性别对HNPCC家系中hMLH1和hMSH2种系突变携带者患癌风险的影响
2011-06-08 08:55张渊智张志芳盛剑秋李世荣任艳敏高慧芳
胃肠病学和肝病学杂志 2011年6期
张渊智,张志芳,盛剑秋,李世荣,张 帆,任艳敏,杨 姝,高慧芳,冯 燕
1.昆明市第一人民医院消化科,云南昆明650011;2.河南省职工医学院附属医院麻醉科;3.北京军区总医院消化科
遗传性非息肉病性结直肠癌综合征(hereditary nonpolyposis colorectal cancer,HNPCC)是一种发病与错配修复基因种系突变密切相关的常染色体显性遗传性结直肠癌,与散发性结直肠癌相比较,具有影响因素单一、家庭聚集性和易于防治的特点。我们先前通过随访14个HNPCC中共222例hMLH1或hMSH2种系突变携带状态明确的家系成员,分析了hMLH1或hMSH2种系突变携带者患癌风险度[1-2],本研究探讨性别对HNPCC家系成员中错配修复基因种系突变携带者发生恶性肿瘤风险度的影响。
1 材料与方法
1.1 研究对象 14个HNPCC家系中共222例hMLH1或hMSH2种系突变携带状态明确的家系成员,其中94例为hMLH1或hMSH2种系突变携带者[1-2](见表1)。94例种系突变携带者中,59例发生结直肠癌,7例发生胃癌,1例发生胆囊癌,1例发生卵巢癌,1例发生皮肤癌;男64例,女30例。
1.2 方法
1.2.1 HNPCC家系成员调查表:所有被调查的HNPCC家系成员均填写HNPCC家系成员调查表,内容包括姓名、性别、出生日期、确诊结直肠癌的时间、家族恶性肿瘤史、个人恶性肿瘤史、肿瘤发生部位和数目、组织学类型等情况。所有参与调查的患者及家系成员均签署知情同意书。
1.2.2 诊断标准:Amsterdam标准Ⅰ(Amsterdam Criteria Ⅰ,ACⅠ)[2]、Amsterdam 标准Ⅱ(ACⅡ)[3]、日本标准(Japanese criteria for HNPCC,JC)[4]。对 Amsterdam标准Ⅱ中结直肠外肿瘤谱略作修改,包括胃癌、肝癌等临床上显示与HNPCC综合征相关的多种器官的恶性肿瘤。
1.3 统计学处理 采用SPSS 14.0统计软件包对资料进行描述性分析,计数资料的相关性分析、率或构成比的比较、相对危险度的计算等均采用χ2检验;突变携带者发生肿瘤的年龄相关累计风险度的计算与比较采用Kaplan-Meier方法、Cox风险比例模型和对数秩检验。显著性水准α=0.05,所有统计学检验均为双侧检验。累积风险度用均数和95%可信区间(confidence interval,CI)表示。
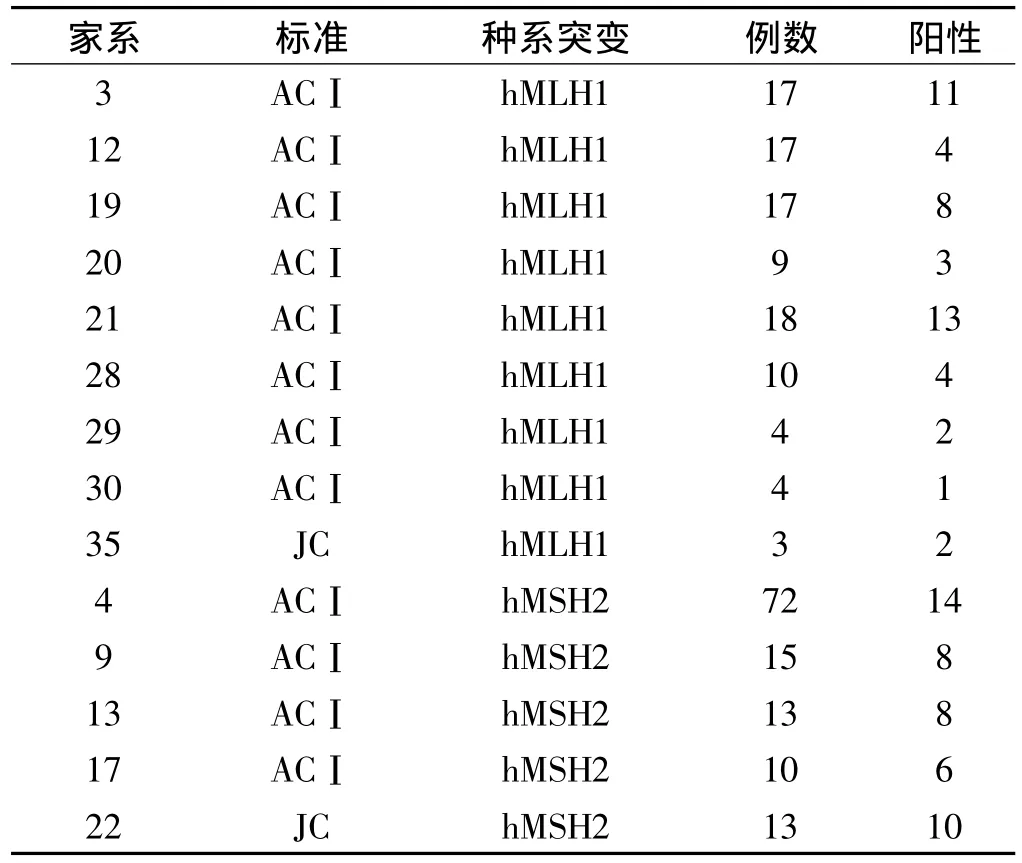
表1 14个HNPCC家系的临床诊断标准、突变基因及家系成员的突变携带情况Tab 1 Clinical criteria,mutation gene and mutation status of members in 14 HNPCC families
2 结果
