
利拉鲁肽与艾塞那肽治疗2型糖尿病降低体质量指标的meta分析
2015-02-07 11:24张楚辞赵玉岩温晶
中国医科大学学报 2015年7期
张楚辞,赵玉岩,温晶
(中国医科大学附属第一医院内分泌科,沈阳 110001)
·论著·
利拉鲁肽与艾塞那肽治疗2型糖尿病降低体质量指标的meta分析
张楚辞,赵玉岩,温晶
(中国医科大学附属第一医院内分泌科,沈阳 110001)
目的系统评价类胰高血糖素样肽1类似物利拉鲁肽与艾塞那肽治疗2型糖尿病降低体质量指标情况。方法计算机检索Cochrane图书馆、PubMed、EMBASE、CNKI、CBM、中国生物医学文献数据库、中国期刊全文数据库,对纳入的随机对照试验(RCT)进行质量评价,并用Stata11.0软件对提取的相关数据进行meta分析。结果共纳入31个RCT,共计7 036例患者,对其体质量降低情况进行了meta分析。结果发现,利拉鲁肽与对照组相比,当注射剂量为1.8 mg时,能有效降低体质量(WMD=-0.45,95%CI:-0.59,-0.31);与阳性对照相比,当注射剂量为1.2 mg和1.8 mg时,均能有效降低体质量(WMD=-0.91,95%CI:-1.07,-0.75;WMD=-0.78,95%CI:-1.02,-0.54)。艾塞那肽与对照组相比,当注射剂量为5 μg和10 μg时,均能有效降低体质量(WMD=-0.36,95%CI:-0.64,-0.09;WMD=-0.99,95%CI:-1.27,-0.72);与阳性对照相比,当注射剂量为10 μg时,能有效降低体质量(WMD=-1.14,95%CI:-1.46,-0.82)。结论利拉鲁肽和艾塞那肽作为新的肠促胰岛激素类似物,均能够减轻体质量,为2型糖尿病患者提供了新的降糖药选择。
糖尿病;类胰高血糖素样肽1;艾塞那肽;利拉鲁肽;meta分析
类胰高血糖素样肽1(glucagon like peptide-1,GLP-1)是一种肠促胰岛素,由末段空肠、回肠、结肠的L细胞产生。体内葡萄糖水平的高低对胰岛素分泌和胰高血糖素的产生均起决定性的作用,同时也可以通过抑制胃排空和增加饱腹感来减少食物的摄入,并对β细胞新生的增加和β细胞的凋亡均有影响。近年来,肠促胰岛素与2型糖尿病(type 2 diabe-tes mellitus,T2DM)病理生理机制间的重要作用已被广泛认识。研究显示,肠促胰岛素通路在T2DM患者中减弱,故可以此通路为靶点开发新的降糖药物[1]。因天然GLP-1易被二肽基肽酶(second dipeptidyl peptidase,DPP)Ⅳ降解并被肾清除,且半衰期很短(<2 min),需要持续皮下注射才能发挥药理效应[2],因此,GLP-1的开发价值受到明显的限制。与DPP-Ⅳ抑制剂相比,GLP-1受体激动剂或类似物能够更好地通过促进胰岛素的分泌来控制血糖,降低体质量;而DPP-Ⅳ抑制剂的有益作用有赖于机体内源性GLP-1的水平,因而它的药理作用较GLP-1类似物的作用弱[3]。综上所述,GLP-1类似物理论上可能是治疗糖尿病的首选药物。
首个获得食品药品监督管理局(FDA)批准的GLP-1类似物药物为艾塞那肽。它具有多种生理活性,如刺激胰岛B细胞的增殖与分化、降低胃排空速率、促进饱食感等;利拉鲁肽是长效GLP-1类似物,已开始应用于临床。目前尚无利拉鲁肽和艾塞那肽治疗T2DM降低体质量方面的系统评价,而现有的国内外随机对照试验(randomized controlled trial,RCT)研究对于利拉鲁肽和艾塞那肽在治疗T2DM降低体质量方面是否存在差异结果不一。故本研究拟采用meta分析方法,评价利拉鲁肽和艾塞那肽在治疗T2DM降低体质量方面的疗效,旨在为T2DM患者提供降糖药选择的参考。
1 材料与方法
1.1 检索策略
