
促性腺激素释放激素拮抗剂和激动剂对不孕患者体外受精
——胚胎移植的疗效
2015-07-07 15:22厉丹丹舒静
中国生化药物杂志 2015年2期
厉丹丹,舒静
(1.浙江省嵊州市人民医院 妇产科,浙江 嵊州 312400;2.浙江大学医学院邵逸夫医院 妇产科,浙江 杭州 310016)
促性腺激素释放激素拮抗剂和激动剂对不孕患者体外受精
——胚胎移植的疗效
厉丹丹1,舒静2
(1.浙江省嵊州市人民医院 妇产科,浙江 嵊州 312400;2.浙江大学医学院邵逸夫医院 妇产科,浙江 杭州 310016)
目的 探讨促性腺激素释放激素拮抗剂(gonadotropin releasing hormone antagonist,GnRH-ant)方案和GnRH激动剂(gonadotropin releasing hormone agonist,GnRH-a)方案对不孕患者体外受精—胚胎移植(in vitro fertilizati on and embryo transfer, IVF-ET)的不同疗效。方法 选取2013年1月~12月于浙江省嵊州市人民医院进行初次控制性促排卵及IVF-EF助孕的不孕症患者400例,其中200例采用GnRH-ant方案(低龄组和高龄组),200例采用GnRH-a(低龄组和高龄组)。通过检测患者的一般情况、治疗及妊娠结果及其临床意义,确定GnRH拮抗剂方案和GnRH激动剂方案的可行性。结果 GnRH-ant低龄组(A组)和GnRH-ant高龄组(B组)在Gn使用时间、Gn用量、促排时间、取卵数及成熟卵数上,分别低于GnRH-a低龄组和GnRH-a高龄组。其中Gn使用时间、Gn用量和促排时间上差异具有统计学意义(P<0.05),取卵数和成熟卵数无统计学意义。 IVF-ET治疗妊娠结果显示GnRH-ant低龄组和GnRH-ant高龄组在胚胎种植率、临床妊娠率和流产率上,均分别低于GnRH-a低龄组和GnRH-a高龄组,而持续妊娠率高于GnRH-a低龄组和GnRH-a高龄组,差异均无统计学意义。结论 对于控制性促排卵及IVF-EF助孕的不孕症患者,GnRH拮抗剂方案和GnRH激动剂方案临床妊娠结果均良好,无明显差异。
促性腺激素释放激素;临床方案;体外受精;胚胎移植;妊娠率
随着试管婴儿技术的发展和1978年第1例试管婴儿的诞生,体外受精—胚胎移植(in vitro fertilizati on and embryo transfer,IVF-ET)技术受到了更加广泛的关注[1-3]。促性腺激素释放激素(gonadotro in releasing hormone,GnRH)对IVF-ET的治疗效果能起到良好的改善作用,其中促性腺激素释放激素激动剂(gonadotropin releasing hormone agonist,GnRH-a)和促性腺激素释放激素拮抗剂(gonadotropin releasing hormone antagonist,GnRH-ant)在临床中应用最为广泛[4]。GnRH-a的作用机理是模拟天然促性腺激素释放激素的效应,抑制促性腺激素释放激素的受体,调节相关激素分泌水平[5-7]。但是GnRH-a也存在一些弊端,如增加促排时间,提高骤发作用及囊肿形成的概率等[8]。GnRH-ant在1991年开始应用于临床,它可以在一定程度上避免GnRH-a的副作用,在治疗周期、用药频率和用量上有一定优势。目前,GnRH-ant和GnRH-a已成为IVF-ET研究的热点[9-12]。本实验通过检测GnRH-ant高龄组、低龄组及GnRH-a高龄组、低龄组4组不孕患者的一般情况、治疗及妊娠结果及其临床意义,对拮抗剂方案和激动剂方案进行初步研究,探究GnRH拮抗剂方案和GnRH激动剂方案的可行性和使用价值。探究对不孕患者最为有效、安全和经济的方案,以期为临床工作作出可行性指导。