2.1 错配修复基因种系突变携带者发生HNPCC相关恶性肿瘤的累积风险度与性别的关系 94例携带hMLH1或hMSH2种系突变的家系成员中,发生恶性肿瘤者共有67例(包括2例绒毛状腺瘤患者),男性携带者与女性携带者在30岁、40岁、50岁,60岁等年龄时发生HNPCC相关肿瘤的累积危险度如表2所示。如不考虑HNPCC相关恶性肿瘤的发生部位,男性与女性种系突变携带者在不同年龄的患癌累积风险度间具有非常显著性差异(χ2=7.74,P<0.01),男性携带者的患癌年龄较女性明显提前(见图1),但在60岁时两者基本趋于一致,均达90%以上;当肿瘤的发生部位为结直肠时,男性与女性种系突变携带者在不同年龄的患癌累积风险度间具有非常显著性差异(χ2=9.47,P<0.01),男性携带者结直肠癌的发病年龄较女性患者明显提前(见图2);当肿瘤的发生部位为胃时,男性与女性种系突变携带者在不同年龄的患癌累积风险度间的差异无统计学意义(χ2=0.34,P>0.05)。
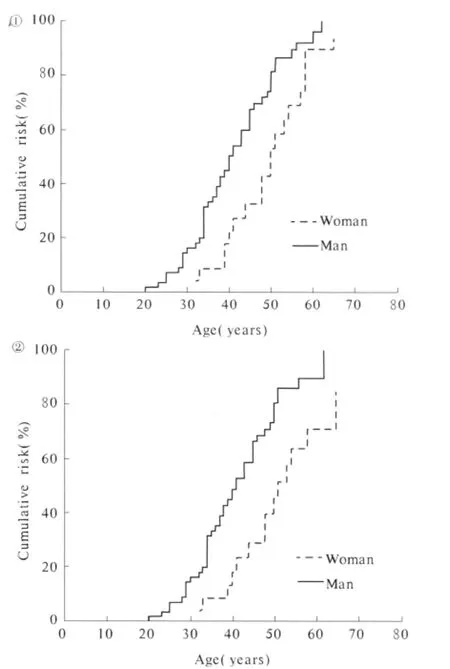
图1 不同性别的hMLH1或hMSH2种系突变携带者发生HNPCC相关肿瘤的年龄累积危险度;图2 不同性别的hMLH1或hMSH2种系突变携带者发生结直肠癌的累积危险度Fig 1 Cumulative cancer risk between man and woman hMLH1 or hMSH2 mutation carriers;Fig 2 Cumulative colorectal cancer risk between man and woman hMLH1 or hMSH2 mutation carriers
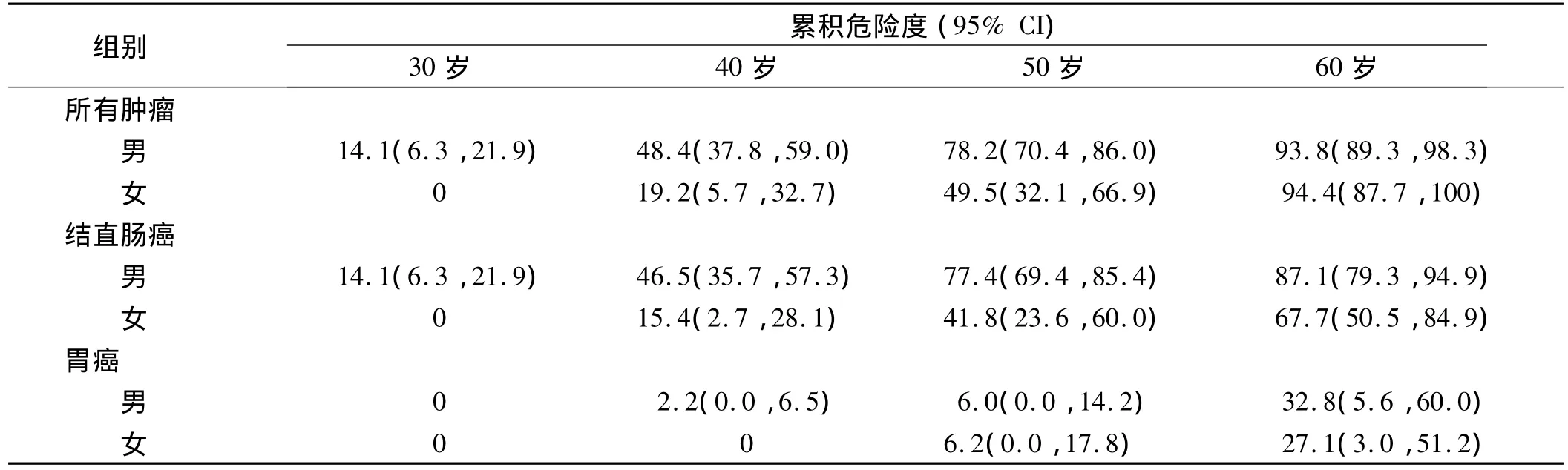
表2 不同性别的hMLH1或hMSH2种系突变携带者发生HNPCC相关恶性肿瘤的累积危险度(%)Tab 2 Cumulative cancer risk between man and woman hMLH1 or hMSH2 mutation carriers(%)
2.2 性别相同时hMLH1和hMSH2种系突变携带者发生HNPCC相关恶性肿瘤的累积风险度 在性别相同的hMLH1和hMSH2种系突变携带者,30岁、40岁、50岁和60岁等年龄时发生HNPCC相关肿瘤的平均累积危险度如表3所示。男性hMLH1和hMSH2种系突变携带者发生所有HNPCC相关恶性肿瘤的累积风险度间的差异无统计学意义(χ2=0.95,P>0.05);女性hMLH1和hMSH2种系突变携带者发生所有HNPCC相关恶性肿瘤的年龄累积风险度间的差异也无统计学意义(χ2=0.45,P>0.05)。hMLH1和 hMSH2种系突变携带者发生结直肠癌或腺瘤的累积风险度间的差异,在男性组(χ2=0.71,P >0.05)、女性组(χ2=2.18,P >0.05)均无统计学意义。
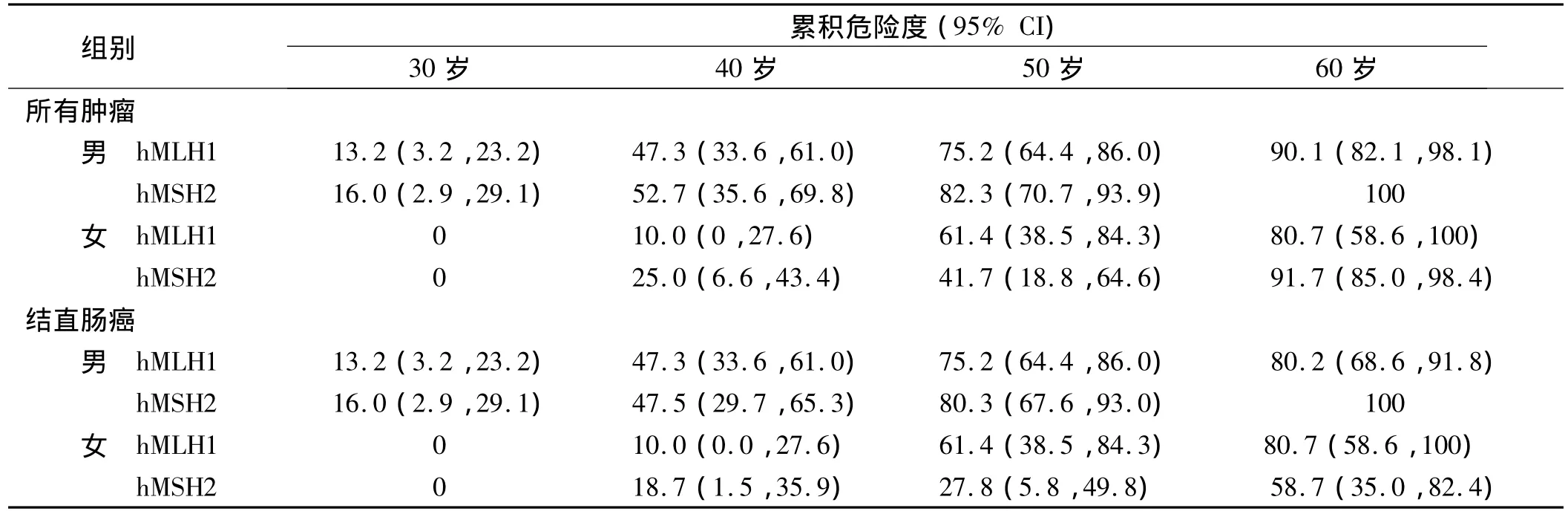
