
Suicide in India: a systematic review
2014-12-09 06:28AnilRANEAbhijitNADKARNI
上海精神医学 2014年2期
Anil RANE*, Abhijit NADKARNI
•Systematic review•
Suicide in India: a systematic review
Anil RANE1*, Abhijit NADKARNI2,3
suicide, India, systematic review, organophosphate pesticide, mental illness
1. Introduction
Suicide is the final outcome of complex interactions of biological, genetic, psychological, sociological and environmental factors. It is an increasingly important public health issue: from 1990 to 2010 the number of global suicides increased by 32%. It is particularly important among young adults 15 to 49 years of age among whom it accounts for 4.8% of all female deaths and 5.7% of all male deaths.[1]Eighty-four percent of global suicides occur in low and middle-income countries (LMICs); India and China alone account for 49% of global suicides.[2]There is substantial variability both in the prevalence of suicide and in the factors that influence the occurrence of suicide between geographic regions, cultures, and over time, so countryspecific analyses are needed to develop targeted suicide prevention efforts.
The World Health Organization (WHO) estimates that of the nearly 900,000 people who die from suicide globally every year, 170,000 are from India.[3]However,India’s National Crime Records Bureau (NCRB) – which report official suicide rates based on police reports –estimated only 135,000 suicides in 2011.[4,5]One possible reason for under-reporting of suicide by the NCRB is that suicide remains a crime in India.[6]Detailed independent verbal autopsy investigations of all unnatural deaths in several rural areas of the country report suicide rates that are up to five-fold higher than the official national average.[7]Despite the importance of suicide both as a health problem and as a social problem, the issue receives little attention from Indian policy makers. This neglect of the issue is reinforced by cultural influences,religious sanctions, stigmatization of the mentally ill,competing political imperatives, and socio-economic factors.[8]
This systematic review aims to provide a more balanced assessment of the prevalence and correlates of suicide in India by identifying and integrating all available reports on the subject.
2. Methods
We searched the following electronic databases:PubMed, PsycINFO, EMBASE, Global Health, Google Scholar and IndMED (database of articles published in Indian biomedical journals). The combination of search terms (in the title or abstract fields) used included‘suicide’ OR ‘suicidal’ OR ‘suicidality’ OR ‘hanging’ OR‘drowning’ OR ‘self-poisoning’ OR ‘overdose’ OR ‘selfinjury’ AND ‘India’ OR ‘Indian’. The titles of the papers identified through the database search were screened and the abstracts of papers that reported on suicide or self-harm in India were retrieved. These abstracts were examined and the full text of papers that reported on the prevalence or correlates of suicide or self-harm were retrieved. These full texts were then examined to determine their compliance with the following eligibility criteria: papers published prior to June 2012 that reported the prevalence or correlates of suicide in any part of India for either gender in any age group. The reference lists of selected papers were hand-searched for additional eligible papers, but no additional paperswere identified. The screening and selection of papers was independently conducted by both authors; in the cases where different papers were selected the paper was re-assessed and discussed by both authors to arrive at a consensus decision.
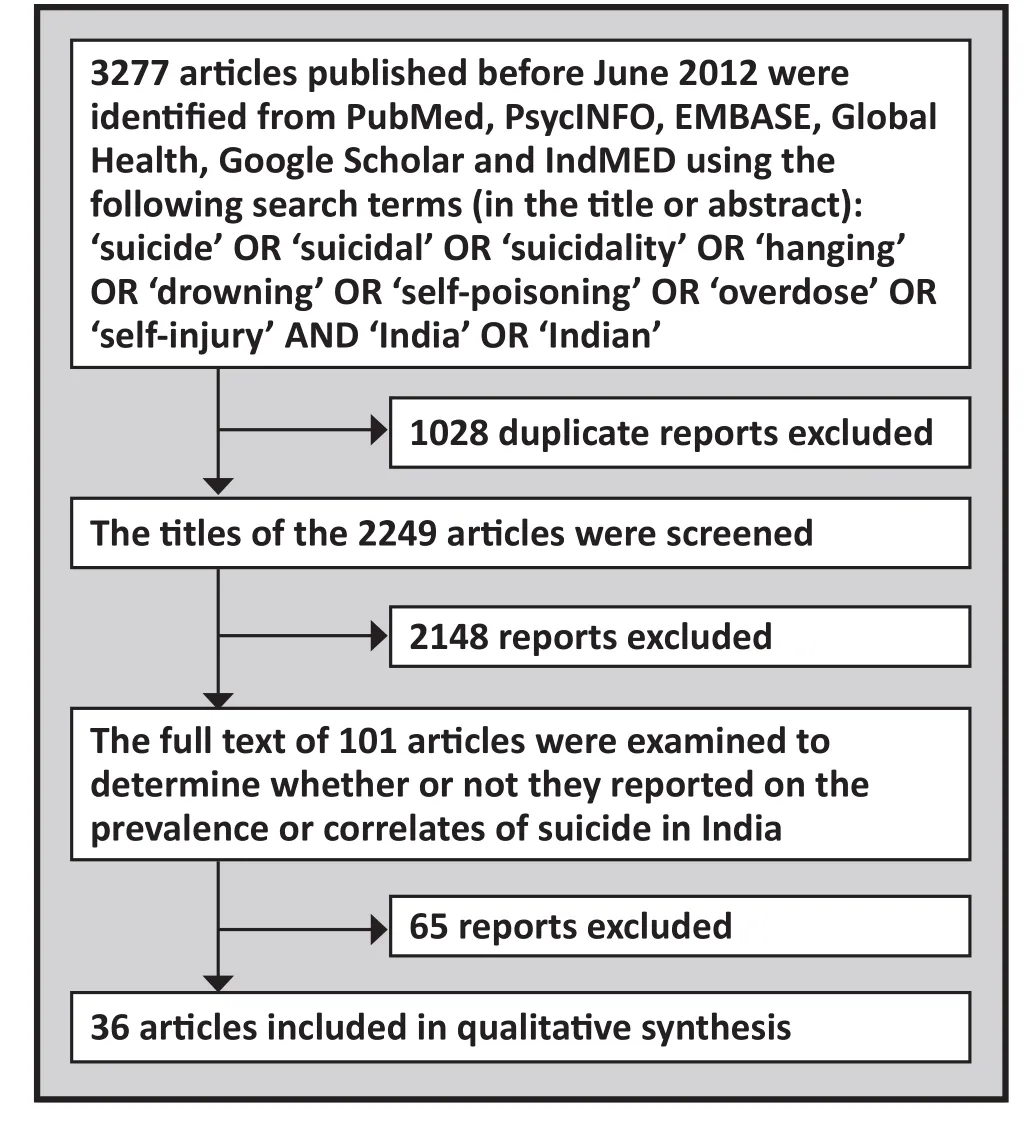
Figure 1. Flowchart of identification of articles
We extracted the following data from included papers: date of publication, study design, setting, center(state, city), methods, sampling technique, sample size, definition of suicide, prevalence, and correlates of suicide. Data extraction was conducted by one reviewer(AR). We present the results as prevalence rates and, where available, corresponding 95% confidence intervals (CI).
