
Long-term survival of patients with hepatocellular carcinoma with hepatic, pulmonary, peritoneal and rare colon metastasis: A case report
2023-10-21 01:02YongQiangGongTaiLiangLuChaoWuChen
Yong-Qiang Gong, Tai-Liang Lu, Chao-Wu Chen
Abstract
Key Words: Hepatocellular carcinoma; Multiple metastasis; Rare colon metastasis;Comprehensive treatments; Long-term survival; Case report
INTRODUCTION
Hepatocellular carcinoma (HCC) is one of the most common malignant cancers, with a high metastatic and invasive potential and a low survival rate[1]. While patients with HCC often present with intrahepatic lung and bone metastasis,digestive tract metastases are rare[2,3]. There are many therapeutic approaches for treating HCC that can be widely classified by their ability to cure or control the tumor. Liver transplant, hepatic resection, and ablative therapies are performed with curative intent, while the majority of locoregional therapies, systemic chemotherapies and sorafenib are considered palliative. Although numerous treatment strategies for metastatic HCC have been evaluated, there has been no significant reduction in HCC mortality. Here we report a case of a long-term survival from primary HCC with early successive liver, lung, peritoneal, and colon metastases following comprehensive treatments.
CASE PRESENTATION
Chief complaints
A 47-year-old male was transferred to our hospital who had received comprehensive treatment for HCC for 4 years and was complaining of hematochezia for 20 d.
History of present illness
The patient was admitted to a local hospital in February 2015 for upper abdominal pain. Computer tomography (CT)revealed several circular low-density shadows with a maximum size of 4.1 cm × 4.5 cm in the right lobe of the liver(Figure 1). Liver cancer with rupture and hemorrhage was suspected, and no evidence of metachronous metastases were observed. A partial right hepatic lobe resection and cholecystectomy was performed on March 5, 2015. The patient also underwent abdominal and pelvic exploration as well as a priming wash. Operative pathology confirmed a moderately differentiated HCC.
The patient was admitted to our hospital for regular follow up 1 mo later. CT showed a small hepatic nodule in his quadrate lobe, suggesting a possible metastasis. He underwent trans-arterial chemoembolization (TACE) for recurrent HCC in the liver on May 13, 2015. The patient recovered well, and no abnormalities were observed at until 1-year follow up in May 2016, when a CT scan found a metastatic tumor in the lower lobe of his right lung and a 2.5 cm × 2.0 cm mass in his peritoneal soft tissue (Figure 2). Based on the Barcelona Clinic Liver Cancer staging system, the patient was started on palliative sorafenib 0.4 gper ostwice daily on May 17, 2016. The patient’s AFP level gradually increased from 2015 to 2017, peaking at 99 ng/ml. The multiple disciplinary team (MDT) suggested the patient undergo surgical resection of his peritoneal and pulmonary metastases. The peritoneal metastases were resected on January 23rd, 2017, and a partial lobectomy was performed on March 27, 2017. A postoperative biopsy confirmed pathologic change within the metastatic deposits (Figure 3). The patient’s postoperative AFP decreased to 20-30 ng/mL. His coagulation and liver function remained normal throughout treatment.
Seven months later, in November 2017, a CT scan observed a lesion in the patient’s ascending colon and multiple small flaky low-density nodules in his liver. The patient underwent a colonoscopy, and biopsy histology was consistent with metastatic HCC (Figure 4). Immunohistochemical results were Hepatocyte (+), Glypican-3 (+), CD34 (indicating vascularization), CDX2 (-), CK7 (-), and CK20 (-). Magnetic resonance imaging and an abdominal ultrasound suggested recurrent HCC. The patient consequently underwent TACE for multifocal HCC recurrence in his liver. Given concern for the patient’s overall condition, a MDT meeting was held and systemic treatment was recommended. The patient was admitted to an anti-programmed death 1 (PD-1) clinical trial in our hospital. The patient received SHR-1210 200mg, i.v.gtt on day 1+ and apatinib mesylate 250 mg,per oson days 1-14, a series that was repeated every 2 wk from July 10, 2018 to March 6, 2019. During this period, the patient’s AFP levels fluctuated between 25 and 100 ng/mL.

Figure 1 Abdominal computer tomography showing several heterogenous lesions in the right lobe of the liver. A: Arterial phase; B: Venous phase; C: Plain scan.