表3 性别相同时hMLH1和hMSH2种系突变携带者发生HNPCC相关恶性肿瘤的累积危险度(%)Tab 3 Cumulative cancer risk of hMLH1 and hMSH2 mutation carriers with the same sex(%)
3 讨论
HNPCC综合征又称Lynch综合征,是最常染色体显性遗传结直肠癌,在临床上以家族为单位发病,且大多数患者发生结直肠癌。国内外研究显示在所有结直肠癌患者中,符合Amsterdam标准Ⅰ的HNPCC患者发病率约为0.3% ~3%[5-12]。目前认为HNPCC的发病与错配修复基因种系突变密切相关,大约45%~92%的HNPCC家系可检出错配修复基因种系突变[3,13-17];其中 hMLH1 与 hMSH2 约占 90%左右[15-16,18-21]。与普通人群相比,发生HNPCC综合征的家系成员是发生恶性肿瘤尤其是结直肠癌的高危人群。国外研究表明错配修复基因种系突变对HNPCC家系成员发生恶性肿瘤及部位的风险度具有一定的预测作用[22-27]。国内类似研究报道较少。关于HNPCC家族成员中hMLH1与hMSH2种系突变携带者发生恶性肿瘤及不同部位肿瘤的风险度与性别的相关性,国外仅有少数研究报道[22,27-28],国内未见类似报道。
Barrow等研究发现,错配修复基因种系突变携带者在70岁时发生结直肠癌的累积风险度50.4%(95%CI:47.8% ~52.9%),男性携带者为 54.3%(95%CI:50.7% ~57.8%),明显高于女性携带者(46.3%,95%CI:42.8% ~49.9%,P=0.02)[28];女性突变携带者70岁时发生肠外肿瘤的累积风险度为47.4%(95%CI:43.9% ~50.8%),明显高于男性患者(26.5%,95%CI:22.6% ~30.4%,P <0.001),但男性携带者70岁时发生胃癌的累积风险度明显高于女性患者(P<0.001)[27]。本研究结果显示,在30岁、40岁、50岁、60岁等年龄点时,男性hMLH1或hMSH2种系突变携带者发生所有HNPCC相关恶性肿瘤的累积危险度较女性种系突变携带者高(P<0.01),男性携带者的发病年龄普遍较女性提前,但均在60岁时达到高峰,二者发病的平均累积危险度基本趋于一致。当肿瘤的发生部位为结直肠时,男性种系突变携带者在各个年龄点的累积危险度明显高于女性突变携带者(P<0.01)。在胃癌方面,男性与女性种系突变携带者发病的年龄相关累积风险度间的差异无统计学意义(P>0.05)。本研究结果与国外同类研究相似[22,27-28],但我国错配修复基因种系突变携带者发生各种HNPCC相关恶性肿瘤及结直肠癌的累积风险度均明显高于国外突变携带者,并且尽管女性突变携带者发病年龄虽较男性晚,但在60岁时二者发病的累积危险度均趋于一致。此外,我国男性与女性错配修复基因种系突变携带者发生胃癌的累积风险度亦较国外携带者高。原因可能与以下因素有关:① 我国HNPCC相关肠外肿瘤最常见的是胃癌[29],而国外最常见的则是子宫内膜癌,胃癌所占的比例较低[22,27-28]。②可能与人种有关。本组资料同时显示,在性别相同时hMLH1与hMSH2错配修复基因种系突变携带者患癌累积风险度间的差异无统计学意义(P>0.05),与国外研究相同[27-28]。