3. Results
The selection of included articles is shown in Figure 1.Thirty-six papers were selected for the review, of which 6 were published between 1971 and 1980, 3 between 1981 and 1990, 3 between 1991 and 2000, and 24 between 2001 and 2010. Thirty papers were about cross sectional surveys, 3 were case control studies and 3 were ecological studies. Details of the studies are shown in Table 1. The studies were conducted in different parts of the country and used different sampling strategies and settings. Most studies either used verbal autopsy(i.e., interviewing family informants and other associates of the deceased) or the integration of multiple sources of information about a death to determine whether or not a death should be classified as a suicide –methods that are generally considered to be reliable.Some studies were part of ongoing community-based surveillance efforts that provided population based rates; but other studies did not specify their sampling strategies or had non-random sampling designs, making it difficult to assess the validity of the reported results.
3.1 Prevalence of suicide
A community-based surveillance system using verbal autopsy covering a population of 108,000 in a rural development block of Tamil Nadu (one of the more highly developed states in southern India) has been operating for several decades.[22,26,33,35,36]Several reports have appeared using these data. The prevalence of suicide for the period from 1994 to 1999 was 95 per 100,000 population (annual rates ranged from 84 to 106 per 100,000) accounting for 8 to 12% of all deaths.[23]From 2000 to 2002 the average suicide rate was 92 per 100,000 (112 in men and 72 in women) accounting for 9.8 to 11.4% of all deaths.[36]For the period from 1998 to 2004 the average suicide rate was 82 per 100,000.[35]In young people 10 to 19 years of age, over the 10-year period from 1992 to 2001 the average male suicide rate was 58 per 100,000 (accounting for 25% of all deaths)and the average suicide rate for women was 148 per 100,000 (accounting for 50 to 75% of all deaths).[26]Over the same 10-year period, the mean suicide rate in persons 55 years of age or older was 189 per 100,000.[33]
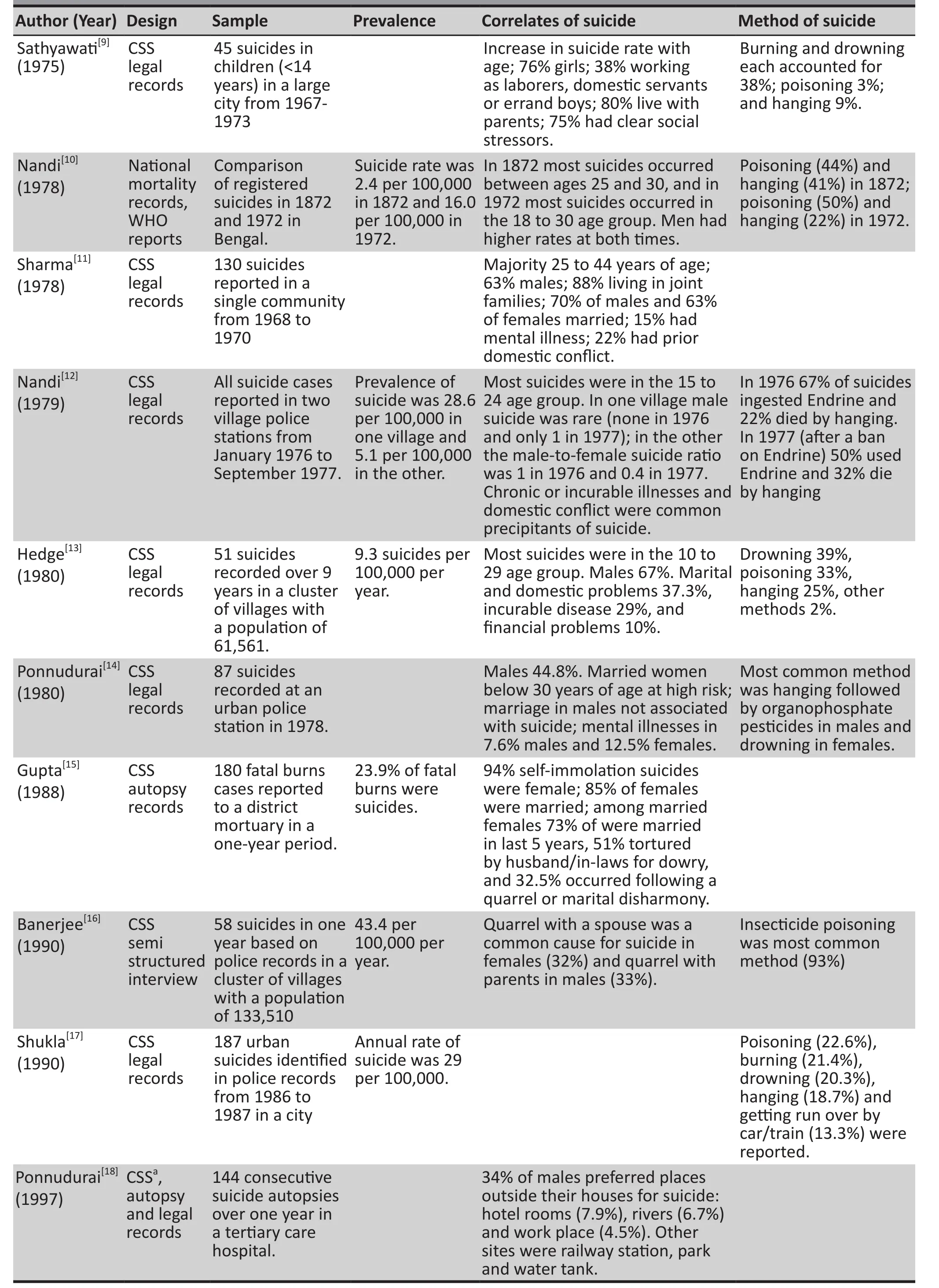
Table 1. Description of reviewed studies

Table 1. Description of reviewed studies (continued)
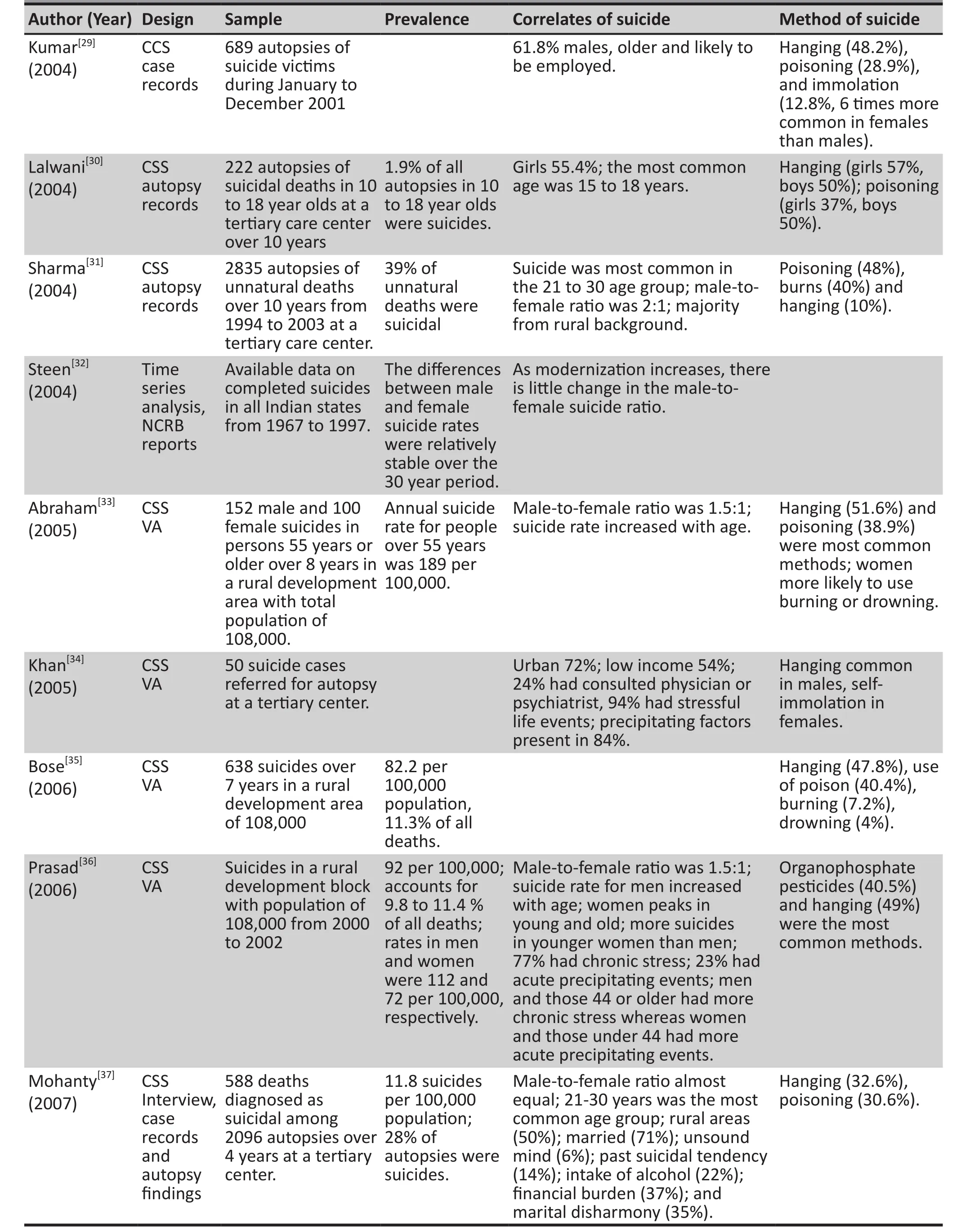
Table 1. Description of reviewed studies (continued)
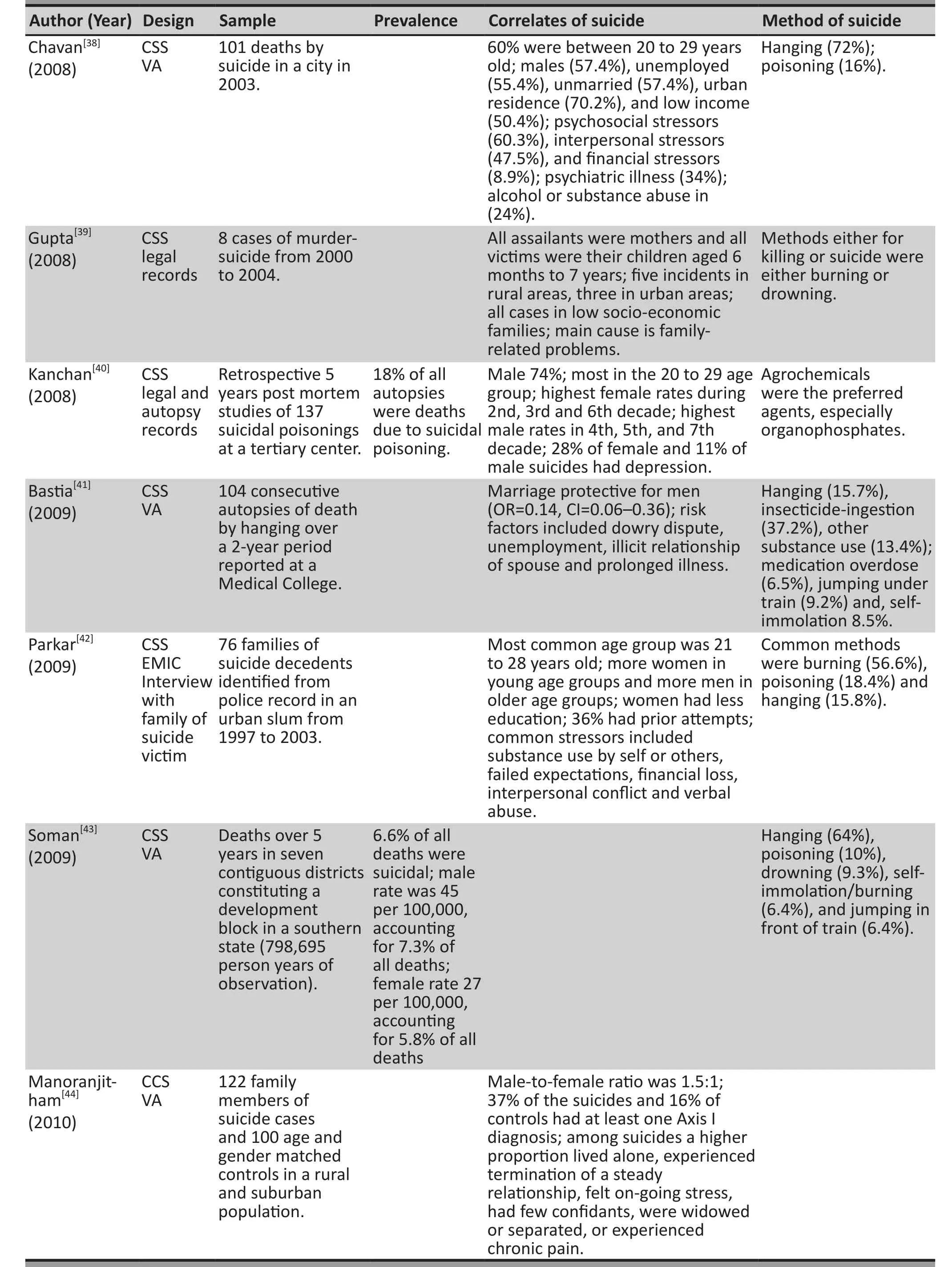
Table 1. Description of reviewed studies (continued)
A prospective community-based cohort study of cause of death in the south Indian state of Kerala from July 2002 to June 2007 reported a male suicide rate of 45 per 100,000 and a female suicide rate of 27 per 100,000, which collectively accounted for 6.6% of all deaths.[43]A retrospective, 4-year autopsy-based study by Mohanty and colleagues reported a suicide prevalence of 12 per 100,000 population.[37]Other autopsy studies[24,27,31,37]with sample sizes ranging from 2096 to 2835 report that the proportion of suicidal deaths among all autopsies ranged from 28 to 39%. A large (n=11,583), 10-year retrospective autopsy study published in 2004 by Lalwani and colleagues reported that 1.9% of all autopsies were suicides in individuals 10 to 18 years of age.[30]An earlier 7-year autopsy study reported in 1975 by Sathyawati and colleagues reported that among 1834 autopsies of suicide decedents, 45(2.4%) were children 14 years of age or younger.[9]
3.2 Methods of suicide
