
Strategic planning and designing of a hospital disaster manual in a tertiary care, teaching, research and referral institute in India
2014-03-17 11:00ShwetaTalatiPrateekBhatiaAshokKumarGuptaColOjha
Shweta Talati, Prateek Bhatia, Ashok Kumar, A. K. Gupta, Col. D Ojha
1Department of Hospital Administration, Post Graduate Institute of Medical Education and Research, Chandigarh, India
2Department of Pediatrics, Post Graduate Institute of Medical Education and Research, Chandigarh, India
3All India Institute of Medical Sciences, Rishikesh, India
Corresponding Author:Shweta Talati, Email: shwetatalati@gmail.com
Strategic planning and designing of a hospital disaster manual in a tertiary care, teaching, research and referral institute in India
Shweta Talati1, Prateek Bhatia2, Ashok Kumar3, A. K. Gupta1, Col. D Ojha1
1Department of Hospital Administration, Post Graduate Institute of Medical Education and Research, Chandigarh, India
2Department of Pediatrics, Post Graduate Institute of Medical Education and Research, Chandigarh, India
3All India Institute of Medical Sciences, Rishikesh, India
Corresponding Author:Shweta Talati, Email: shwetatalati@gmail.com
BACKGROUND:As per the "Disaster Management Act, 2005" of India, it is mandatory for government hospitals in India to prepare a disaster plan. This study aimed to prepare a disaster manual of a 1 900 bed tertiary care hospital, in consultation and involvement of all concerned stakeholders.
METHODS:A committee of members from hospital administration, clinical, diagnostic and supportive departments worked on an initial document prepared according to the Act and gave their inputs to frame afinal disaster manual.
RESULTS:The prepared departmental standard operating procedures involved 116 people (doctors and paramedical staff), and were then synchronized, in 12 committee meetings, to produce thefinal hospital disaster manual.
CONCLUSIONS:The present disaster manual is one of the few comprehensive plans prepared by the stakeholders of a government hospital in India, who themselves form a part of the disaster response team. It also helped in co-ordinated conduction of mock drills.
Disaster Management Act; Disaster manual; Hospital administration; Stakeholders; Mock drills
INTRODUCTION
Disasters pose unique challenge for every medical care facility in terms of infrastructure, capacity and preparedness. From the hospital's point of view, a disaster exists when the patient load far exceeds the capabilities of a emergency department to provide emergency care and the hospital is forced to apply additional resources for providing care to a large number of victims.
The Indian sub-continent is a disaster prone area, with 59% of land vulnerable to earthquakes, 8.5% to cyclones, and 5% to floods.[1]As a result of disasters, less than 1 million houses are damaged annually.[1]The National Disaster Management Act (NDMA, India), 2005 is mandatory for all hospitals in India to have a disaster management contingency plan.[2]The components of a disaster response cycle include response, rescue, recovery, mitigation, risk reduction, prevention and preparedness. The most important component of the cycle is proactive with a contingency plan to deal with the disaster, and in hospitals it includes preparation of a disaster manual that addresses the action plan. However, before preparation of a disaster manual, it is important to remember a few key elements of the disaster plan (Table 1). Moreover, the hospital disaster plan should also cater to internal disaster scenarios like majorfire, major power failure, employee strike or internal building damage/collapse.
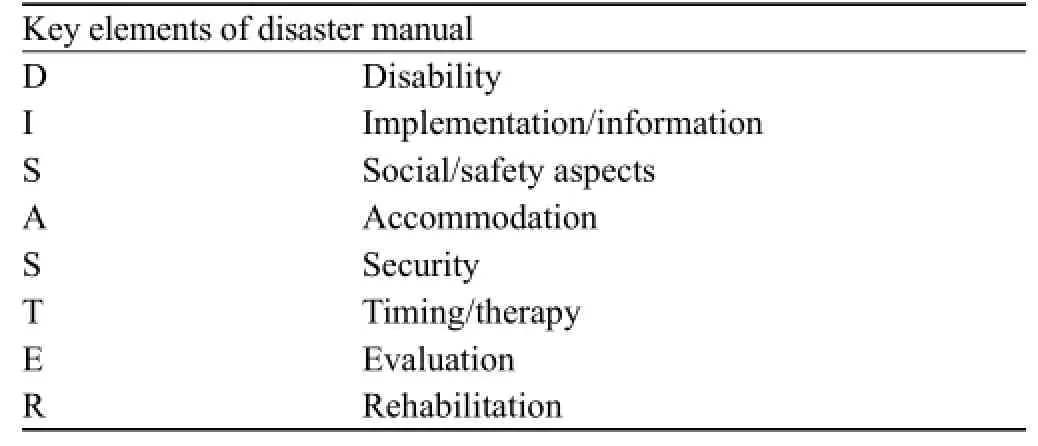
Table 1. The key elements of a disaster manual
The objectives of the present study were to prepare a disaster manual of a tertiary care hospital with 1 900 beds involving all stakeholders and to execute the contingency plan during disaster drill to observe and analyze the shortcomings.