以中文关键词“利拉鲁肽”、“艾塞那肽”、“随机对照试验”、“2型糖尿病”,英文关键词“Liraglutide”、“Exenatide”、“Random control trial”、“Type 2 Diabetes”检索1987-2014年PubMed、Cochrane Database of Systematic Review、Embase、知网(CNKI)、万方数据库;与作者和生产厂家联系,收集未发表的文献(灰色文献)。文献检索包括4个步骤:(1)检索各数据库中相关的系统评价和meta分析;(2)在各中英文数据库中检索相关的演示论文,并对所获文献文题、摘要、所用的关键词以及主题词进行分析,以进一步确定文献检索的关键词;(3)运用所有相关的主题词和关键词进行数据检索,如果摘要初步符合纳入标准,则进一步查找并阅读全文;(4)发表语种不限;(5)通过所获文献后附参考文献进行进一步检索。
1.2 纳入标准
(1)利拉鲁肽和艾塞那肽治疗T2DM的RCT;(2)对样本大小有明确规定;(3)资料有原始数据、均数及标准差或者可以转化为均数及标准差;(4)汇总的结果可以用相应的统计指标表达;(5)年龄18~80岁,以1999年WHO标准确诊为T2DM患者,非妊娠,无心、肝、肾功能异常;(6)不包括职业人群的研究资料;(7)由2名评价员采用统一的纳入标准同时对所选文献进行纳入,如遇分歧通过讨论由第3位研究者协助解决;(8)干预措施:试验组采用利拉鲁肽,对照组使用安慰剂,阳性对照组采用口服降糖药物(oral hypoglycemic drugs,OAD),其他治疗措施完全相同。
1.3 排除标准
(1)排除质量差、重复报告、报告信息太少以及数据描述不详的文献;(2)排除未进行比较、未报道具体临床结果的文献。
1.4 数据处理
按meta分析的要求整理数据,建立数据库并核对数据。对入选文献进行异质性检验。若同质则采用固定效应模型进行合并分析;否则采用随机效应模型(D-L法)进行合并分析,然后计算出其加权均数差(weighted mean difference,WMD)及其95% CI,做出森林图。最后进行敏感性分析,做倒漏斗图评估发表偏倚。由2名评价员采用统一的数据提取表格,同时独立提取资料数据,如遇分歧通过讨论由第3位研究者协助解决。以上所有过程均采用Stata 11.0软件进行处理。
2 结果
2.1 文献检索结果
本研究初检出相关文献384篇,其中,英文文献103篇,中文文献281篇。根据以上文献资料的纳入及排除标准,经筛选并纳入本次meta分析的文献共31篇[4~34],其中,英文文献25篇,中文文献6篇。
2.2 纳入研究一般特征
上述文献均为随机对照研究,且民族与职业不限;对照组与病例组在同一地区。文献的筛选纳入参照AMSTAR质量评价标准,对每篇病例对照研究进行质量评分。
2.3 meta分析结果
2.3.1 利拉鲁肽vs安慰剂:共纳入5个RCT[14,24,25,27,30]比较了1.8 mg利拉鲁肽与安慰剂治疗T2DM。采用随机效应模型,meta分析结果显示:利拉鲁肽治疗T2DM在降低体质量方面优于安慰剂,差异有统计学意义(WMD=-0.45,95%CI:0.59~-0.31)。
2.3.2 利拉鲁肽vs OAD
2.3.2.1 1.2 mg利拉鲁肽共纳入3个RCT[5,22,28]比较了利拉鲁肽与OAD治疗T2DM。采用随机效应模型,meta分析结果显示:利拉鲁肽治疗T2DM在降低体质量方面优于OAD,差异有统计学意义(WMD=-0.91,95%CI:-1.07~-0.75)。
2.3.2.2 1.8 mg利拉鲁肽共纳入4个RCT[4,22,27,28]比较了利拉鲁肽与OAD治疗T2DM。采用随机效应模型,meta分析结果显示:利拉鲁肽治疗T2DM在降低体质量方面优于OAD,差异有统计学意义(WMD=-0.78,95%CI:-1.02~-0.54)。
2.3.3 艾塞那肽vs安慰剂
2.3.3.1 5 μg艾塞那肽共纳入4个RCT[12,20,21,23]比较了艾塞那肽与安慰剂治疗T2DM。采用随机效应模型,meta分析结果显示:艾塞那肽治疗T2DM在降低体质量方面优于安慰剂,差异有统计学意义(WMD=-0.36,95%CI:-0.64~-0.09)。