Hanging was the most frequently reported method of suicide in most of the studies, accounting for 10 to 72%of all suicides.[13,14,17,19,20,26,28,29,31,33-35,37,38,42,43]The second most frequently reported method was self-poisoning(often ingestions of organophosphate pesticides), which accounted for 16 to 49% of all suicides.[13,16,17,19,26,28,29,31,33-35,37,38,42,43]The proportion of all suicides attributed to drowning ranged from 3 to 39%[13,17,19,26,35,43]and the proportion attributed to burning or self-immolation ranged from 6 to 57%.[17,19,26,28,29,31,34,35,38,42,43]Other reported methods of suicide include jumping off heights(0.5 to 2% of all suicides),[17,19,38]being run over by a train(6 to 13% of all suicides)[17,43]and using a fi rearm (3% of all suicides).[17]
Some studies report gender-based differences in method preference. A community-based surveillance study by Prasad and colleagues reported in 2006 found that significantly more women chose drowning and burning as modes of suicide than men, while significantly more men chose hanging.[36]A similar pattern of gender-based method preference was reported by Abraham and colleagues among persons 55 years of age and older.[33]Other studies report higher rates of suicides by hanging in males than females,[17,34,42]a predominance of males in suicide decedents who use other violent methods[17,34](e.g., jumping in front of a train), and a predominance of females among suicides by self-immolation.[17,33]
3.3 Correlates of suicide
3.3.1 Age
Suicides in the third decade of life (i.e., in persons 20 to 29 years of age) account for 41 to 62% of all suicides.[13,16,17,28,31,34,37,38,42]Among older adults, the age-specific suicide rate increases with age: it is 137 per 100,000 for persons 55 to 64 years of age, 204 for persons 65 to 74 years of age, and 331 for persons 75 years of age or older.[33]Studies among children under 18 years of age also found that suicide rates increase with age,[9,30]with the highest rate in the oldest children (i.e., those 15 to 18 years of age).
Age related trends differ by gender. The mean (sd) age of suicides as reported by Bastia and colleagues in 2009 was 32.5 (13.6) in males and 25.9 (8.7) in females.[41]Other studies have also reported higher mean age among male versus female suicide decedents (28.9 [12.6] v. 24.6 [10.5];p<0.02).[17]In the community-based surveillance study in rural Tamil Nadu, the suicide rate for men increased with age while the suicide rate for women had two peaks, one between 15 and 24 years of age and the other over 65 years old.[36]Several studies have reported higher suicide rates among younger women than younger men and higher suicide rates among older men than among older women.[14,21-23,25,40-42]A prospective 5-year cohort study reported that the age-specific male to female ratio of suicide rates ranged from 0.4 in the youngest age group (i.e. 0 to 14 years) to 4.5 in the 45 to 54 age group.[43]
3.3.2 Gender
The evidence for differences in the rate of suicide by gender is inconsistent. Some studies report that a higher proportion of suicides are male (57 to 74%)[11,13,20,31,36,38,40]while others report that a higher proportion of suicides are female (56 to 79%).[14,16,41]Still other studies report that there is no significant difference in the proportion of suicides by gender.[37]Reports based on the community surveillance data in Tamil Nadu indicate that the male-to-female gender ratio (combining all age groups) has been stable over the last 30 years, ranging from 1.3:1 to 1.5:1 (i.e., an excess of males).[21,32,36]As discussed above, the male-to-female gender ratio of suicide rates is lower than 1 (i.e., a predominance of females) in the young age groups and greater than 1 (i.e.,a predominance of males) in the middle and older age groups.
3.3.3 Marital status