1 资料与方法
1.1 一般资料 选取2013年1月~2013年12月在浙江省嵊州市人民医院妇产科行IVF-ET助孕的不孕症患者400例,其中年龄大于30岁和小于30岁患者各200例。分为GnRH-ant低龄组(A组)和GnRH-ant高龄组(B组),每组各100例。GnRH-a低龄组(C组)和GnRH-a高龄组(D组),每组各100例。比较上述4组患者的一般情况和治疗结果。排除标准:子宫因素不孕;结核病史;输卵管积水;子宫内膜息肉;卵巢高反应。纳入标准:基础卵泡刺激素<12 U/L;取卵数>5个;初次接受IVF-ET助孕;卵巢储备功能正常。本实验获得患者知情同意,且全程有本院伦理委员会监督。
1.2 方法
1.2.1 促性腺激素释放激素拮抗剂方案:GnRH-ant方案的步骤和方法见表1。
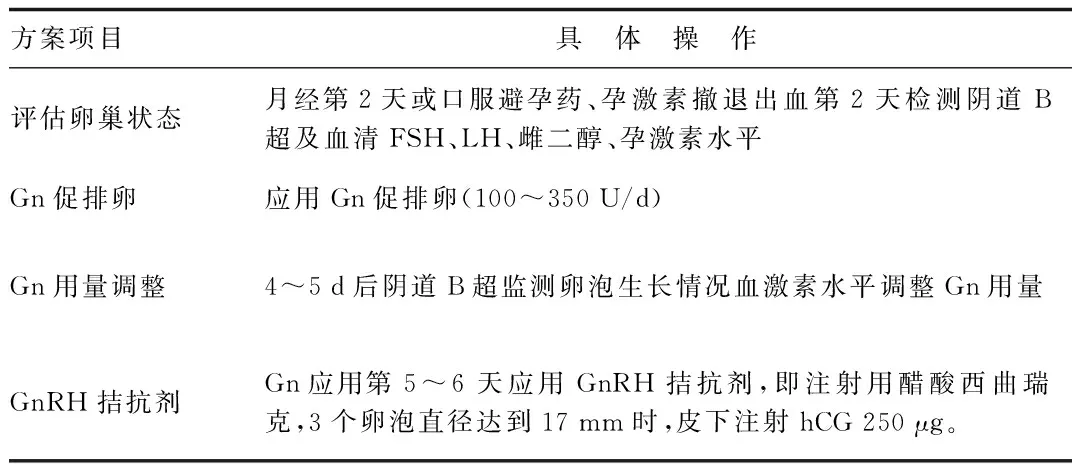
表1 GnRH-ant方案的操作步骤Tab.1 The operation steps of GnRH-ant plan
1.2.2 促性腺激素释放激素激动剂方案:GnRH-a方案的步骤和方法见表2。
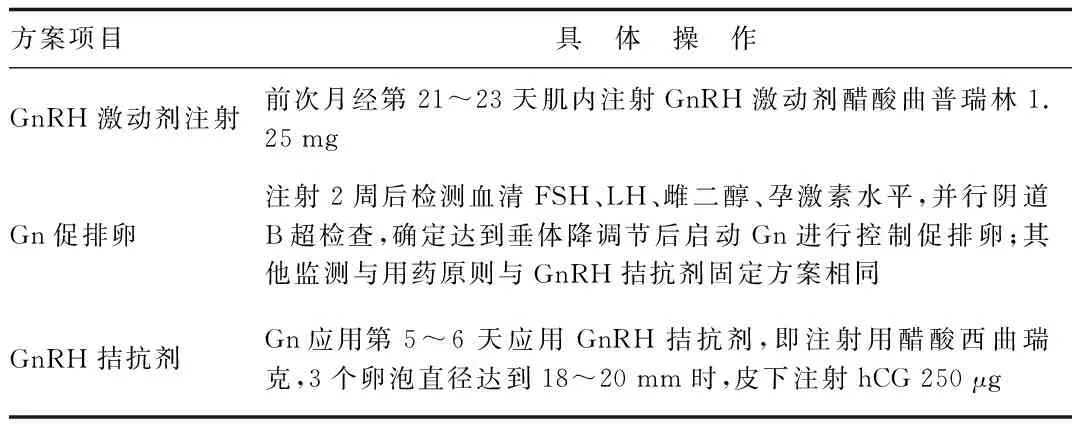
表2 GnRH-a方案的操作步骤Tab.2 The operation steps of GnRH-a plan
1.3 取卵、黄体支持 在hCG注射36 h后B超引导取卵。4 h后进行常规IVF或ICS受精。3 d后进行胚胎移植,并给予黄体支持。肌肉注射黄体酮60 mg/d。取卵后5 d进行胚胎移植。
1.4 结果检测 妊娠情况判断:在胚胎移植14 d后,检测血清hCG水平。28 d后进行B超检查,见宫内胎囊和心管搏动即为临床妊娠。

2 结果
2.1 2组患者一般情况比较 GnRH-ant低龄组(A组)、GnRH-ant高龄组(B组)、GnRH-a低龄组(C组)和GnRH-a高龄组(D组)4组不孕患者在平均年龄、不孕时长、不孕类别、体质量指数(BMI)及基础FSH水平相比较,差异均无统计学意义。结果见表3。

表3 各组患者一般情况比较±s)Tab.3 Comparison of patient’s normal ±s)
2.2 患者治疗情况比较 GnRH-ant低龄组(A组)和GnRH-ant高龄组(B组)在Gn使用时间、Gn用量、促排时间、取卵数及成熟卵数上,分别低于GnRH-a低龄组和GnRH-a高龄组。其中Gn使用时间、Gn用量和促排时间上差异具有统计学意义(P<0.05),取卵数和成熟卵数无明显统计学意义,见表4。
表4 患者治疗情况比较±s)Tab.4 Comparison of patient’s treatment ±s)
*P<0.05,A组与C组相比较,group A compared with group C;#P<0.05,B组与D组相比较, group B compared with group D
2.3 IVF-ET治疗妊娠结果比较 IVF-ET治疗妊娠结果如表5所示。GnRH-ant低龄组和GnRH-ant高龄组在胚胎种植率、临床妊娠率和流产率上,均分别低于GnRH-a低龄组和GnRH-a高龄组,而持续妊娠率高于GnRH-a低龄组和GnRH-a高龄组,差异均无统计学意义。
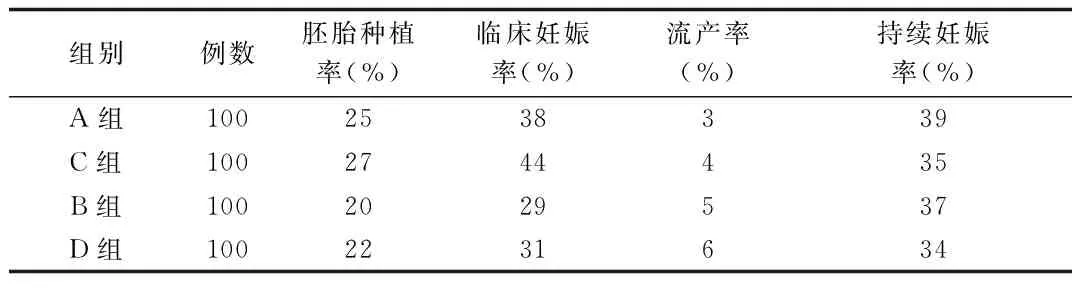
表5 患者治疗情况比较Tab.5 Comparison of patient’s treatment
3 讨论