METHODS
The disaster manual was prepared in two phases:
Strategic planning phase
This phase included the following actions: i) Formulation of the Hospital Disaster Control Committee; ii) Clinical, non-clinical and supportive departments involved in the committee; iii) Laying down of objectives; iv) Preparing a general document according to the guidelines defined in the National Disaster Management Act, 2005; and v) meetings for defining the roles of the members of the committee.
Designing phase
This phase included the following actions: i) Inviting inputs from the clinical, non-clinical and supportive departments in form of their intra-departmental Standard Operating Procedures (SOPs); ii) Presentations of each departmental SOPs to the committee members, followed by critical analysis, discussion, modification or restructure if required and then acceptance; iii) Interdepartmental synchronization of SOPs and incorporation into main hospital disaster document; iv) Designing of comprehensive flow charts to address both external and internal disasters; v) Surprise conduct of mock-drills and re-evaluation of SOPs with additions, substitutions or modifications. The disaster contingency plans were classified as per the NDMA, 2005[2]as follows: class A: The plan which can contain an event of disaster without any disruption of normal routine and work; class B: With minor disruption to routine work; class C: Major readjustment with increased demand on human and material resources.
RESULTS
The 116 hospital staff, including senior and junior consultants, technicians, nurses and residents were involved in preparing the final disaster manual. They included 10 members each from 5 clinical departments, 6 members each from 6 diagnostic departments, 2 officers each from 12 support services and 7 members from the administration (Table 2). A total of three committee meetings in the strategic planning phase and nine in the designing phase were held tofinalize the hospital disaster manual.
In the strategic planning phase meetings, the step wise details of processes involved were as follows:
1. Constitution of the Hospital Disaster Control Committee: The committee is chaired by the medical superintendent (MS) of the institute, who also acts as the chief of operations during disaster. The other members include deputy medical superintendents as member conveners, senior faculty representatives from the departments of neurosurgery, general surgery, internal medicine, orthopedics and anesthesia. In addition, the committee comprises chief security officer (CSO), chief nursing officer (CNO), sanitation officer (SO) and head engineer services. The main responsibility of the committee is to decide and document the prevention & mitigation tactics as per the threat perception, situational and SWOT analysis of the organizational capability.
2. Laying down of objectives to be achieved: The main goals are to document a plan to enable all designated personnel to enact their roles and responsibility in a smooth and coordinated manner with the goal to achieve maximum efficiency. Thefinal plan is needed to fulfill the following objectives:
a) To define the role and responsibility of different responders;
b) To inform each respondent about their roles and responsibilities;
c) To identify and assess the vulnerability of PGIMER to external and internal disasters and how to deal with them;
d) To document disaster activation and deactivation plan;