2.3.3.2 10 μg艾塞那肽共纳入20个RCT比较了艾塞那肽与安慰剂治疗T2DM[6,7,9~14,16,17,19~24,29,31~33]。采用随机效应模型,meta分析结果显示:艾塞那肽治疗T2DM在降低体质量方面优于安慰剂,差异有统计学意义(WMD=-0.99,95%CI:-1.27~-0.72)。
2.3.4 艾塞那肽vs OAD:10 μg艾塞那肽共纳入6个 RCT[8,10,14,15,17,18]比较了艾塞那肽与 OAD治疗T2DM。采用随机效应模型,meta分析结果显示:艾塞那肽治疗T2DM在降低体质量方面优于OAD,差异有统计学意义(WMD=-1.14,95%CI:-1.46~-0.82)。
2.4 敏感性分析
对研究资料采用固定效应模型和随机效应模型分别计算,结果的一致程度可在一定水平上反映其合并结果的可靠性。本研究采用2种模型估计合并,2种模型所得结果WMD值以及95%CI结果非常接近,说明本研究的合并结果基本可靠,见表1。
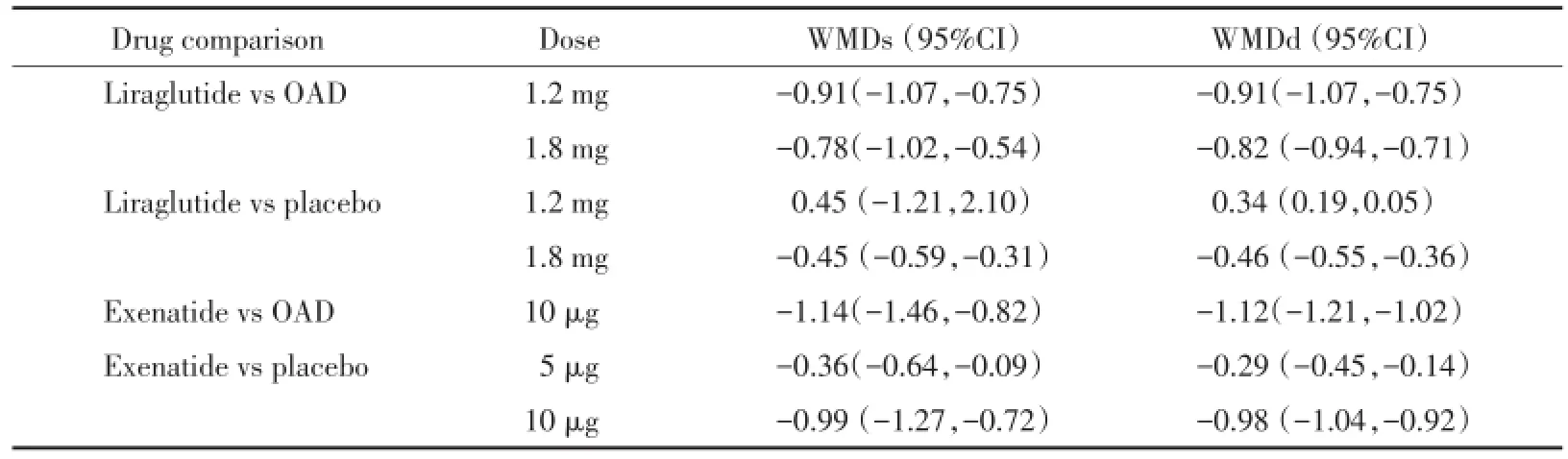
表1 随机效应模型和固定效应模型计算结果比较Tab.1 Results of comparison between random effect model and fixed effect model
3 讨论
利拉鲁肽和艾塞那肽均为GLP-1受体激动剂,2药虽为同类药物,但在来源、分子结构、药代动力学方面却存在差异,国内外对其降糖、减重等效应也有广泛研究。本研究通过meta分析的方法量化了利拉鲁肽和艾塞那肽对T2DM患者体质量的影响,并通过亚组分析的方法研究了2种药物在使用不同剂量时对患者体质量的影响。结果显示:与服用安慰剂的患者相比,仅当患者使用利拉鲁肽1.2 mg时,不降低患者体质量,差异无统计学意义,其余各剂量组利拉鲁肽均可显著降低患者体质量;除使用5 μg艾塞那肽治疗与OAD比较没有充分研究外,其余研究通过meta分析证实艾塞那肽比较其他治疗均可显著降低患者体质量。
本研究中共纳入8个研究(n=3 351),全部为RCT。从文献质量评价的结果来看,质量等级多为moderated,大多数文献均报告了如何产生随机分配序列、随机方案如何隐藏、盲法如何实施,提示纳入研究存在选择性偏倚的可能,但有些研究方法存在一定局限性。由于阴性结果文章往往无法发表,可能存在一定发表偏倚。由于几乎所有试验的疗程都少于30周,因而对利拉鲁肽长期有效性和安全性的评价受到限制。从研究人群来看,7个研究主要为欧美白种人,1个研究主要为欧洲和亚洲人,6个研究主要为亚洲人,人种差异可能对研究结果产生一定的影响。
利拉鲁肽和艾塞那肽均采用皮下注射,部分患者不愿意接受,故在随机选择研究对象时可能存在选择性偏倚。研究将<18岁的青少年和>80岁的老年人、妊娠或哺乳妇女排除在外,故结论可能不能应用于以上人群。因纳入研究主要由制药企业提供赞助,潜在的经济利益可能对试验结果产生一定的影响。
本研究纳入的文献均为多中心研究,文献质量高,虽然没有实施盲法,但结局指标均为客观指标,故盲法的实施与否对研究结果的影响较小。综上所述,利拉鲁肽和艾塞那肽作为新的肠促胰岛激素类似物,较对照组能显著减轻体质量,为T2DM患者提供了新的降糖药选择。因纳入研究的样本量较小,随访时间较短,尚需要开展大样本、高质量的研究,进一步论证其疗效和安全性。
参考文献:
[1]Drucker DJ,Nauck MA.The incretin system:glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes[J].Lancet,2006,368(9548):1696-1705.
[2]Green BD,Gault VA,Mooney MH,et al.Novel dipeptidyl peptidase IV resistant analogues of glucagon-like peptide-1(7-36)amide have preserved biological activities in vitro conferring improved glucoselowering action in vivo[J].J Mol Endocrinol,2003,31(3):529-540.