GnRH-ant和GnRH-a方案是目前使用最多的2种控制排卵方案。GnRH-ant可以有效减少卵巢过度刺激综合征(ovarian hyper-stimulation syndrome, OHSS)的发生,但GnRH-ant的取卵率及妊娠率均较低,限制了GnRH-ant在临床上的广泛应用[13-15]。随着临床经验的积累,GnRH-ant方案的临床妊娠率逐渐提高。目前广泛应用的主要有2种GnRH-ant方案,分别为固定方案和灵活方案[16]。GnRH-a方案可改善卵子的质量,提高妊娠率,但也存在骤发作用、促排卵时间长及用药量大等问题。如何更有效地使用GnRH-ant和GnRH-a方案已成为生殖医学研究的重点。
3.1 GnRH-ant和GnRH-a方案妊娠结果比较 本研究中GnRH-ant组的取卵数和成熟卵数低于GnRH-a组,但各组的胚胎种植率和临床妊娠率无明显的统计学差异,说明GnRH-ant组和GnRH-a组方案效果相当。2010年肖劲松等[3]发现,GnRH-a方案与GnRH-ant方案在临床妊娠率上无显著差异。可能与GnRH-ant进入临床后用药方案不统一和使用GnRH-ant的经验不足有关,也可能与GnRH-ant对卵子、胚胎质量和子宫内膜容受性的影响有关。
3.2 GnRH-ant和GnRH-a方案Gn用药量、促排时间比较 本研究发现,与GnRH-a组方案相比较,GnRH-ant组Gn用药量、促排时间及用药时间均显著减少。这提示,GnRH-ant组整体治疗时间更短、Gn用药量更少。这与Simon C等[17]的报道一致,因垂体局部受体脱敏与消耗达到降调节作用,GnRH-a用药后需1周才能达到垂体抑制状态。因此,GnRH-a方案的Gn用量和促排时间明显延长。而GnRH-ant可与GnRH受体(GnRH-r)特异性竞争结合,通过调节GnRH-r基因的表达起到抑制GnRH活性的作用,且在给药数小时内即可发挥作用。
综上所述,对于接受IVF-ET助孕的不孕患者,GnRH-ant方案与GnRH-a方案比较,可获得同样满意的临床妊娠率,均为不孕患者IVF-ET的首选治疗方案,在临床中可以根据不同患者的实际情况灵活选择。本研究为不孕患者体外受精-胚胎移植的治疗提供了新思路。
[1] Lainas TG,Sfontouris IA,Zorzovilis IZ,et a1.Flexible GnRH antagonist protocol versus GnRH agonist long protocol in patients with polycystie ovary syndrome treated for IVF:a prospective randomized controlled trial (RCT)[J].Hum Reprod,2010,25(3):683-689.
[2] Kolibianakis EM,Venetis CA,Kalogeropoulou L,et al.Fixed versus flexible gonadotropin releasing hormone antagonist adminitralion in in vitro fertilization:a randomized controlled trial[J].Ferlil Steril,2011,95(2):558-562.
[3] 肖劲松, 陈双陨, 张春莲,等.促性腺激素释放激素拮抗剂在体外受精-胚胎移植中有效性的系统性评价[J].中国循证医学杂志,2010, 10(12):1432-1438.
[4] 杨硕, 陈新娜, 乔杰,等.GnRH拮抗剂固定方案和GnRH激动剂长方案在卵巢储备功能正常的不孕患者初次IVF-ET中的疗效比较[J].中华妇产科杂志,2012,47(4):245-249.