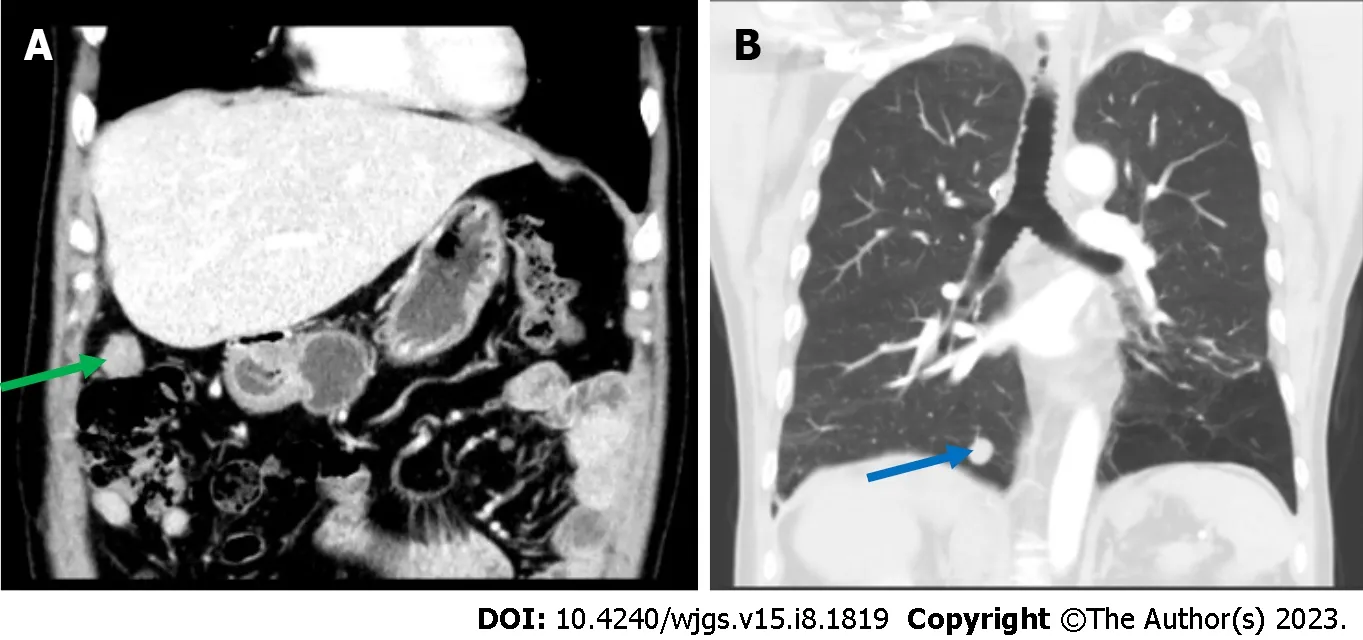
Figure 2 An abdominal computer tomography showed a 2.0 cm × 1.6 cm nodular soft tissue density lesion in the right upper peritoneum(green arrow), and thoracic computer tomography showed a nodular lesion about 1.6 cm in diameter in the basal segment of the right lower lung (blue arrow). A: An abdominal computer tomography; B: Thoracic computer tomography.
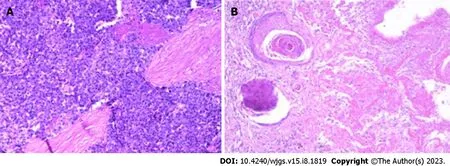
Figure 3 Pathology of the peritoneal mass and pulmonary lesion, which were consistent with metastatic hepatocellular carcinoma. A:Peritoneal mass; B: Pulmonary lesion.
The patient complained of hematochezia for over 20 d. Considering the possibility of colon mass rupture and bleeding,the patient was withdrawn from anti-PD-1 immunotherapy until March 17, 2019.
History of past illness
Hepatitis B diagnosed in 2009.
Personal and family history
The patient denied any special personal or family history.
