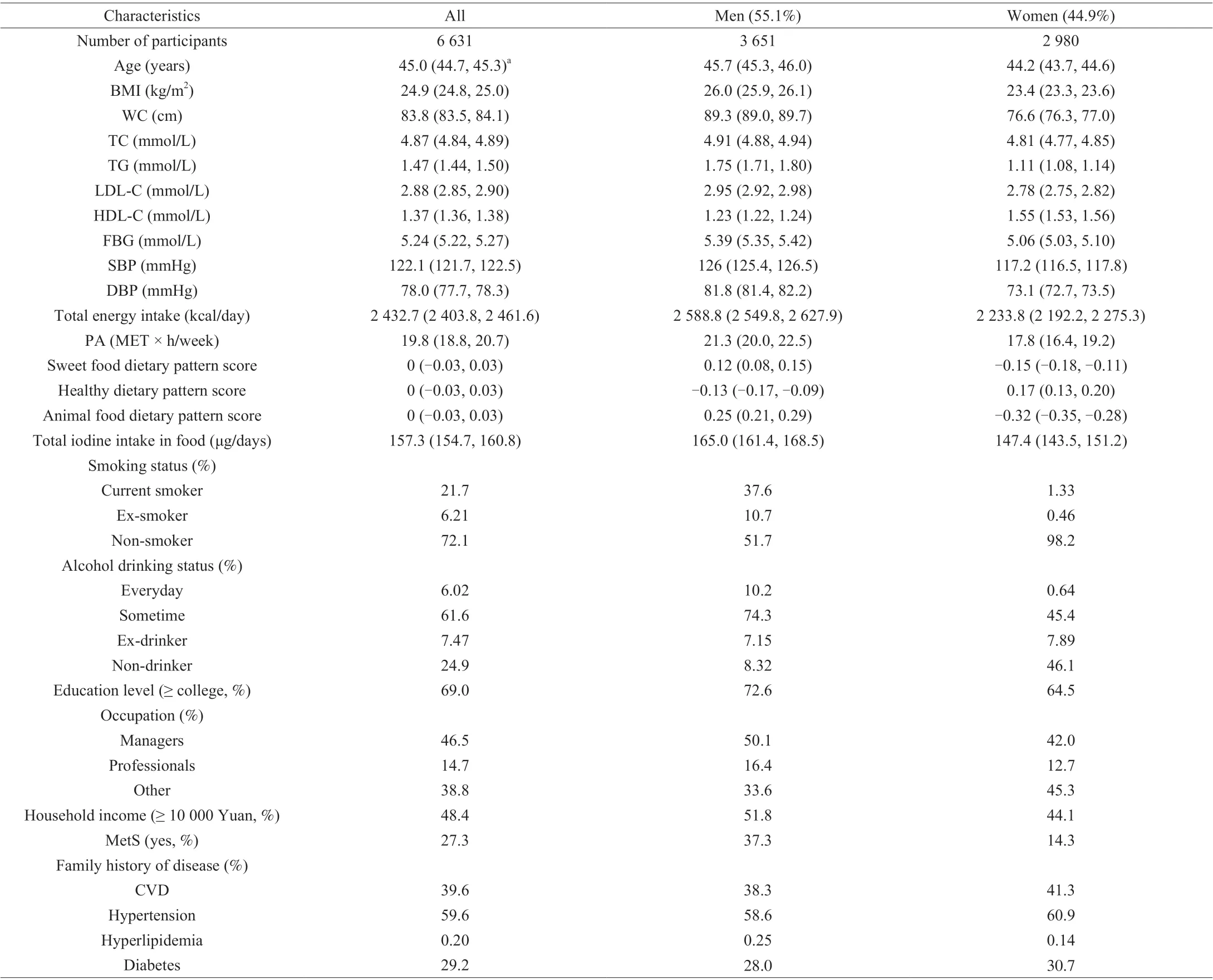
Table 1 Baseline characteristics of participants (n = 6 631)a.