e) To identify methods of communication inside the facility as well as with outside agencies;
f) To promote development of SOPs in respect of each department and development of job action cards;
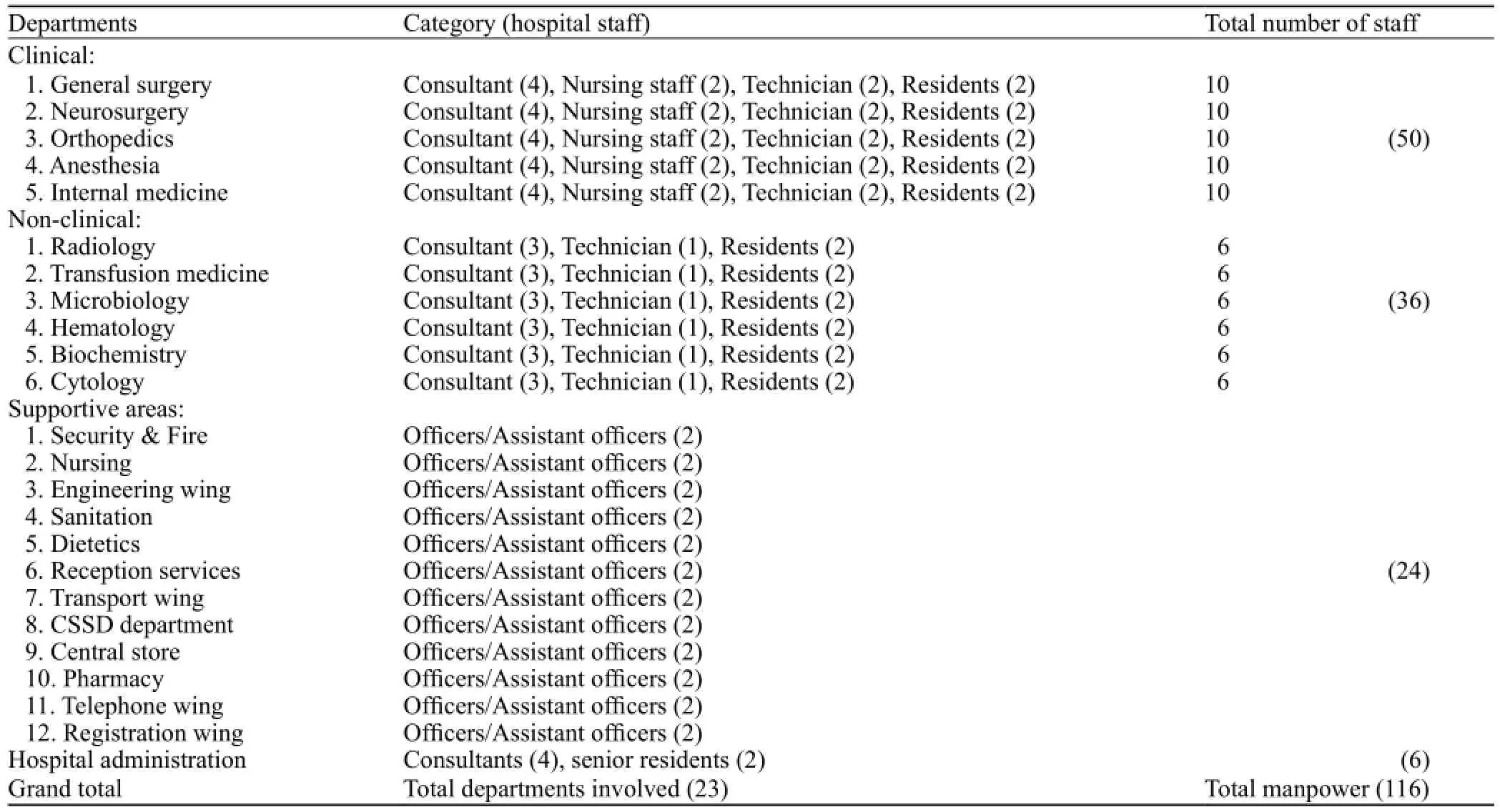
Table 2. Members (committee-wise) involved in planning and designing of hospital disaster manual
g) To classify contingency plan for disaster response;
h) To promote ,enhance, and sustain capacity building.
3. Preparing a general guiding document according to the guidelines of NDMA, 2005: An extensive review of the literature was made by a hospital administration department resident on various policies, plans and documents available online regarding hospital disaster response.[2–8]These documents and plans were analyzed, and a general guiding document was prepared as a dissertation, taking into account PGIMER infrastructure, facility, lay-out and capacity. This was placed before the committee members for deliberation and further refinement. The key components of the disaster draft plan include:
a) Classification of contingency plans into classes as A, B and C as per NDMA guidelines.
b) Activation and deactivation of plan – Alert/Standby/Call out & Stand down messaging to all responders via the group SMS system
c) Identification of disaster control rooms/incident command centers: Main command center in medical superintendent office to receive continuous feedback on the situation and to control various hospital activities. The office will keep the disaster duty roasters and job action sheets of all departments and support services of the institute.
d) Establishing communication with external agencies like other government and private hospitals Union Territory (UT) Health Administration and Police cell.
e) Media management and crowd management and control: To be attended by public relation officer and chief security officer respectively.
f) Triage and shifting policies: The heads of the departments of orthopedics, general surgery, neurosurgery to constitute triage, resuscitation and treatment teams. They will be composed of at least two senior residents, staff nurses, nursing interns and hospital and sanitary attendants. Patients to be prioritized, as per tags, by the triage team in a separate area within emergency complex and then assessed by the resuscitation or treatment teams.
g) Evacuation plans for internal disaster: Details of all exit routes to be used for patients shifting and transfer. The exits should be kept free of any obstructions and the duty of fire officers to ensure their functioning and maintenance.
h) Maintaining directory of key internal and external contacts like other government and private hospitals in region, non-governmental organizations, red cross society, UT health, police posts, DNAfinger printing and diagnostic labs, etc.
i) List of vital equipments like ventilators, defibrillators, suction machines, intravenous pumps and poles to be maintained by chief nursing officers along with theirnumbers and distribution areas. A separate cabin to be kept as a disaster cabinet within emergency complex for storage of vital drugs, injectables, personal protective equipments, dressings, gowns and other related material, under direct supervision of deputy nursing superintendent incharge of emergency.
j) Plan for conduction, observation and analysis of disaster mock drills.
k) Outline for post disaster recovery, education and training.