Most studies report that the majority of suicide decedents were married at the time of death (57 to 73%),[11,17,20,24,37,41,44]but two studies reported that a higher proportion of suicide decedents were unmarried(52 to 58%).[34,38]In one prospective study of suicide autopsies, male suicide decedents were more likely to be single (60.5%) while female suicide decedents were more likely to be married (73.8%); marriage was protective in males (OR=0.1, 95% CI=0.1–0.4), but not in females.[41]In a case series of suicidal deaths,being married put women – particularly women under 30 years of age – at a higher risk of suicide, but this was not the case for men.[14]One case control study found a much higher risk of suicide in persons who are widowed, separated or divorced compared to persons who are currently married (13% v. 1%; p=0.003)[19]; this finding was supported by another study that found that being separated or widowed was significantly associated with suicide (OR=2.9, 95% CI=1.1-7.7).[44]
3.3.4 Education
Evidence for the association of education and suicide is inconsistent. In one study, individuals who were illiterate or less educated were at significantly higher risk of suicide (χ2=44.33, p<0.001),[37]a finding that was also reported in two studies that had female-only samples.[17,42]However, a psychological autopsy study reported that a larger proportion of subjects had completed high school(33%) or college (25%).[38]
3.3.5 Occupation
The association of occupation to suicide is also inconsistent. In a psychological autopsy of suicides, 55%were unemployed and a further 40% were semiskilled workers.[38]In a community based study, most of the women who completed suicide (54%) were housewives.[42]In a study of suicides among children (i.e.,under 14 years of age), 38% were working as daily wage laborers, domestic servants or errand boys.[9]
3.3.6 Socioeconomic status (SES)
There are fairly consistent reports of higher suicide rates in persons of low SES. Low SES was reported in 50 to 66% of suicide victims.[34,38,42,44]A case control study[28]reported that 35% of suicides occurred in households with monthly incomes of less than 3000 rupees (about 50 $US) and another 35% occurred in households with incomes of 3001 to 6000 rupees (50 to 100 $US).Another control study reported that low socio-economic status was an independent risk factor for suicide.[37]
3.3.7 Residence
In a psychological autopsy study in the city of Chandīgarh, 70% of the identified suicide decedents were from an urban background, 10% were from rural areas, and 20% from suburban areas.[38]In this study,57% of the identified suicide decedents had migrated from other parts of India and abroad. One study reported that 50% of suicide decedents were from rural areas,[37]and another reported a rural-to-urban ratio of suicide decedents of 1.4:1.[24]
3.3.8 Psychological stressors
The common stressors associated with suicides included interpersonal difficulties (especially conflicts with spouse or other family members),[11,13,16,22,26,27,37,38,42]psychosocial stress,[11,24,26,27,38,42]financial problems,[11,13,22,27,37,38,42]chronic illnesses,[11,13,22,27,41]domestic violence,[22,26,41,42]work-related problems,[11,27,38,41,42]extramarital relationships,[11,22,41]legal problems,[38]academic difficulties,[26,27]living alone,[44]and other types of stressful life events.[19,28,34,44]
One multivariate analysis of the independent role of various psychosocial stressors as risk factors for suicide[28]reported that longstanding alcohol abuse (odds ratio=4.8, 95% CI 1.9-12.8), absence of social support networks (3.1, 95% CI 1.1-8.5) and limited resources(11.5, 95% CI 4.6-28.8) were independent risk factors for suicide. Factors considered in the study that were not significantly associated with suicide included presence of a mental illness (1.6, 95% CI 0.4-2.5), emotional abuse(2.6, 95% CI 0.1-56.2) and prior experience of physical violence (1.8, 95% CI 0.4-8.1).[28]Another multivariate analysis[44]identified on-going stress (odds ratio=97.7,95% CI 27.8-3343.2) and chronic pain (66.1; 95% CI 5.0-873.5) as important risk factors for suicide.