3.2 Association between edible mushrooms consumption and risk of SCTD
Table 2 presents the crude and adjusted associations between categories of edible mushrooms consumption and subclinical hypothyroidism. In the age-, sex-, and BMI-adjusted model, HRs and 95% CIs for subclinical hypothyroidism across edible mushrooms consumption categories (almost never, 1–3 times/week and ≥ 4 times/week)were 1.00 (reference), 0.53 (0.30, 0.95) and 0.31 (0.12, 0.83),respectively (Pfor trend = 0.01). Further adjustment for lifestyle and family history of disease (model 3) did not appreciably alter the negative association between edible mushrooms consumption and risk of subclinical hypothyroidism. After adjusting for dietary factors,these associations were not altered. In model 5 additionally adjusted for total iodine intake in foods, the multivariable HRs (95% CIs) were 1.00 (reference), 0.53 (0.29, 0.97) for 1–3 times/week and 0.30 (0.10,0.87) for ≥ 4 times/week (Pfor trend = 0.02).
Table 3 presents the crude and adjusted associations between categories of edible mushrooms consumption and subclinical hyperthyroidism. Model 1, the HRs and 95% CIs for subclinical hyperthyroidism across edible mushrooms consumption categories(almost never, 1–3 times/week and ≥ 4 times/week) were 1.00(reference), 0.54 (0.28, 0.99) and 0.56 (0.23, 1.36), respectively (Pfor trend = 0.21). After adjusting for factors, the multivariable HRs (95%CIs) were 1.00 (reference), 0.53 (0.28, 1.00) and 0.72 (0.27, 1.96)(Pfor trend = 0.38).
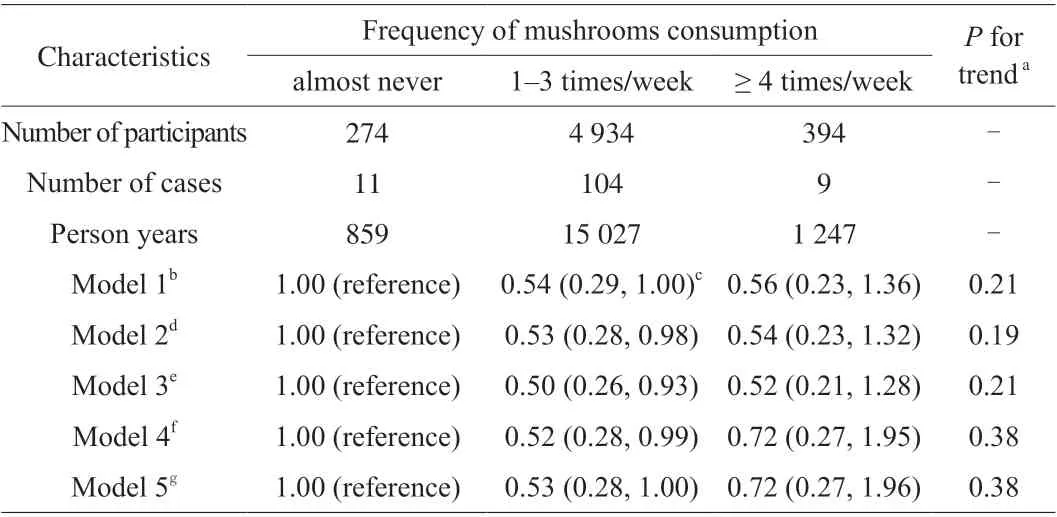
Table 3 Associations between frequency of mushrooms consumption and risk of subclinical hyperthyroidism (n = 5 602).
Stratified analyses indicated that edible mushrooms consumption was associated with subclinical hypothyroidism in men or obese individuals (BMI ≥ 24 kg/m2) but not in women or non-obese individuals (BMI < 24 kg/m2) (Fig. 2).