[3]Kalra S.Emerging role of dipeptidyl peptidase-IV(DPP-4)inhibitor vildagliptin in the management of type 2 diabetes[J].J Assoc Physicians India,2011,59(2):237-245.
[4]王锋,陈刚,李雪侠.利那鲁肽治疗2型糖尿病疗效观察[J].山东医药,2014,54(4):44-46.
[5]陆静尔.利拉鲁肽治疗新诊断2型糖尿病患者临床疗效的观察[J].中国糖尿病杂志,2014,22(4):350-352.
[6]蒋建家,牟伦盼,苏劲波,等.艾塞那肽对口服降糖药治疗欠佳的肥胖2型糖尿病患者的疗效及安全性[J].中华糖尿病杂志,2011,3(4):305-308.
[7]杜予俊.艾塞那肽与甘精胰岛素治疗血糖控制不佳的2型糖尿病的临床对照研究[J].实用药物与临床,2014,17(5):579-580.
[8]陈晓媛,孟姝含,霍珊,等.艾塞那肽治疗新发2型糖尿病的临床疗效观察[J].国际老年医学杂志,2012,33(5):193-196.
[9]Apovian CM,Bergenstal RM,Cuddihy RM,et al.Effects of exenatide combined with lifestyle modification in patients with type 2 diabetes[J].Am J Med,2010,123(5):468.
[10]Barnett AH,Burger J,Johns D,et al.Tolerability and efficacy of exenatide and titrated insulin glargine in adult patients with type 2 diabetes previously uncontrolled with metformin or a sulfonylurea:a multinational,randomized,open-label,two-period,crossover noninferiority trial[J].Clin Ther,2007,29(11):2333-2348.
[11]Bergenstal R,Lewin A,Bailey T,et al.Efficacy and safety of biphasic insulin aspart 70/30 versus exenatide in subjects with type 2 diabetes failing to achieve glycemic control with metformin and a sulfonylurea[J].Curr Med Res Opin,2009,25(1):65-75.
[12]Buse JB,Henry RR,Han J,et al.Effects of exenatide(exendin-4)on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes[J].Diabetes Care,2004,27(11):2628-2635.
[13]Buse JB,Bergenstal RM,Glass LC,et al.Use of twice-daily exenatide in basal insulin-treated patients with type 2 diabetes:a randomized,controlled trial[J].Ann Intern Med,2011,15(42):103-112.