In the designing phase, intra-departmental SOPs were invited from 5 clinical departments (general surgery, neurosurgery, orthopedics, snesthesia & critical care, and internal medicine), 6 non-clinical departments (radiology, transfusion medicine, medical microbiology, biochemistry, cytology and hematology) and 12 supportive services (hospital engineering services, security & fire services, nursing wing, sanitation department, central sterile supply department, dietetics unit, pharmacy, central stores, reception wing, registration wing, transport unit, and telephone services) of the hospital. The SOPs from all services and departments had the following information in common:
(i) The details of staff on standby duty during disaster and their contact numbers;
(ii) The roles and responsibilities of all concerned staff;
(iii) The coordination between related services and departments during disaster (eg. between general surgery and neurosurgery).
The SOPs were presented by the respective department stakeholders in the committee meetings and further structured, streamlined and synchronized by inputs from the committee members. These were then incorporated into the main common disaster draft and afinal disaster manual was prepared. The final manual was placed before the committee for approval and it was suggested to review the same based on outcomes from mock drill disaster tests. A total of two disaster mock drills were conducted after framing the manual and the analysis revealed shortcomings in the areas of relay of information according to line of command, communication gap between different response teams and lack of awareness of complete contingency plan amongst the stakeholders. To address these shortcomings, the hospital administration department designed three comprehensive flow charts to detail the roles and responsibilities of concerned staff during external, internal and epidemic (infectious disease) disasters (Figures 1–3). The hospital disaster manual review and updating was decided tobe done annually. The updating of key information about contact numbers, vital equipment details, etc was assigned to chief nursing officer. The regular updating of intra-departmental SOPs with regard to any change in manpower/contact details was notified to committee chairperson (MS) office and copy of any such changes was then circulated to committee members during routine meetings. After theirfinal approval, the changes were suggested to be incorporated into the main manual.
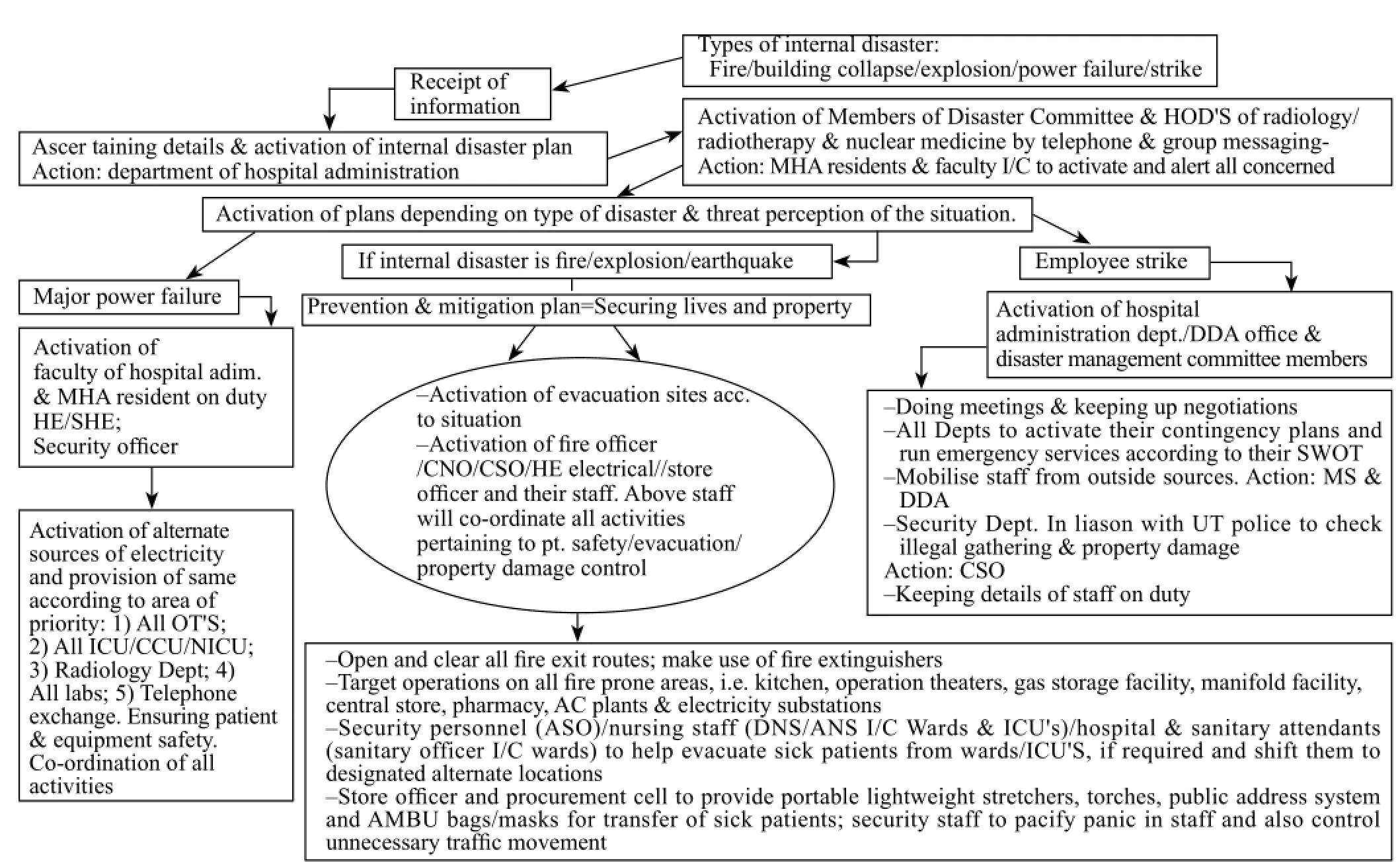
Figure 1. Roles and responsibilities during internal disaster.