本研究提示,虽然男性错配修复基因种系突变携带者发生HNPCC相关恶性肿瘤的风险度较女性提前,但两者的发病风险度均在40岁时明显增加,并在60岁时发病的风险度均超过90%。因此在40岁以后要加强对HNPCC家系成员中错配修复基因种系突变携带者的随访力度,定期进行胃镜和肠镜检查,并且女性携带者要定期进行生殖器官检查,以达到肿瘤早期防治和最大限度节省医疗费用的目的。
[1]Zhang YZ,Sheng JQ,Chen B,et al.Screening of minor mutation of hMLH1 and hMSH2 based on denatured HPLCC [J].Progress In Modern Biomedicine,2008,8(12):2315-2320.张渊智,盛剑秋,陈彪,等.变性高效液相色谱法筛检hMLH1和hMSH2微小突变技术[J].现代生物医学进展,2008,8(12):2315-2320.
[2]Vasen HFA,Mecklin JP,Khan PM,et al.The International Collaborative Group on Hereditary Non-Polyposis Colorectal Cancer(ICGHNPCC)[J].Dis Colon Rectum,1991,34(5):424-425.
[3]Vasen HFA,Watson P,Mecklin JP,et al.New clinical criteria for hereditary nonpolyposis colorectal cancer(HNPCC,Lynch syndrome)proposed by the International Collaborative group on HNPCC[J].Gastroenterology,1999,116(6):1453-1456.
[4]Fujita S,Moriya Y,Sugihara K,et al.Prognosis of hereditary nonpolyposis colorectal cancer(HNPCC)and the role of Japanese criteria for HNPCC [J].Jpn J Clin Oncol,1996,26(5):351-355.
[5]Slattery ML,Levin TR,Ma K,et al.Family history and colorectal cancer:predictors of risk[J].Cancer Causes Control,2003,14(9):879-887.
[6]Olsson L,Lindblom A.Family history of colorectal cancer in a Sweden county[J].Fam Cancer,2003,2(2):87-93.