[14]Davies MJ,Donnelly R,Barnett AH,et al.Exenatide compared with long-acting insulin to achieve glycaemic control with minimal weight gain in patients with type 2 diabetes:results of the helping evaluate exenatide in patients with diabetes compared with longacting insulin(HEELA)study[J].Diabetes Obes Metab,2009,11(12):1153-1162.
[15]DeFronzo RA,Triplitt C,Qu Y,et al.Effects of exenatide plus rosiglitazone on beta-cell function and insulin sensitivity in subjects with type 2 diabetes on metformin[J].Diabetes Care,2010,33(5):951-957.
[16]Diamant M,Van Gaal L,Stranks S,et al.Once weekly exenatide compared with insulin glargine titrated to target in patients with type 2 diabetes(DURATION-3):an open-label randomised trial[J].Lancet,2010,375(9733):2234-2243.
[17]Gallwitz B,Bohmer M,Segiet T,et al.Exenatide twice daily versus premixed insulin aspart 70/30 in metformin-treated patients with type 2 diabetes:a randomized 26-week study on glycemic control and hypoglycemia[J].Diabetes Care,2011,34(3):604-606.
[18]Gallwitz B,Guzman J,Dotta F,et al.Exenatide twice daily versus glimepiride for prevention of glycaemic deterioration in patients with type 2 diabetes with metformin failure(EUREXA):an openlabel,randomised controlled trial[J].Lancet,2012,379(9833):2270-2278.
[19]Heine RJ,Van Gaal LF,Johns D,et al.Exenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes:a randomized trial[J].Ann Intern Med,2005,14(38):559-569.
[20]Kadowaki T,Namba M,Yamamura A,et al.Exenatide exhibits dose -dependent effects on glycemic control over 12 weeks in Japanese patients with suboptimally controlled type 2 diabetes[J].Endocr J,2009,56(3):415-424.
[21]Kendall DM,Riddle MC,Rosenstock J,et al.Effects of exenatide(exendin-4)on glycemic control over 30 weeks in patients with type 2 diabetes treated with metformin and a sulfonylurea[J].Diabetes Care,2005,28(5):1083-1091.
[22]Liutkus J,Rosas Guzman J,Norwood P,et al.A placebo-controlled trial of exenatide twice-daily added to thiazolidinediones alone or in combination with metformin[J].Diabetes Obes Metab,2010,12(12):1058-1065.
[23]Moretto TJ,Milton DR,Ridge TD,et al.Efficacy and tolerability of exenatide monotherapy over 24 weeks in antidiabetic drug-naive patients with type 2 diabetes:a randomized,double-blind,placebocontrolled,parallel-group study[J].Clin Ther,2008,30(8):1448-1460.
[24]Nauck MA,Duran S,Kim D,et al.A comparison of twice-daily exenatide and biphasic insulin aspart in patients with type 2 diabetes who were suboptimally controlled with sulfonylurea and metformin:a non-inferiority study[J].Diabetologia,2007,50(2):259-267.
[25]Nauck M,Frid A,Hermansen K,et al.Efficacy and safety comparison of liraglutide,glimepiride,and placebo,all in combination with metformin,in type 2 diabetes:the LEAD(liraglutide effect and action in diabetes)-2 study[J].Diabetes Care,2009,32(1):84-90.
[26]Lee WC,Dekoven M,Bouchard J,et al.Improved real-world glycaemic outcomes with liraglutide versus other incretin-based therapies in type 2 diabetes[J].Diabetes Obes Metab,2014,16(9):819-826.
[27]Russell-Jones D,Vaag A,Schmitz O,et al.Liraglutide vs insulin glargine and placebo in combination with metformin and sulfonylurea therapy in type 2 diabetes mellitus(LEAD-5 met+SU):a randomised controlled trial[J].Diabetologia,2009,52(10):2046-2055.
[28]Yang W,Chen L,Ji Q,et al.Liraglutide provides similar glycaemic control as glimepiride(both in combination with metformin)and reduces body weight and systolic blood pressure in Asian population with type 2 diabetes from China,South Korea and India:a 16-week,randomized,double-blind,active control trial(*)[J].Diabetes Obes Metab,2011,13(1):81-88.
[29]Zinman B,Hoogwerf BJ,Duran Garcia S,et al.The effect of adding exenatide to a thiazolidinedione in suboptimally controlled type 2 diabetes:a randomized trial[J].Ann Intern Med,2007,14(67):477-485.