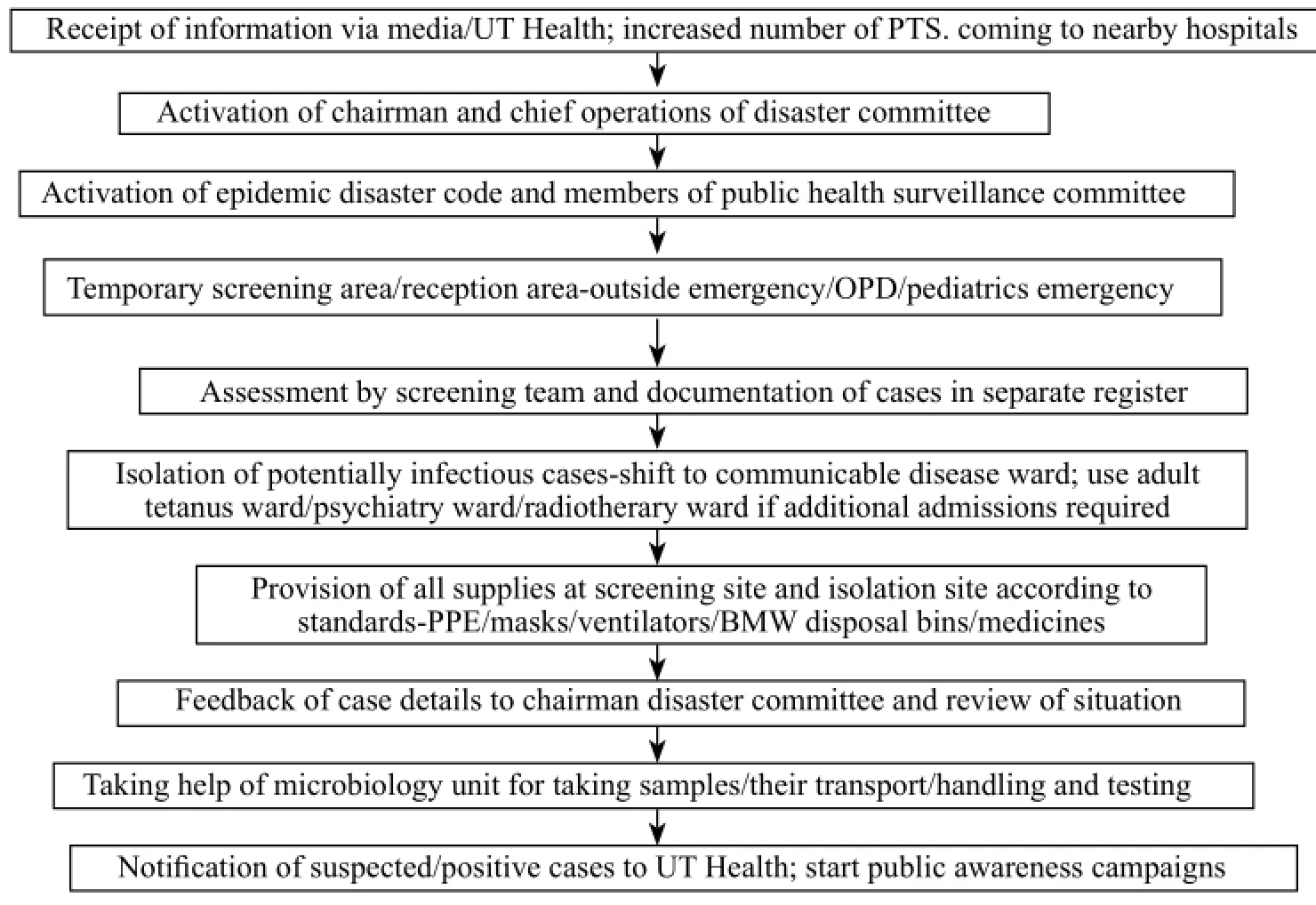
Figure 2. Roles and responsibilities during epidemic (infectious disease) disaster.