3.3.9 Mental illness
The prevalence of any psychiatric illness among suicide decedents varied based on the source of the data: psychological autopsy studies reported a 34%prevalence of mental disorders in suicide decedents,case series studies reported a prevalence of 24% and studies based on police records reported a prevalence ranging from 5 to 25%.[11,14,22,37,38,40]
Several studies found that the presence of a current mental disorder increased the risk of suicide(odds ratios range from 3.1 to 19.5).[19,28,44]Several specific conditions were associated with elevated risk for suicide: alcohol consumption (odds ratio=4.5, 95%CI=3.0-6.8), a history of chronic alcohol abuse in self(23.4, 95% CI=12.9-43.7), a history of chronic alcohol abuse in one’s spouse (6.1, 95% CI=2.5-15.4),[28]alcohol dependence (2.8, 95% CI=1.0-6.8), adjustment disorders(3.4, 95% CI=1.2-9.6)[44]and personality disorder (9.5,95% CI=2.3-84.1).[19]
4. Discussion
Understanding a complex phenomenon like suicide in a country as diverse as India through studies of varying strengths and limitations is quite a challenge. As of June 2012 we could not find a single pan-India study investigating the prevalence or correlates of suicide. The sampling strategies and methodologies of the 36 studies we identified were quite heterogeneous so it was not possible to conduct a meta-analysis that would integrate the fi ndings.
There are, however, some trends that emerge from this qualitative review of the available literature.Suicides in India are largely under-reported; the rates reported in the papers identified for this review are likely to be underestimates. Hanging and self-poisoning,especially with organophosphate pesticides, are the most common methods of suicide. The young,particularly young women are at a high risk of suicide.Low socioeconomic status, interpersonal stressors and the presence of mental illness are important risk factors for suicide. There is insufficient evidence to draw conclusions about the importance of education, marital status, residence or employment status as potential risk factors for suicide.
Based on results of a nationally representative mortality survey implemented by the Registrar General of India between 2001 and 2003, the estimated rate of suicide in persons 15 years of age or older in 2010 was 22 per 100,000 population, accounting for 3% of all deaths in persons 15 or older.[6]Large scale verbal autopsy studies of all deaths fi nd that the suicide rates in rural areas are three- to four-fold higher than those reported by the government.[45]The reported annual rates of suicide per 100,000 population by the NCRB from 2008 through 2012 were 10.8, 10.9, 11.4, 11.2 and 11.2, respectively.[46]These official government figures– which are about half those identified in the Registrar General mortality study – clearly underestimate the magnitude of the problem. The stigma associated with suicide and the criminalization of suicides under Indian law both deter reporting, and, thus, lead to serious under-estimation of the suicide rate.
The availability of specific means for suicide affects national patterns of suicide methods. In the United States, firearms are used in most suicides[47]while in countries with large rural populations such as China and the Republic of Korea pesticides are the most common method.[35,48]In Australia, Japan, New Zealand, Pakistan,and Thailand, hanging dominates while in Hong Kong and Singapore, jumping (typically from tall apartment buildings) is the most frequent method used.[49,50]Our review found that hanging was the most common method of suicide in India closely followed by selfpoisoning, especially with organophosphate pesticides.In the Registrar General mortality study about half of suicide deaths were due to poisoning (mainly ingestions of pesticides) and hanging was the second most common method.[6]The Registrar General study also reported that burning (self-immolation) was a relatively common method of suicide in women, accounting for one-sixth of all female suicides.[6]India has the dubious distinction of having the highest absolute number of self-immolation cases, the highest fatality rate from self-immolation, and the highest proportion of hospital admissions for burns that are due to self-immolation.[51]
Our review clearly indicates that the young in India are at a high risk of suicide, a finding that is consistent with the Registrar General mortality study and the NCRB data.[4,6]In the Registrar General mortality survey, 40%of suicide deaths in men and 56% in women occurred between the ages of 15 and 29. A 15-year-old individual in India had a cumulative risk of 1.3% of dying by suicide before the age of 80.[6]
Although our review could not demonstrate a clear gender difference in risk for suicide, many of the reviewed studies reported an overall male excess when combining suicides across all age groups. However,several of the studies also reported a higher prevalence of suicide in females than males in the younger age groups. This gender difference is in keeping with that seen in other Asian countries. Unlike in most European countries and the United States, where male suicides far outnumber female suicides (3:1 to 4:1),[52]in most Asian countries the ratio is much lower, and in China the ratio actually falls below 1:1 (i.e., there are more female suicides than males suicides).[53]The higher rates of female suicide in Asian countries may be linked to the position of women in the traditionally patriarchal societies of Asia. Niaz and Hassan[54]argue that “women’s lack of empowerment and both financial and emotional dependence have restricted their self-expression and choices in life. This, along with family, social and work pressures, has a definite impact on women’s mental health.”