[5] Lainas TG,Sfontouris IA,Zorzovilis IZ,et a1.Flexible GnRH antagonist protocol versus GnRH agonist long protocol in patients with polycystie ovary syndrome treated for IVF:a prospective randomized controlled trial(RCT)[J].Hum Reprod,2010,25(3):683-689.
[6] Kolibianakis EM,Venetis CA,Kalogeropoulou L,et al.Fixed versus flexible gonadotropin-releasing hormone antagonist adminitralion in in vitro fertilization:a randomized controlled trial[J].Ferlil Steril,2011,95(2):558-562.
[7] Carranza A,Faya M,Merlo ML,et al.Effect of GnRH analogs in postnatal domestic cats[J].Theriogenology,2014,82(1):138-143.
[8] Taneja SS.Cardiovascular morbidity associated with gonadotropin releasing hormone agonists and anantagonist[J].J Uro,2014,191(4):985-986.
[9] Kim CH,Ahn JW,You RM,et al.Combined administration of gonadotropin-releasing hormone agonist with human chorionic gonadotropin for final oocyte maturation in GnRH antagonist cycles for in vitro fertilization[J].Reprod Med,2014,59(1):63-68.
[10] Lai Q,Zhang H,Zhu G,et al.Comparison of the GnRH agonist and antagonist protocol on the same patients in assisted reproduction during controlled ovarian stimulation cycles[J].Int J Clin Exp Pathol,2013,16(9):1903-1910.
[11] Pu D,Wu J,Liu J.Comparisons of GnRH antagonist versus GnRH agonist protocol in poor ovarian responders undergoing IVF[J].Hum Reprod,2011,26(10):2742-2749.
[12] Cota AM,Oliveira JB,Petersen CG,et al.GnRH agonist versus GnRH antagonist in assisted reproduction cycles:oocyte morphology[J].Reprod Biol Endocrinol,2012:10(1):33-34.