[7]Evans DG,Walsh S,Jeacock J,et al.Incidence of hereditary non-polyposis colorectal cancer in a population-based study of 1137 consecutive cases of colorectal cancer[J].Br J Surg,1997,84(9):1281-1285.
[8]Aaltonen LA,Salovaara R,Kristo P,et al.Incidence of hereditary nonpolyposis colorectal cancer and the feasibility of molecular screening for the disease[J].N Engl J Med,1998,338(21):1481-1487.
[9]Peel DJ,Ziogas A,Fox EA,et al.Characterization of hereditary nonpolyposis colorectal cancer families from a population-based series of cases[J].J Natl Cancer Inst,2000,92(18):1517-1522.
[10]Katballe N,Christensen M,Wikman FP,et al.Frequency of hereditary non-polyposis colorectal cancer in Danish colorectal cancer patients[J].Gut,2002,50(1):43-51.
[11]Cornaggia M,Tibiletti MG,Albarello L,et al.Low incidence of hereditary nonpolyposis colorectal cancer syndrome in a selected area of the Lombardy Cancer Registry [J].Tumori,2000,86(6):439-444.
[12]Zhang YZ,Sheng JQ,Li SR,et al.Hereditary predisposition of colorectal cancer and prevalence of hereditary nonpolyposis colorectal cancer in general population of colorectal cancer patients in China[J].Natl Med J China,2005,85(42):2995-3000.张渊智,盛剑秋,李世荣,等.中国部分地区结直肠癌遗传易感性与遗传性非息肉病性结直肠癌流行状况分析[J].中华医学杂志,2005,85(42):2995-3000.
[13]Järvinen HJ.Genetic testing for polyposis:practical and ethical aspects[J].Gut,2003,52 Suppl 2:ii19-ii22.