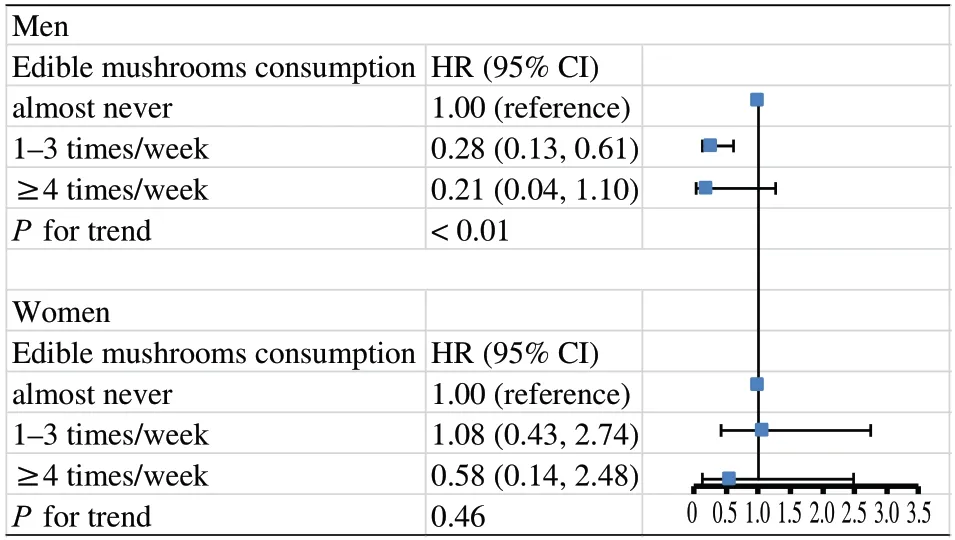
Men Edible mushrooms consumption HR (95% CI)almost never 1.00 (reference)1–3 times/week 0.28 (0.13, 0.61)≥4 times/week 0.21 (0.04, 1.10)P for trend < 0.01 Women Edible mushrooms consumption HR (95% CI)almost never 1.00 (reference)1–3 times/week 1.08 (0.43, 2.74)≥4 times/week 0.58 (0.14, 2.48)P for trend 0.460 0.5 1.0 1.5 2.0 2.5 3.0 3.5
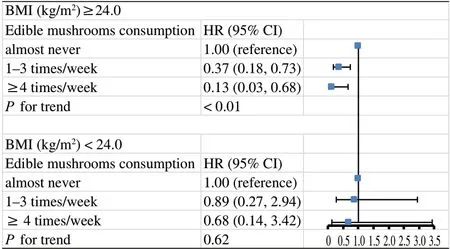
Fig. 2 Association of edible mushrooms consumption with subclinical hypothyroidism stratified by sex and BMI. Multivariable model was adjusted for age, sex, BMI, smoking status, alcohol drinking status, education level,occupation, household income, physical activity, family history of disease(including cardiovascular disease, hypertension, hyperlipidemia, and diabetes),hypertension, hyperlipidemia, diabetes, three main dietary pattern scores, total iodine intake in food.
We found no interaction between edible mushrooms consumption and variables on subclinical hypothyroidism: age (< 40 or ≥40 years) (Pfor interaction = 0.09), sex (men or women) (Pfor interaction = 0.14), BMI (< 24.0 or ≥ 24.0 kg/m2) (Pfor interaction =0.30), smoking status (current, former, or never) (Pfor interaction =0.82), alcohol drinking status (everyday drinker, sometime drinker,ex-drinker, or non-drinker) (Pfor interaction = 0.40), occupation(managers, professionals, or other) (Pfor interaction = 0.40), household income (≤ or > 10 000 Yuan) (Pfor interaction = 0.09), physical activity(< or ≥ 23 MET-hour/week) (Pfor interaction = 0.59), family history of hypertension (yes or no) (Pfor interaction = 0.27), family history of hyperlipidemia (yes or no) (Pfor interaction = 0.96), family history of diabetes (yes or no) (Pfor interaction = 0.86), except for education level(< or ≥ college graduate) (Pfor interaction = 0.01).
In sensitivity analysis, the results were unchanged after excluding participants who consumed nutritional supplements/health products at baseline (n= 407), the fully model adjusted HRs 95% CIs for subclinical hypothyroidism across edible mushrooms consumption categories were 1.00 (reference), 0.51 (0.27, 0.94) and 0.26 (0.08,0.80) (Pfor trend < 0.01). Furthermore, the results were not substantially changed when we adjusted for waist circumference instead of BMI. The fully model adjusted HRs 95% CIs for subclinical hypothyroidism across edible mushrooms consumption categories were 1.00 (reference), 0.51 (0.28, 0.91) and 0.28 (0.10,0.81) (Pfor trend = 0.01).