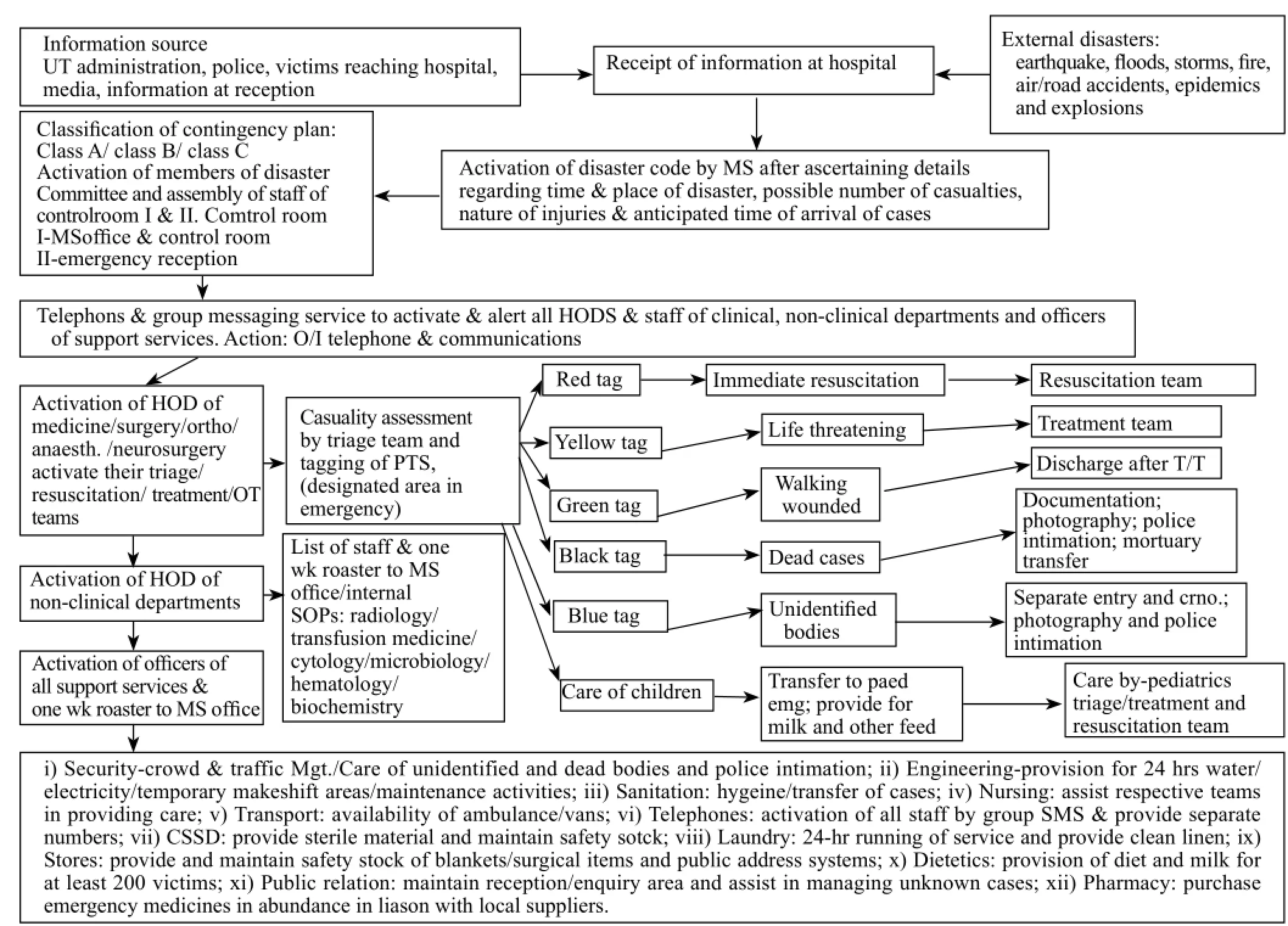
Figure 3. Roles and responsibilities during external disaster.