[13] Lai Q,Chen C,Zhang Z,et al.The significance of antral follicle size prior to stimulation in predicting ovarian response in a multiple dose GnRH antagonist protocol[J].Int J Clin Exp Pathol,2013,6(30):258-266.
[14] Prapas Y,Petousis S,Dagklis T,et al.GnRH antagonist versus long GnRH agonist protocol in poor IVF responders:a randomized clinical trial[J].Eur J Obstet Gynecol Reprod Biol,2013,166(12):43-46.
[15] Lavorato HL,Oliveira JB,Petersen CG,et al.GnRH agonist versus GnRH antagonist in IVF/ICSI cycles with recombinant LH supplementation:DNA fragmentation and apoptosis in granulosa cells[J].Eur J Obstet Gynecol Reprod Biol,2012;165(1):61-65.
[16] Berardelli R,Gianotti L,Karamouzis I,et al.Effects of cetrorelix,a GnRH-receptor antagonist,on gonadal axis in women with functional hypothalamic amenorrhea[J].Gynecol Endocrinol,2011,27(3):753-758.[17] Simon C,Oberyé J,Bellver J,et al.Similar endometrial development in oocyte donors treated with either high-or standard-dose GnRH antagonist compared to treatment with a GnRH agonist or in natural cycles[J]. Hum Reprod,2005,20(12):3318-3327.
(编校:谭玲)
Effect of gonadotropin releasing hormone antagonists and agonists on vitro fertilization and embryo transfer of patients with infertility
LI Dan-dan1,SHU Jing2
(1.Department of Obstetrics and Gynecology, The People’s Hospital of Shengzhou, Shengzhou 312400, China; 2.Department of Obstetrics and Gynecology, Shao Yifu Hospital of Medical College of Zhejiang University, Hangzhou 310016, China)
ObjectiveTo compare the clinical outcomes of gonadotropin releasing hormone antagonist(GnRH-ant)protocol and gonadotropin releasing hormone agonist(GnRH-a) protocol in infertile patients of their first vitro fertilization-embryo transfer (IVF-ET) cycle.Methods400 cases selected in Shengzhou people’s hospital from January 2013 to December 2013 undergoing the first controlled ovarian hyperstimulation and IVF-EF assisted reprodution, of which 200 cases using GnRH-ant scheme (young group and old group), and 200 cases were treated with GnRH-a (young group and old group).Through the detection of the general condition of patients, therapy,outcome of pregnancy and its clinical significance, to determine the GnRH-ant and GnRH-a feasibility.ResultsGnRH-ant young group (group A) and GnRH-ant old group (group B) were lower than the GnRH-a young group and GnRH-a elderly group in Gn time, Gn dosage, promoting excretion time, oocyte and mature oocyte number, respectively, which Gn time, Gn dosage and promoting excretion time had statistical significance (P<0.05), oocyte and mature oocyte number with no statistical significance.GnRH-ant young group (group A) and GnRH-ant old group (group B) were lower than the GnRH-a young group and GnRH-a elderly group in embryo implantation rate, clinical pregnancy rate and abortion rate, respectively, while ongoing pregnancy rate was higher, but with no statistical significance. ConclusionFor the infertility patients of control ovarian hgperstimulation and IVF-EF assisted reprodution, clinical pregnancy outcomes are good of GnRH-ant scheme and GnRH-a scheme, with no obvious difference.
gonadotropin releasing hormone; clinical protocols; fertilization in vitro; embryo transfer; pregnancy rate
2011年浙江省医药卫生计划(2011KYA085)
厉丹丹, 女,本科,主治医师,研究方向:妇科内分泌,不孕不育,E-mail:qch1821460010@163.com。
R321
A
1005-1678(2015)02-0149-03
猜你喜欢
中华活页文选·教师版(2022年19期)2022-12-31
中国典型病例大全(2022年16期)2022-06-10
家长(2021年20期)2021-12-03
食品安全导刊(2021年20期)2021-08-30
中华养生保健(2020年9期)2021-01-18
企业改革与管理(2021年10期)2021-01-02
就业与保障(2020年23期)2020-11-24
自我保健(2019年10期)2019-12-11
健康必读(上旬刊)(2019年9期)2019-10-21
中国实验动物学报(2019年4期)2019-09-03