4. Discussion
In this large-scale prospective study of a Chinese adult population,we have examined the relationship between edible mushrooms consumption and the incidence of SCTD in general population. The results suggested that edible mushrooms are negatively related to the incidence of subclinical hypothyroidism, but no significant related to the incidence of subclinical hyperthyroidism.
In our study, the subclinical hypothyroidism incidence rate was 8.9 cases per 1 000 person-years, which is higher than the incidence rate in Taiwan [25], where during an average follow-up of 4.2 years, the subclinical hypothyroidism incidence rate in that study was 4.3 cases per 1 000 person-years. The subclinical hyperthyroidism incidence rate was 7.2 cases per 1 000 person-years, which is also higher than the incidence of 2.9 per 10 000 person-years in Britain [26] where the median follow-up period was 4.3 years. However, results vary depending on different survey times, different diagnostic criteria, and different sample populations.
We adjusted for multiple potentially confounding factors in our analysis. First, since studies have shown that thyroid function is related to age, sex and BMI [27,28], we adjusted for these three variables. Secondly, studies [29,30] have shown that sociodemographic factors, lifestyle factors, nutritional status, and chronic diseases could also influence the prevalence of subclinical hypothyroidism, we made further adjustments for smoking status,drinking status, educational level, working status, household income,PA and family history of disease. However, adjustments for these confounding factors did not change the observed associations. In addition, we have adjusted three dietary pattern scores, the negative association between edible mushrooms consumption and subclinical hypothyroidism did not substantially change after adjustment for these factors. Finally, we have adjusted for total iodine intake in foods,the final result has not been changed. However, after adjusting for factors, there is no significant association between edible mushrooms consumption and subclinical hyperthyroidism.
Although the exact mechanisms of edible mushrooms consumption in subclinical hypothyroidism have not been elucidated,biologically active ingredients in mushrooms might be the candidates for this negative relationship. Firstly, Mushrooms have high concentrations of ergosterol (vitamin D2) in their cell walls(approximately 61.5 mg/100 g dry weight), which is a good source of vitamin D [31]. The two main dietary forms of vitamin D are D2, found in fungi and yeast, and D3, found in animals [32], and both are used as vitamin D supplements. Recent literature has illustrated the presumed association between serum vitamin D and thyroid diseases [33].Vitamin D deficiency can increase the incidence of subclinical hypothyroidism because the polymorphisms of vitamin D receptors(VDR) are related to the predisposition of people to subclinical hypothyroidism [34], and vitamin D is an important immune system regulator that can inhibit the development of autoimmune diseases [11]. Moreover, flavonols in mushrooms was demonstrated can inhibit the activities of enzymes antithyroperoxidase and liver deiodinase as the key enzyme in the biosynthesis of thyroid hormones and bring about some changes in thyroid functions [12]. Animal studies [35,36] suggested that flavonols may lower the level of thyroid hormone, which would enhance the secretion of TSH and lead to the development of subclinical hypothyroidism. Finally, subclinical hypothyroidism is most often caused by autoimmune thyroiditis.Cellular autoimmunity with the TH1 profile of CD4+T helper precursor cells is predominant in subclinical hypothyroidism [37].The active substances in edible mushrooms can improve the immune system by activating immune effector cells including macrophages,natural killer cells, and T cells [38,39], and thus can reduce the incidence of subclinical hypothyroidism caused by immunodeficiency. Further studies are required to clarify the exact mechanisms of this effect.
Since sex-specific differences were observed in subclinical hypothyroidism, we analyzed the relationship between edible mushrooms and subclinical hypothyroidism by sex in this study. Our results found that there is a greater negative relationship between edible mushroom consumption and subclinical hypothyroidism in males than in females (Fig. 2). This result may be explained by the regulatory effect of androgen on the thyroid. A previous study [40]shows that high levels of androgen can lead to an increase in TSH level and subclinical hypothyroidism, while active ingredients in mushrooms can reduce androgen synthesis, thus the effect of edible mushroom consumption on subclinical hypothyroidism was is greater in men.