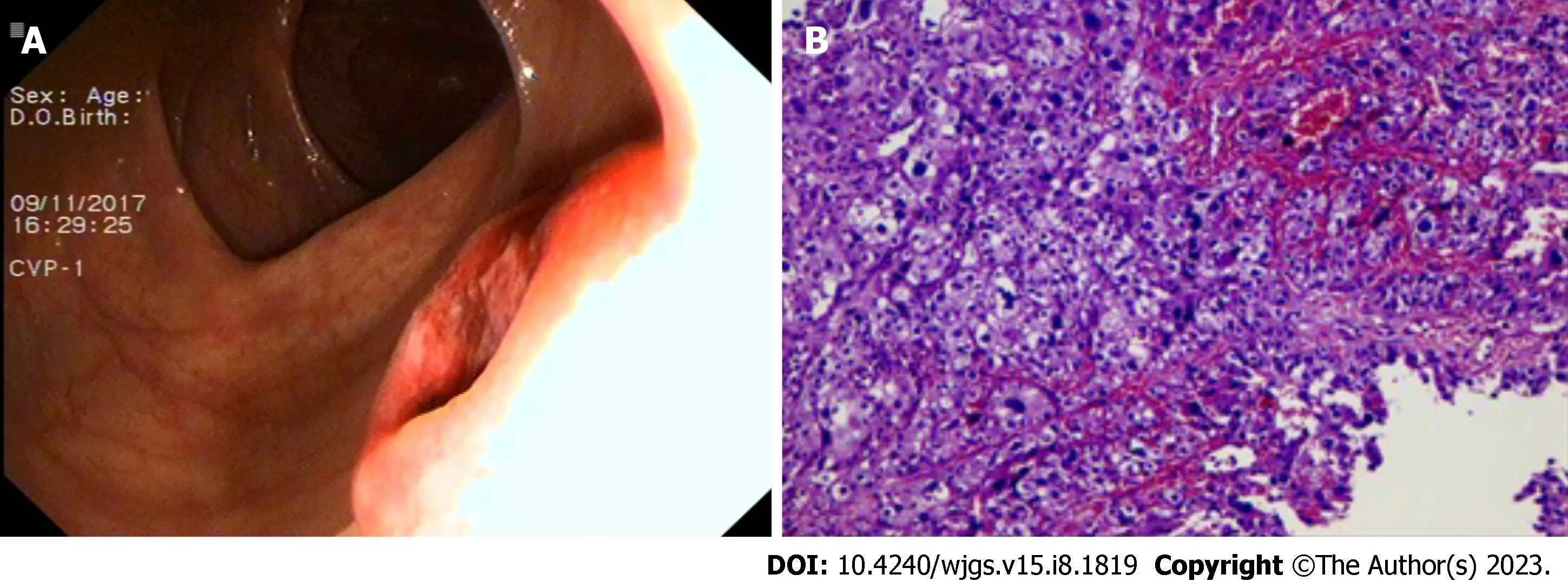
Figure 4 Colonoscopy found a mass in the ascending colon and the biopsy confirmed metastatic hepatocellular carcinoma in the ascending colon. A: Colonoscopy; B: Biopsy.
Physical examination
A flat and soft abdomen with several visible surgical scars on the epigastrium.
Laboratory examinations
Alpha-fetoprotein (AFP) level was 34 ng/mL (reference range 0-20 ng/mL).
Imaging examinations
A 2015 CT scan revealed multiple circular low-density shadows with a maximum size of 4.1 cm × 4.5 cm in the right lobe of the liver (Figure 1). A May 2016 CT scan showed a metastatic tumor in right lower lobe of lung (Figure 2A) and a 2.5 cm × 2.0 cm mass in the peritoneal soft tissue (Figure 2B). Operative pathology of the peritoneal mass (Figure 3A) and pulmonary lesion (Figure 3B) confirmed pathologic change in the metastatic HCC. In November 2017, a CT scan found a lesion in the ascending colon and multiple small flaky low-density nodules in the liver. A colonoscopy was performed to biopsy the mass in the ascending colon (Figure 4A), which confirmed metastatic HCC in the ascending colon (Figure 4B).
FINAL DIAGNOSIS
HCC with hepatic, pulmonary, peritoneal, and colon metastases.
TREATMENT
The patient was withdrawn from anti-PD-1 immunotherapy on March 17, 2019, because of hematochezia, which was thought to be from a ruptured mass in his colon. A CT scan revealed increased size of the mass in the ascending colon wall. The MDT recommended a colectomy, and a radical resection of the right colon was performed on May 26, 2019,with pathology consistent with metastatic HCC. The patient recovered well postoperatively, and no abnormalities or metastases were observed over the proceeding 4-years of follow-up.
OUTCOME AND FOLLOW-UP
After comprehensive treatment, including partial surgical resection of his liver, lung, and colon, and palliative management such as systemic chemotherapy, TACE, targeted therapy with sorafenib, and cryotherapy, the patient is still alive and relatively healthy 8 years after being diagnosed with HCC.