A comparison of key information, as provided in the disaster manual, of few international hospitals[3,4]and those formulated by Indian government hospitals[5,6]was also made with the present manual. It was noted that all the plans addressed both important internal and external disasters, had detailed outlines of roles and responsibilities of all departments and services and were subjected to a system of review and updating. However, the disaster plans of Indian hospitals, including our plans failed to properly address chemical, biological and nuclear disasters. In addition, our disaster manual is a more comprehensive manual in terms of well defined SOP plans, in form of flow charts, of each department (both clinical and basic) and support service of the institute.
DISCUSSION
The present disaster manual is one of the few comprehensive disaster response plans prepared by the stakeholders of a government hospital in India, who themselves form a part of the disaster response team. The key components of the plan included defining the flow of patients and keeping the triage area near the disembarkation point, earmarking treatment room, resuscitation room, and area for centralized incident command center, devising an effective communication system via group SMS/Phone, maintaining safety stock in predetermined disaster cabinets in emergency wards, provision for early identification and isolation of contaminated/infected patients, and ensuring effective co-ordination with other hospitals and non-governmental organizations and creation of an information desk at the reception for addressing families and media.
The importance of hospital preparation and response to mass causalities has also been emphasized.[9,10]The plan and design of a disaster manual for a hospital require an extensive review of hospital infrastructure, workforce, materials and resources.[11]The policy-making should be based on capacity and layout of the hospital. The main issues during the process of planning included irregular representation by committee members of clinical and surgical departments because of their clinical, academic and personal reasons, lack of awareness of the importance of disaster address and usually delayed among support service staff, erratic and uncoordinated meetings of the committee. The process, however, streamlined on intervention and active involvement of MS and issuance of instructions on importance of disaster control by repeated reminders. The committee meetings were allowed to be attended by any other concerned departmental nodal officer if the active member of the committee was a senior faculty and was unavailable to attend all routine meetings. The issues during designing phase included lack of expertise on part of most departmental and support service staff on preparation of SOPs in form of structuredflow charts. This resulted in unnecessary delays in final manual preparation. The presentation of SOPs during committee meetings was not timely done by few of departments and services and hence extra meetings had to be called for.
The present study also included the assessment and overview of the hospital disaster plan by mock disaster drills. Two such drills were conducted with complete secrecy as to their nature. The first drill revealed glaring gaps in spread of information along the defined line of command/authority and communication failure in the response of the resuscitation and treatment teams. The supportive staff and hospital administration department was however proactive in controlling the situation to a certain extent. These problems lead the disaster control committee to review its contingency plan by doing a SWOT analysis of the disaster manual after the first drill (Table 3), and create awareness in the concerned staff as to their roles and responsibilities during the event of a disaster. As a result, easy to follow and practice flow charts, addressing internal, external disasters and epidemics were prepared by the hospital administration department for information to the concerned stakeholders. This was followed by a rereview of the preparedness in a second drill two months later. The second drill was quiet effective in terms of level of response, communication and proactiveness of the concerned staff and only minor issues needed addressal.
The manual was also updated with information regarding the key internal and external personnel contacts, details of safety cabinet supplies, details of emergency equipments as to their number and distribution areas, evacuation routes in case of internal disasters, contacts and addresses of regional and state hospitals and forensic labs and patient information cards.
In cinclusion, the hospital disaster manual should be subject to continuous review and update for effectiveimplementation. The hospital disaster manual should be prepared with involvement of all concerned stakeholders and should be widely circulated and made available to all concerned individual officials, offices and departments. Mock drills should be routinely conducted to assess the hospital preparedness and adequate measures should be taken to address the gaps in contingency plan.
ACKNOWLEDGEMENT
We are grateful to all the members of the Hospital Disaster Control Committee and the stakeholders involved in the planning and designing of the manual.
Funding:None.
Ethical approval:Not needed.
Conflicts of interest:We have no conflicts of interest to the study.
Contributors:Dr. Talati, Dr. Bhatia and Dr. Ojha developed the intellectual content of the manuscript and participated in writing, reviewing and editing. Dr. Gupta and Dr. Kumar did the manuscript review and editing.
REFERENCES
1 An introduction to the vulnerability atlas of India: A tool to natural disaster prevention, preparedness and mitigation for housing and related infrastructure. Building materials and technology promotion council, Ministry of housing and urban poverty alleviation, government of India (First revision), 2006.
2 The Disaster Management Act, 2005. The Ministry of Law & Justice (Legislative Department), government of India, 2005.
3 Hospital disaster plan, Wisconsin Hospital, USA. Available online at: http://www.dhfs.state.wi.us/rl_dsl/hospital/ hospitaldisastrplng.htm.