[14]Wagner A,Barrows A,Wijnen JT,et al.Molecular analysis of hereditary nonpolyposis colorectal cancer in the United States:high mutation detection rate among clinically selected families and characterization of an American founder genomic deletion of the MSH2 gene[J].Am J Hum Genet,2003,72(5):1088-1100.
[15]Bisgaard ML,Jager AC,Myrhoj T,et al.Hereditary non-polyposis colorectal cancer(HNPCC):phenotype-genotype correlation between patients with and without identified mutation[J].Hum Mutat,2002,20(1):20-27.
[16]Lynch HT,Lynch JF,Lynch PM,et al.Hereditary colorectal cancer syndromes:molecular genetics,genetic counseling,diagnosis and management[J].Fam Cancer,2008,7(1):27-39.
[17]Sheng JQ,Chan TL,Chan YW,et al.Microsatellite instability and novel mismatch repair gene mutations in northern Chinese population with hereditary non-polyposis colorectal cancer[J].Chin J Dig Dis,2006,7(4):197-205
[18]Peltomaki P.Deficient DNA mismatch repair:a common etiologic factor for colon cancer[J].Hum Mol Genet,2001,10(7):735-740
[19]Peltomaki P,Gao X,Mecklin JP.Genotype and phenotype in hereditary nonpolyposis colon cancer:a study of families with different vs.shared predisposing mutations [J].Fam Cancer,2001,1(1):9-15.
[20]Cai Q,Sun MH,Fu G,et al.Mutation analysis of hMSH2 and hM-LH1 genes in Chinese hereditary nonpolyposis colorectal cancer families[J].Chin J Pathol,2003,32(4):323-328.蔡崎,孙孟红,付刚,等.中国人遗传性非腺瘤病病性结直肠癌家系hMSH2和hMLH1基因突变分析[J].中华病理学杂志,2003,32(4):323-328.
[21]Liu SR,Zhao B,Wang ZJ,et al.Clinical features and mismatch repair gene mutation screening in Chinese patients with hereditary nonpolyposis colorectal carcinoma[J].World J Gastroenterol,2004,10(18):2647-2651.
[22]Watson P,Lynch HT.Cancer risk in mismatch repair gene mutation carriers[J].Fam Cancer,2001,1(1):57-60.
[23]De Jong AE,Morreau H,Van Puijenbroek M,et al.The role of mismatch repair gene defects in the development of adenomas in patients with HNPCC[J].Gastroenterology,2004,126(1):42-48.
[24]Vasen HF,Stormorken A,Menko FH,et al.MSH2 mutation carriers are at higher risk of cancer than MLH1 mutation carriers:a study of hereditary nonpolyposis colorectal cancer families[J].J Clin Oncol,2001,19(20):4074-4080
[25]Hendriks YM,Wagner A,Morreau H,et al.Cancer risk in hereditary nonpolyposis colorectal cancer due to MSH6 mutations:impact on counseling and surveillance[J].Gastroenterology,2004,127(1):17-25.
[26]Syngal S,Bandipalliam P,Garber J,et al.Clinical presentation correlates with the type of mismatch repair gene involved in hereditary nonpolyposis colon cancer[J].Gastroenterology,2004,126(3):936-937.
[27]Barrow E,Robinson L,Alduaij W,et al.Cumulative lifetime incidence of extracolonic cancers in Lynch syndrome:a report of 121 families with proven mutations [J].Clin Genet,2009,75(2):141-149.
[28]Barrow E,Alduaij W,Robinson L,et al.Colorectal cancer in HNPCC:cumulative lifetime incidence,survival and tumour distribution.A report of 121 families with proven mutations[J].Clin Genet,2008,74(3):233-242.
[29]Zhang YZ,Sheng JQ,Li SR,et al.Clinical phenotype and prevalence of hereditary nonpolyposis colorectal cancer in Chinese population[J].World J Gastroenterol,2005,11(10):1481-1488.
猜你喜欢
现代临床医学(2022年4期)2022-09-29
中华实用诊断与治疗杂志(2022年1期)2022-08-31
中国临床医学影像杂志(2022年5期)2022-07-26
中老年保健(2021年12期)2021-08-24
宁夏医学杂志(2020年4期)2021-01-21
医学与法学(2020年3期)2020-09-18
现代消化及介入诊疗(2019年4期)2019-05-28
吉林林业科技(2018年6期)2018-11-21
故事作文·高年级(2017年3期)2017-04-12
听力学及言语疾病杂志(2015年5期)2015-12-24