Though not unequivocal, our review found that female suicide decedents were more likely to be married and male suicide decedents were more likely to be single. The peak in the suicide rates for females was in the 15 to 29 age group, which coincides with the traditional age for marriage for Indian females.Cultural attitudes toward the woman’s role in marriage may partially explain the comparatively higher ratio of female to male suicides found in Asian countries compared to those in Europe and the United States.In countries like India, Pakistan and Sri Lanka where arranged marriages are common, the social and familial pressure on a woman to stay married even in abusive relationships may be one of the factors that increases the risk of suicide in women.[28]Dowry-related suicides are not uncommon in India; when dowry expectations are not met young brides can be harassed to the point where they are driven to suicide.[55]
The data related to the potential role of educational status as a risk factor for suicide identified in the review was ambiguous so no clear correlation could be established. However, the evidence about a relationship between low socioeconomic status and suicide was more robust. India is experiencing rapid socio-economic changes and a related widening of the gulf between the rich and the poor. In both high-income and low- and middle-income countries suicide rates tend to be higher in the subgroups of the population that are unable to realize the aspirations engendered by economic prosperity, those who remain in chronic poverty,unemployment and debt.[28,45,56,57,58]
The available studies do not provide a definitive answer about the relationship of location of residence and suicide, but there do appear to be higher suicide rates in rural versus urban areas both in India and in other countries with large agricultural populations.[4,6,45]If true, the likely explanations for the higher suicide rates in rural areas would include rapid migration,economic hardship, lack of social support, isolation,relatively easy access to lethal means (e.g., pesticides)and the lack of high-quality resuscitation services.[45,59]
Interpersonal conflicts, particularly those with family members, were the most common type of stressors associated with suicide identified in the studies considered in this review. Asian countries have traditionally been characterized by the centrality of extended family systems, dependence on the family,and the subjugation of individual concerns to the needs of the family. However, rapid economic development,social transformation and globalization are changing the role of the family and the relationships between the individual and the family in many of these countries. These changes are engendering new types of interpersonal conflicts as traditional expectations of families encounter modern aspirations of individuals.As just one of several markers of cross-cultural differences in the psychological valence of interpersonal risk and protective factors for suicide, the suicideprotective effect of being married reported in highincome countries does not appear to be confirmed in studies from India and China, where single individuals are no more vulnerable to suicide than their married counterparts.[53,60]
Psychological autopsy studies conducted in developed countries report that psychiatric disorders are present in about 90% of people who die by suicide and that these conditions contribute 47 to 74% of the population attributable risk of suicide.[61,62]In our review mental illness – particularly alcohol use disorders –were also important risk factors for suicide, but not to the extent reported in high-income counties. Almost all studies from high-income countries indicate that affective disorder (i.e., depression and mania) is the mental disorder most closely associated with suicide(followed by substance abuse and schizophrenia)[61,63]and that more than half of all people who die of suicide meet current diagnostic criteria for an affective disorder.[64]This review suggests that depression plays a less dominant role in suicide in India. Other studies fi nd that in Asian cultures impulse control disorders are stronger predictors of suicidal behavior than affective disorders.[65]
5. Conclusion
The quality of the information about suicide in India is quite limited, but the picture drawn from the eclectic mix of studies identified in this review indicate that it is an important and growing public health problem that is not being given sufficient attention by the government or the society at large. Compared to the pattern of suicides in high-income countries, suicide in India is more prevalent in women (particularly young women), is much more likely to involve ingestion of pesticides, and is more closely associated with poverty and less closely associated with mental illness. Initial targets for suicide prevention in India should include:(a) decriminalization of suicide; (b) restricting access to pesticides; and (c) improving the monitoring of fatal and non-fatal suicidal behavior.
Conflict of Interest
The author reports no conflict of interest related to this manuscript.
Funding
The authors did not receive any funding support to conduct this review.
1. Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet.2012;380: 2095-2128. doi: http://dx.doi.org/10.1016/S0140-6736(12)61728-0
2. Phillips MR, Cheng HG. The changing global face of suicide. Lancet. 2012;379: 2318-2319. doi: http://dx.doi.org/10.1016/S0140-6736(12)60913-1
3. World Health Organisation. The Global Burden of Disease:2004 update. Geneva: WHO; 2008
4. National Crime Records Bureau. Accidental Deaths and Suicide in India. New Delhi: Government of India; 2011
5. National Crime Records Bureau. Accidental Deaths and Suicides in India. New Delhi: Government of India; 2008
6. Patel V, Ramasundarahettige C, Vijayakumar L, Thakur JS,Gajalakshmi V, Gururaj G et al. Suicide mortality in India: a nationally representative survey. Lancet. 2012;379: 2343-2351. doi: http://dx.doi.org/10.1016/S0140-6736(12)60606-0
7. Gajalakshmi V, Peto R. Suicide rates in rural Tamil Nadu,South India: verbal autopsy of 39 000 deaths in 1997–98. Int J Epidemiol.36: 203-207. doi: http://dx.doi.org/10.1093/ije/dyl308
8. Vijayakumar L, Pirkis J, Huong TT. Socio-economic, cultural and religious factors affecting suicide prevention in Asia.In: Hendin H, Phillips MR, Vijayakumar L, eds. Suicide and Suicide Prevention in Asia. Geneva: World Health Organization; 2008: 19-30
9. Sathyavathi K. Suicide among children in Bangalore. Indian J Pediatr. 1975;42: 149-157. doi: http://dx.doi.org/10.1007/BF02827289
10. Nandi D, Banerjee G, Boral G. Suicide in West Bengal-A Century Apart. Indian J Psychiatry. 1978;20: 155-160