We observed that edible mushrooms consumption was inversely associated with subclinical hypothyroidism in obese individuals but not non-obese individuals (Fig. 2), Although we adjusted BMI in the Cox proportional hazards regression models, it did not appreciably alter the negative association between edible mushrooms consumption and subclinical hypothyroidism. We also did the interaction between BMI and edible mushrooms consumption on subclinical hypothyroidism(Pfor interaction = 0.30). It is well known that serum cholesterol levels were significantly higher among obese individuals [41],and a study demonstrated that TSH was positively associated with serum cholesterol [42]. Thus, obese individuals will show higher level of TSH. Edible mushrooms have been proved to have antioxidant capacities, which increase the antioxidant defense systems in cells.They can boost anti-inflammatory actions and thereby protect against obesity-related dyslipidemia [43]. Therefore, the effect of edible mushrooms on subclinical hypothyroidism among obese individuals may more significant than that in non-obese individuals.
There are few prospective cohort studies with SCTD as the outcome,and epidemiological studies linking edible mushrooms consumption and SCTD are scarce. The current study demonstrated that edible mushrooms consumption is inversely associated with subclinical hypothyroidism.Thus, our research not only supplemented the data of SCTD, but also provided the new insight on edible mushrooms intake and chronic disease. To our knowledge, this is the first study to investigate the association of edible mushrooms intake with SCTD in the general Chinese population. Moreover, the strengths of this study include its prospective cohort design, large sample size, high rates of follow-up,detailed measurements of diet and lifestyle factor.
Some limitations merit further discussion. Firstly, data on edible mushroom species and the cooking methods of edible mushrooms were not available in this study. Thus, there are probably unknown effects on SCTD from different kinds of edible mushrooms and different cooking and processing methods of edible mushrooms.However, according to previous studies, many different kinds of edible mushrooms are rich in active substances such as vitamin D [7]and polysaccharides [44], which play an important role in preventing subclinical hypothyroidism. Therefore, the effect of different mushroom species on the prevention of subclinical hypothyroidism may not be significant. Secondly, owing to the nature of selfadministered questionnaire, some level of reporter and recall bias is possible. However, unreliable FFQs were excluded in our study.Thirdly, further stratification cannot conduct due to the low incidence of SCTD, resulting in fewer cases in the cohort. Finally, since the study results only represent the study region, it is possible that our results cannot be generalized to other populations. Further studies are needed to verify the results in other populations. Finally, omics analysis and sequencing should be carried out to identify the key regulatory factors of edible mushrooms in improving thyroid function.
5. Conclusion
In conclusion, this large-scale study provides perspective evidence that edible mushrooms consumption was negatively associated with risk of subclinical hypothyroidism, especially in obese individuals,but not subclinical hyperthyroidism. Future study is needed to replicate our findings and disentangle the underlying mechanisms.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgments
This study was supported by grants from the National Natural Science Foundation of China (81941024), Tianjin Major Public Health Science and Technology Project (21ZXGWSY00090),National Health Commission of China (SPSYYC 2020015), Food Science and Technology Foundation of Chinese Institute of Food Science and Technology (2019-12), 2014 and 2016 Chinese Nutrition Society (CNS) Nutrition Research Foundation -DSM Research Fund(2016-046, 2014-071 and 2016-023), China.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in the online version, at http://doi.org/10.1016/j.fshw.2022.07.019.
- 食品科学与人类健康(英文)的其它文章
- Wine, beer and Chinese Baijiu in relation to cardiovascular health:the impact of moderate drinking
- Comparative analysis of physicochemical properties, ginsenosides content and α-amylase inhibitory effects in white ginseng and red ginsen
- Monitoring and identif ication of spoilage-related microorganisms in braised chicken with modif ied atmosphere packaging during refrigerated storage
- Effect of cooking processes on tilapia aroma and potential umami perception
- Formation mechanisms of ethyl acetate and organic acids in Kluyveromyces marxianus L1-1 in Chinese acid rice soup
- Volatile prof ile and multivariant analysis of Sanhuang chicken breast in combination with Chinese 5-spice blend and garam masala