4 Wayne P Chesbro. Disaster medical care: The basic hospital disaster plan. California Medicine 1961; 95: 371–373.
5 Disaster plan for AIIMS hospital. Available online at: http:// www.searo.who.int/LinkFiles/Hospitals_Safe_from_Disasters_ Document20.pdf.
6 Disaster management plan for Sir J.J. group of hospitals, Mumbai. Available online at: www.grantmedicalcollegejjhospital.org/disaster.pdf.
7 Shakti K Gupat. Overview of health services disaster plan. Workshop on integrating hospitals safe from disasters. Available online at: www.jkhealth.org.
8 Safe hospitals in emergencies and disasters: Structural, nonstructural and functional indicators. WHO 2010 document. Available online at: www.wpro.who.int/emergencies_disasters.
9 Kaushal M, Banta RK, Sen RK, Chhabra MS, Bahadur R. Hospital preparedness status in mass casualty management. Ind J Orthopedics 2000; 34: 112–114.
10 Milsten A. Hospital responses to acute-onset disasters: A review. Prehosp Disaster Med 2000;15: 32–45.
11 Bechtel GA, Hansberry AH, Gray-Brown D. Disaster planning and resource allocation in health services. Hosp Mater Manage Q 2000; 22: 9–17.
Received July 20, 2013
Accepted after revision December 11, 2013
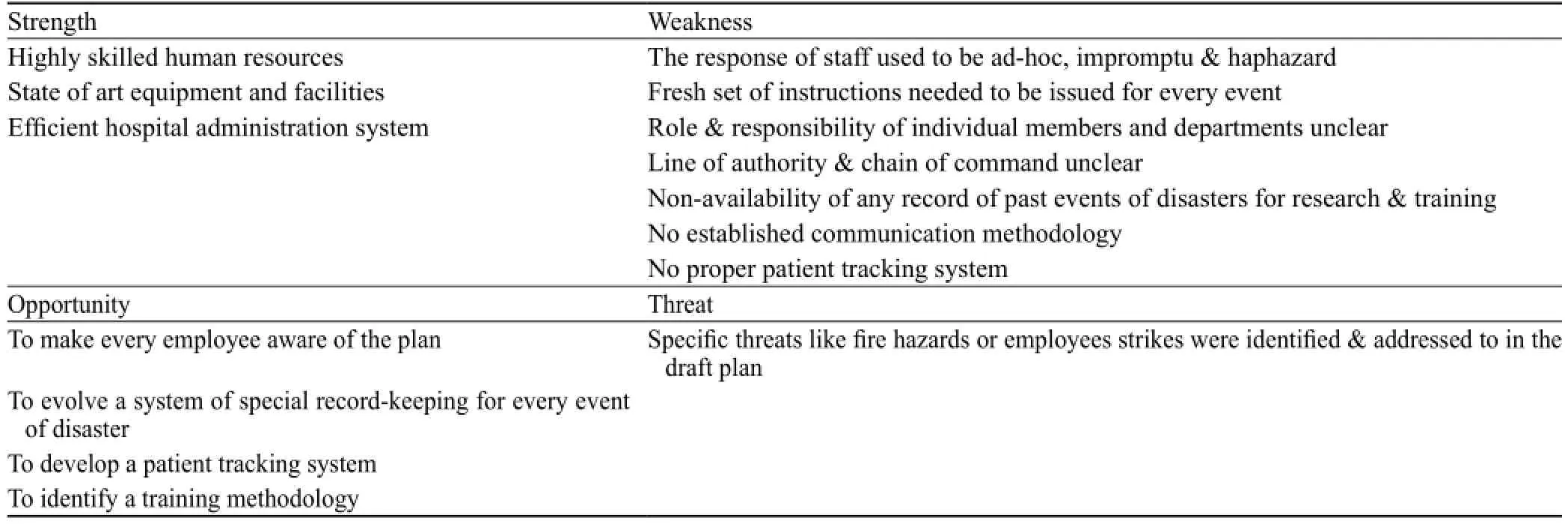
Table 3. SWOT analysis of disaster manual afterfirst drill
World J Emerg Med 2014;5(1):35–41
10.5847/ wjem.j.issn.1920–8642.2014.01.006
 World journal of emergency medicine2014年1期
World journal of emergency medicine2014年1期
- World journal of emergency medicine的其它文章
- Wilderness medicine
- Lean techniques for the improvement of patients'flow in emergency department
- The knowledge level offinal year undergraduate health science students and medical interns about cardiopulmonary resuscitation at a university teaching hospital of Northwest Ethiopia
- Effects of early rehabilitation therapy on patients with mechanical ventilation
- Bispectral index in predicting the prognosis of patients with coma in intensive care unit
- Significance of blood pressure variability in patients with sepsis