11. Sharma SD, Gopalakrishna R. Suicide-a retrospective study in a culturally distinct community in India. Int J Soc Psychiatry. 1978;24: 13-18. doi: http://dx.doi.org/10.1177/002076407802400103
12. Nandi D, Mukherjee S, Banerjee G, Ghosh A, Boral G,Chowdhury A et al. Is suicide preventable by restricting the availability of lethal agents ? a rural survey of West Bengal.Indian J Psychiatry.1979;21(3): 251-255. doi: http://dx.doi.org/10.4103/0019-5545.75553
13. Hedge RS. Suicide in rural community. Indian J Psychiatry.1980;22:368-70
14. Ponnudurai R, Jeyakar J. Suicide in Madras. Indian J Psychiatry. 1980;22: 203-205
15. Gupta R, Srivastava A. Study of fatal burns cases in Kanpur(India). Forensic Sci Int. 1988;37: 81-89. doi: http://dx.doi.org/10.1016/0379-0738(88)90096-5
16. Banerjee S, Chowdhury AN, Schelling E, Brahma A, Biswas MK, Weiss MG. Deliberate self-harm and suicide by pesticide ingestion in the Sundarban region, India. Tropical Medicine& International Health. 2009;14: 213-219. doi: http://dx.doi.org/10.1111/j.1365-3156.2008.02199.x
17. Shukla G, Verma B, Mishra DN. Suicide in Jhansi City. Indian J Psychiatry. 1990;32: 44-51
18. Ponnudurai R, Patnaik K, Sathianathan R, Subhan K. A study of the venues of Suicide. Indian J Psychiatry. 1979;39(1): 34-36
19. Vijayakumar L, Rajkumar S. Are risk factors for suicide universal? A case-control study in India. Acta Psychiatr Scand. 1999;99: 407-411. doi: http://dx.doi.org/10.1111/j.1600-0447.1999.tb00985.x
20. Bhatia MS, Aggarwal NK, Aggarwal BBL. Psychosocial profile of suicide ideators, attempters and completers in India.Int J Soc Psychiatry. 2000;46: 155-163. doi: http://dx.doi.org/10.1177/002076400004600301
21. Mayer P, Ziaian T. Are women in Indian society protected from suicide? Crisis. 2002;23: 98-103
22. Batra AK. Burn mortality: recent trends and sociocultural determinants in rural India. Burns. 2003;29: 270-275
23. Joseph A, Abraham S, Muliyil JP, George K, Prasad J, Minz S et al. Evaluation of suicide rates in rural India using verbal autopsies, 1994-9. BMJ. 2003;326: 1121-1122. doi: http://dx.doi.org/10.1136/bmj.326.7399.1121
24. Sharma BR, Sharma V, Harish D, Vij K. Suicides in northern India: causes, methods used and prevention. Medicine,Science and the Law. 2003;43: 221-229. doi: http://dx.doi.org/10.1258/rsmmsl.43.3.221
25. Steen DM, Mayer P. Patterns of suicide by age and gender in the Indian states: a reflection of human development?Arch Suicide Res. 2003;7: 247-264. doi: http://dx.doi.org/10.1080/13811110301556
26. Aaron R, Joseph A, Abraham S, Muliyil J, George K, Prasad J et al. Suicides in young people in rural southern India.Lancet. 2004;363: 1117-1118
27. Girdhar S, Leenaars AA, Dogra TD, Leenaars L, Kumar G. Suicide notes in India: what do they tell us? Arch Suicide Res. 2004;8: 179-185. doi: http://dx.doi.org/10.1080/13811110490271362
28. Gururaj G, Isaac MK, Subbakrishna DK, Ranjani R. Risk factors for completed suicides: a case-control study from Bangalore,India. Inj Control Saf Promot. 2004;11: 183-191
29. Kumar PNS. An analysis of suicide attempters versus completers in Kerala. Indian J Psychiatry. 2004;46: 144-149.30. Lalwani S, Sharma G, Kabra S, Girdhar S, Dogra T. Suicide among children and adolescents in south Delhi (1991–2000).Indian J Pediatr. 2004;71: 701-703. doi: http://dx.doi.org/10.1007/BF02730657
31. Sharma BR, Singh VP, Sharma R, Sumedha. Unnatural deaths In northern India: a profile. Journal of Indian Academy of Forensic Medicine. 2004;26: 140-146
32. Steen DM, Mayer P. Modernization and the male–female suicide ratio in India 1967–1997: Divergence or Convergence? Suicide Life-Threat Behav. 2004;34: 147-159.doi: http://dx.doi.org/10.1521/suli.34.2.147.32782
33. Abraham VJ, Abraham S, Jacob KS. Suicide in the elderly in Kaniyambadi block, Tamil Nadu, South India. Int J Geriatr Psychiatry. 2005;20: 953-955. doi: http://dx.doi.org/10.1002/gps.1385
34. Khan F, Anand B, Devi MG, Murthy KK. Psychological autopsy of suicide-a cross-sectional study. Indian J Psychiatry. 2005;47: 73-78. doi: http://dx.doi.org/10.4103/0019-5545.55935
35. Bose A, Konradsen F, John J, Suganthy P, Muliyil J, Abraham S.Mortality rate and years of life lost from unintentional injury and suicide in South India. Tropical Medicine & International Health. 2006;11: 1553-1556. doi: http://dx.doi.org/10.1111/j.1365-3156.2006.01707.x
36. Prasad J, Abraham VJ, Minz S, Abraham S, Joseph A,Muliyil JP et al. Rates and factors associated with suicide in Kaniyambadi Block, Tamil Nadu, South India, 2000-2002.Int J Soc Psychiatry. 2006;52: 65-71. doi: http://dx.doi.org/10.1177/0020764006061253
37. Mohanty S, Sahu G, Mohanty MK, Patnaik M. Suicide in India: a four year retrospective study. J Forensic Leg Med. 2007;14: 185-189. doi: http://dx.doi.org/10.1016/j.jcfm.2006.05.007
38. Chavan B, Singh G, Kaur J, Kochar R. Psychological autopsy of 101 suicide cases from northwest region of India.Indian J Psychiatry. 2008;50: 34-38. doi: http://dx.doi.org/10.4103/0019-5545.39757
39. Gupta B, Singh O. A unique trend of murder–suicide in the Jamnagar region of Gujarat, India (a retrospective study of 5 years). J Forensic Leg Med. 2008;15: 250-255. doi: http://dx.doi.org/10.1016/j.jflm.2007.12.013
40. Kanchan T, Menezes RG. Suicidal poisoning in southern India: gender differences. J Forensic Leg Med. 2008;15: 7-14.doi: http://dx.doi.org/10.1016/j.jflm.2007.05.006
41. Bastia BK, Kar N. A psychological autopsy study of suicidal hanging from Cuttack, India: focus on stressful life situations.Arch Suicide Res. 2009;13: 100-104. doi: http://dx.doi.org/10.1080/13811110802572221
42. Parkar SR, Dawani V, Weiss MG. Clinical diagnostic and sociocultural dimensions of deliberate self-harm in Mumbai,India. Suicide LifeThreat Behav. 2006;36: 223-228. doi:http://dx.doi.org/10.1521/suli.2006.36.2.223
43. Soman C, Vijayakumar K, Ajayan K, Safraj S, Kutty V.Suicide in South India: a community-based study in Kerala.Indian J Psychiatry. 2009;51: 261-264. doi: http://dx.doi.org/10.4103/0019-5545.58290
44. Manoranjitham SD, Rajkumar AP, Thangadurai P, Prasad J,Jayakaran R, Jacob KS. Risk factors for suicide in rural south India. Br J Psychiatry. 2010;196: 26-30. doi: http://dx.doi.org/10.1192/bjp.bp.108.063347
45. Hendin H, Vijayuakumar L, Bertolote JM, Wang H, Phillips MR, Pirkis J. Epidemiology of suicides in Asia. In: Hendin H, Phillips MR, Vijayakumar L, eds. Suicide and Suicide Prevention in Asia. Geneva: World Health Organization;2008: 7-18
46. National Crime Records Bureau. Accidental deaths and suicides in India. New Delhi: Government of India; 2012
47. Brent DA, Bridge J. Firearms availability and suicide:evidence, interventions, and future directions. Am Behav Sci.2003;46: 1192-1210
48. Shin SD, Suh GJ, Rhee JE, Sung J, Kim J. Epidemiologic characteristics of death by poisoning in 1991-2001 in Korea.J Korean Med Sci. 2004;19: 186-194. doi: http://dx.doi.org/10.3346/jkms.2004.19.2.186