[30]Zinman B,Gerich J,Buse JB,et al.Efficacy and safety of the human glucagon-like peptide-1 analog liraglutide in combination with metformin and thiazolidinedione in patients with type 2 diabetes(LEAD-4 Met+TZD)[J].Diabetes Care,2009,32(7):1224-1230.
[31]Inagaki N,Atsumi Y,Oura T,et al.Efficacy and safety profile of exenatide once weekly compared with insulin once daily in Japanese patients with type 2 diabetes treated with oral antidiabetes drug(s):results from a 26-week,randomized,open-label,parallelgroup,multicenter,noninferiority study[J].Clin Ther,2012,34(9):1892-1908.
[32]Davies M,Heller S,Sreenan S,et al.Once-weekly exenatide versus once-or twice-daily insulin detemir:randomized,open-label,clinical trial of efficacy and safety in patients with type 2 diabetes treated with metformin alone or in combination with sulfonylureas[J]. Diabetes Care,2013,36(5):1368-1376.
[33]Bunck MC,Diamant M,Corner A,et al.One-year treatment with exenatide improves beta-cell function,compared with insulin glargine,in metformin-treated type 2 diabetic patients:a randomized,controlled trial[J].Diabetes Care,2009,32(5):762-768.
[34]Nauck M,Frid A,Hermansen K,et al.Long-term efficacy and safety comparison of liraglutide,glimepiride and placebo,all in combination with metformin in type 2 diabetes:2-year results from the LEAD-2 study[J].Diabetes Obes Metab,2013,15(3):204-212.
[35]Shea BJ,Grimshaw JM,Wells GA,et al.Development of AMSTAR:a measurement tool to assess the methodological quality of systematic reviews[J].BMC Med Res Methodol,2007,7:10.
(编辑 王又冬)
EffectsofExenatide and Liraglutide on Body Weight:AMeta-analysis
ZHANGChu-ci,ZHAOYu-yan,WENJing
(DepartmentofEndocrinology,The FirstHospital,China MedicalUniversity,Shenyang 110001,China)
ObjectiveTo systematically evaluate the effects of glucagon-like peptide-1(GLP-1)analogues exenatide and liraglutide on body weight in patients with type 2 diabetics mellitus.MethodsSuch databases as PubMed,Embase,CNKI and CMFD(1987-2014)were searched for randomized controlled trials.The meta-analysis was performed on the extracted related data using the software STATA 11.ResultsTotally 31 RCTs(7 036 patients)were included.The meta-analysis on body weight in these patients showed the following findings:compared to controls,liraglutide(1.8 mg)effectively decreased body weight(WMD=-0.45,95%CI:-0.59,-0.31);compared to positive controls,liraglutide(1.2 mg and 1.8 mg)also effectively decreased body weight(WMD=-0.91.95%CI:-1.07,-0.75;WMD=-0.78,95%CI:-1.02,-0.54).Compared to controls,exenatide(5 μg and 10 μg)effectively decreased body weight(WMD=-0.36,95%CI:-0.64,-0.09;WMD=-0.99,95%CI:-1.27,-0.72);compared to positive controls,exenatide(10μg)also effectively decreased body weight(WMD=-1.14,95%CI:-1.46,-0.82).ConclusionAs novelintestinal pancreatotropic hormone analogues,exenatide and liraglutide can effectively reduce body weight,providing new alternatives of hypoglycemic agentsforpatients with type 2 diabeticsmellitus.
diabetes;glucagon-like peptide-1;exenatide;liraglutide;meta-analysis
R587.1
A
0258-4646(2015)07-0591-05
国家自然科学基金(81071460,81470998)
张楚辞(1985-),女,医师,硕士.
赵玉岩,E-mail:g572@sina.com
2014-10-27
网络出版时间:
猜你喜欢
西南医科大学学报(2022年2期)2022-11-23
中国药学药品知识仓库(2022年1期)2022-03-23
实用中西医结合临床(2020年5期)2020-12-23
中国骨质疏松杂志(2020年6期)2020-10-27
科技风(2019年21期)2019-09-04
特别健康·下半月(2019年6期)2019-08-01
祝您健康(2019年3期)2019-03-22
时代英语·高一(2018年5期)2018-11-19
时代英语·高一(2017年5期)2017-11-14
中华胰腺病杂志(2013年6期)2013-10-19