DISCUSSION
HCC, a major subtype of primary liver cancer, is the third most common cause of cancer-related death worldwide,leading to over 600000 deaths annually[4]. While a significant amount of research has been performed into possible HCC treatments, it still carries an extremely dismal prognosis due to its late diagnosis and its high risk of recurrence and drug resistance. HCC always metastasizesviaintrahepatic blood vessels, direct infiltration, or the lymphatic system, and thus typically affecting the liver, lung, bone, lymphatics and brain[5]. Metastases to the digestive tract, in particular the colon are very rare. The patient underwent abdominal and pelvic exploration and irrigation for liver cancer with rupture and hemorrhage. It is worth considering whether the colon metastases occurredvianormal intestinal metastasis or abdominal implantation. We do not rule out the risk of intraperitoneal implantation, but consider the possibility of metastasis through the normal intestinal pathway to be more likely. First, the patient had successive liver, lung, and peritoneal metastases, with intestinal metastases occurring 2 years later. If the colonic metastases were due to peritoneal implantation, they would have occurred almost simultaneously with the abdominal metastasis. Further, the colonic metastases grew within the intestinal cavity rather than infiltrating it, as shown on imaging and colonoscopy. It is hard to distinguish metastatic carcinoma of the colon from primary colon cancer because the metastases have few specific clinical manifestations. Clinicians should therefore be vigilant to the possibility of rare metastatic tumor sites, such as the colon in the case of our patient, which may avoid misdiagnosis or delayed treatment.
There are many treatments for HCC, which include liver transplantation, surgical resection, locoregional therapy (e.g.,TACE), and systemic therapy (e.g., multikinase inhibitor sorafenib). Among the therapies mentioned above, liver transplantation and surgical resection remain the gold standard curative treatments for HCC. Locoregional and systemic therapies are usually considered controlling but not curative, or a means for decreasing tumor size or bridging the patient to surgery. It has been reported that patients treated with TACE have a considerably longer overall survival than the best supportive care in a randomized controlled study[6]. For patients with advanced HCC who are not surgical candidates or who have failed locoregional therapy, the multikinase inhibitor sorafenib may be considered[7]. An expanding body of evidence suggests that cytoreductive surgery can prolong the survival of patients with various metastatic malignancies and improve their quality of life[8,9]. Thus, despite their poor outcomes, the comprehensive treatment of patients with HCC and hepatic or extrahepatic metastases may improve their prognosis[10,11]. The comprehensive use of cytoreductive surgery, regional chemotherapy and other interventions contribute to lowering cancer burden, alleviating the symptoms and improving the quality of life of patients with metastatic HCC. However, patients with advanced HCC require a comprehensive assessment of multiple indicators. A specific preoperative assessment is therefore performed to identify appropriate treatment decisions. The postoperative pathological biopsy of this patient confirmed a moderately differentiated HCC. However, he developed liver, lung, peritoneum, and colon metastases at an early stage, classifying his diagnosis as advanced malignant HCC. According to the National Cancer Institute’s SEER database, the average fiveyear survival rate of HCC patients in the United States is 19.6%, but can be as low as 2.5% for those with advanced metastatic disease. Although this patient had a moderately differentiated HCC, an 8-year effective survival period should still be considered a longer than expected survival.
There are several deficiencies and omissions in this case. The absence of a well-developed PET-CT to most objectively identify the patient’s systemic lesions and metastases is a major weakness of this work. Further, it is a great pity that postoperative adjuvant therapy was administered earlier to this patient despite his high risk of recurrence.
CONCLUSION
In conclusion, this case describes a patient with atypical HCC with multiple extrahepatic metastases who survived for 8 years following comprehensive treatment. The primary HCC and metastatic tumors in his liver, lung, peritoneum, and colon were surgically removed. This may indicate that reducing the tumor burden may delay disease progression, thus improving quality of life. This report highlights the role of comprehensive treatment for certain patients with advanced stage HCC. It also supports the early recognition of rare metastatic sites and can provide instruction for the treatment of HCC.
FOOTNOTES
Author contributions:Gong YQ collected the literature and wrote the manuscript. Lu TL supervised the manuscript. Chen CW conceived the idea and drafted the manuscript. All authors have read and approve the final manuscript.
Informed consent statement:Informed consent statement was obtained from the patient and his family for publication of this report and any accompany images.
Conflict-of-interest statement:The authors declare no conflicts of interest.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Yong-Qiang Gong 0000-0002-9215-8790; Tai-Liang Lu 0000-0002-2156-5460; Chao-Wu Chen 0000-0001-5912-9050.
S-Editor:Yan JP
L-Editor:A
P-Editor:Yan JP
 World Journal of Gastrointestinal Surgery2023年8期
World Journal of Gastrointestinal Surgery2023年8期
- World Journal of Gastrointestinal Surgery的其它文章
- Initial suction drainage decreases severe postoperative complications after pancreatic trauma: A cohort study
- Vascular complications of chronic pancreatitis and its management
- Historical changes in surgical strategy and complication management for hepatic cystic echinococcosis
- Post-transplant biliary complications using liver grafts from deceased donors older than 70 years:Retrospective case-control study
- Goldilocks principle of minimally invasive surgery for gastric subepithelial tumors
- Prognosis after splenectomy plus pericardial devascularization vs transjugular intrahepatic portosystemic shunt for esophagogastric variceal bleeding