49. Ung EK. Youth suicide and parasuicide in Singapore. Annals of the Academy of Medicine. 2003;32: 12-18
50. Yip PS. Suicides in Hong Kong, Taiwan and Beijing. Br J Psychiatry. 1996;169: 495-500
51. Laloë V. Patterns of deliberate self-burning in various parts of the world: A review. Burns. 2004;30(3): 207-215. doi: http://dx.doi.org/10.1016/j.burns.2003.10.018
52. Cantor CH. Suicide in the western world. In: Hawton K, van Heeringen K, eds. International Handbook of Suicide and Attempted Suicide. Chichester: John Wiley and Sons; 2000:9-28
53. Phillips MR, Li X, Zhang Y. Suicide rates in China, 1995–99.The Lancet. 2002;359: 835-840. doi: http://dx.doi.org/10.1016/S0140-6736(02)07954-0
54. Niaz U, Hassan S. Culture and mental health of women in South-East Asia. World Psychiatry. 2006;5: 118-120
55. Kumar V. Poisoning deaths in married women. J Clin Forensic Med. 2004;11: 2-5. http://dx.doi.org/10.1016/j.jcfm.2003.10.010
56. Kim M-D, Hong S-C, Lee S-Y, Kwak Y-S, Lee C-I,Hwang S-W et al. Suicide risk in relation to social class: a national registerbased study of adult suicides in Korea, 1999–2001. Int J Soc Psychiatry. 2006;52: 138-151
57. Zhang J, Conwell Y, Zhou L, Jiang C. Culture, risk factors and suicide in rural China: a psychological autopsy case control study. Acta Psychiatr Scand. 2004;110: 430-437. doi: http://dx.doi.org/10.1111/j.1600-0447.2004.00388.x
58. Collings S, Blakely T, Atkinson J, Fawcett J. Suicide Trends and Social Factors - New Zealand from 1981 to 1999: Analyzes from the New Zealand Census-Mortality Study. Wellington:University of Otago; 2005
59. Eddleston M, Phillips MR. Self poisoning with pesticides.BMJ. 2004;328: 42-44. doi: http://dx.doi.org/10.1136/bmj.328.7430.42
60. Rao AV. Suicide in the elderly: a report from India. Crisis.1991;12: 33-39
61. Cavanagh JTO, Carson AJ, Sharpe M, Lawrie SM.Psychological autopsy studies of suicide: a systematic review. Psychol Med. 2003;33: 395-405. doi: http://dx.doi.org/10.1017/S0033291702006943
62. Moscicki E. Epidemiology of suicide. In: Goldsmith S, ed.Risk Factors for Suicide. Washington, DC: National Academy Press; 2001: 1-4
63. Harris EC, Barraclough B. Excess mortality of mental disorder.Br J Psychiatry. 1998;173: 11-53
64. Hawton K, van Heeringen K. Suicide. Lancet. 2009;373:1372-1381
65. Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M,Beautrais A et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry.2008;192: 98-105. doi: http://dx.doi.org/10.1192/bjp.bp.107.040113
2014-1-20 accepted: 2014-4-01)

Anil Rane obtained his Bachelor’s degree from Goa Medical College, India in 1999 and his MD in Psychiatry from the Institute of Psychiatry & Human Behaviour in Bambolim in 2003. He has worked as a lecturer in Psychiatry in the same department since 2006. He is also the secretary of the Psychiatric Society of Goa. His main research interests are substance use disorders and the occurrence of non-communicable diseases in persons with severe mental illness.
有关印度自杀的系统综述
Anil RANE, Abhijit NADKARNI
自杀,印度,系统综述,有机磷农药,精神病
Background:Suicide is an important cause of death in India but estimated suicide rates based on data from India’s National Crime Records Bureau are unreliable.Aim:Systematically review existing literature on suicide and the factors associated with suicide in India.Methods:PubMed, PsycINFO, EMBASE, Global Health, Google Scholar and IndMED were searched using appropriate search terms. The abstracts of relevant papers were independently examined by both authors for possible inclusion. A standardized set of data items were abstracted from the full text of the selected papers.Results:Thirty-six papers met inclusion criteria for the analysis. The heterogeneity of sampling procedures and methods of the studies made meta-analysis of the results infeasible. Verbal autopsy studies in several rural locations in India report high suicide rates, from 82 to 95 per 100,000 population – up to 8-fold higher than the official national suicide rates. Suicide rates are highest in persons 20 to 29 years of age. Female suicide rates are higher than male rates in persons under 30 years of age but the opposite is true in those 30 years of age or older. Hanging and ingestion of organophosphate pesticides are the most common methods of suicide. Among women, self-immolation is also a relatively common method of suicide. Low socioeconomic status, mental illness (especially alcohol misuse) and inter-personal difficulties are the factors that are most closely associated with suicide.Conclusion:The quality of the information about suicide in India is quite limited, but it is clearly an important and growing public health problem. Compared to suicides in high-income countries, suicide in India is more prevalent in women (particularly young women), is much more likely to involve ingestion of pesticides, is more closely associated with poverty, and is less closely associated with mental illness.
http://dx.doi.org/10.3969/j.issn.1002-0829.2014.02.003
1Institute of Psychiatry & Human Behaviour, Goa, India
2London School of Hygiene & Tropical Medicine, London, United Kingdom
3Sangath, Goa, India
* correspondence: dranilrane@gmail.com
A full-text Chinese translation will be available at www.saponline.org on May 15, 2014.
背景:自杀是印度重要的死亡原因之一,但基于印度国家犯罪统计局数据估算的自杀率并不可靠。目标:系统回顾现有的有关印度自杀及自杀相关因素的文献。方法:选择适当的检索词在PubMed,PsycINFO,EMBASE,全球健康,谷歌学术和IndMED数据库中查找文献。查找到的论文摘要由两位作者分别独立筛选是否符合纳入标准,再从筛选出的论文全文中摘录标准化数据。结果:本研究筛选出符合纳入标准的36篇论文进行分析。由于抽样过程和研究方法的异质性,荟萃分析的方法不可行。在印度部分农村地区的死因推断研究中报道的自杀率较高,每10万人口中有82至95人自杀,比官方报道的全国自杀率高出8倍。其中20至29岁人群的自杀率最高;30岁以下人群中女性自杀率高于男性,而30岁及以上的人群则正好相反。自缢和服用有机磷农药是最常见的自杀方式,自焚在女性较为常见。社会经济地位低、精神疾病(尤其是酒精滥用)和人际交往障碍是与自杀关系最为密切的因素。结论:有关印度自杀的数据质量非常有限。但显而易见,自杀是一个重要且日益严重的公共卫生问题。相对于高收入国家而言,印度自杀特点为:女性(尤其是年轻妇女)自杀率高于男性、较多选择服用农药的自杀方式、与贫穷因素关系更为紧密而与精神疾病因素相关性较低。
猜你喜欢
健康体检与管理(2022年4期)2022-05-13
当代陕西(2020年17期)2020-10-28
石油沥青(2018年6期)2018-12-29
NBA特刊(2018年21期)2018-11-24
小学科学(学生版)(2018年9期)2018-09-21
资源节约与环保(2018年1期)2018-02-08
中国塑料(2016年2期)2016-06-15
功能高分子学报(2016年1期)2016-04-26
中国卫生标准管理(2015年17期)2016-01-20
四川党的建设(2014年9期)2014-08-23
- 上海精神医学的其它文章
- The dopamine system and alcohol dependence
- Effectiveness of self-management training in community residents with chronic schizophrenia: a single-blind randomized controlled trial in Shanghai, China
- Randomized controlled trial comparing changes in serum prolactin and weight among female patients with first-episode schizophrenia over 12 months of treatment with risperidone or quetiapine
- Retrospective comparison of cognitive behavioral therapy and symptom-specific medication to treat anxiety and depression in throat cancer patients after laryngectomy
- Providing free treatment for severe mental disorders in China
- Case report on lithium intoxication with normal lithium blood levels