
急诊B超对肾绞痛病因的诊断效率
2016-08-25 09:45沈悦凡汪宁李辉钟欢王荣江浙江省湖州市第一人民医院泌尿外科浙江湖州313000
中国现代医生 2016年17期
沈悦凡 汪宁 李辉 钟欢 王荣江浙江省湖州市第一人民医院泌尿外科,浙江湖州 313000
急诊B超对肾绞痛病因的诊断效率
沈悦凡汪宁▲李辉钟欢王荣江
浙江省湖州市第一人民医院泌尿外科,浙江湖州313000
目的 探讨急诊B超对肾绞痛病因的诊断效率。方法 回顾性研究2014年8月~2015年9月行急诊B超检查的392例肾绞痛患者,其中228例行CT检查,采用χ2检验与Fisher确切概率法评价B超敏感性与结石大小、位置、肾积水的关系,运用Pearson双变量相关分析研究B超结石大小与CT的相关性。结果 急诊B超诊断输尿管结石敏感性为90.5%,对上、中、下段结石敏感性分别为98.5%、83.8%、81.9%(P<0.05),对<6 mm,6~10 mm,10~20 mm,>20 mm结石敏感性依次为73.9%、93.9%、95.7%、100.0%(P<0.05),B超在有肾积水与无肾积水条件下检测结石敏感性分别为92.0%、72.0%,B超检测结石大小与CT高度相关,其Pearson相关系数为0.781(P<0.05)。结论 急诊B超诊断肾绞痛患者的病因非常有效,其敏感性随结石增大而增加,上段结石高于中、下段,有肾积水高于无肾积水,特别对于>6 mm的结石,B超与CT结石大小有较高符合率。
输尿管结石;B超;敏感性;CT;相关性
[Abstract]Objective To explore the diagnosis effect of emergency B ultrasound on the pathogenesis of renal colic. Methods A total of 392 patients with renal colic who received emergency B ultrasound examination from August 2014 to September 2015 were retrospectively investigated.Among them,228 patients were given CT examination,and χ2test and Fisher's exact test were applied to evaluate the correlation between the sensitivity of B ultrasound and calculus size,position and hydronephrosis.Pearson's bivariate correlation analysis was applied to study the correlation between B ultrasound and CT in the diagnosis of calculus size.Results The sensitivity of emergency B ultrasound in the diagnosis of ureteral calculus was 90.5%.The sensitivity in the diagnosis of upper,middle calculus and lower calculus was 98.5%,83.8%and 81.9%respectively(P<0.05).The sensitivity in the diagnosis of the calculus smaller than 6 mm,6-10 mm,10-20 mm and larger than 20 mm was 73.9%,93.9%,95.7%and 100.0%respectively(P<0.05).The sensitivity of B ultrasound with hydronephrosis and without hydronephrosis in the diagnosis of calculus was 92.0%and 72.0%.B ultrasound was largely correlated to CT in the diagnosis of calculus size,and Pearson correlation coefficient was 0.781 (P<0.05).Conclusion Emergency B ultrasound in the diagnosis of the pathogenesis of renal colic is highly effective,and its sensitivity increases along with the increasing calculus size.The sensitivity is higher in upper calculus than in lower,middle calculus,and the sensitivity is higher with hydronephrosis than without hydronephrosis.Especially for the calculus larger than 6 mm,B ultrasound and CT in the diagnosis of calculus size have higher accordance rate.
[Key words]Ureteral calculus;B ultrasound;Sensitivity;CT;Correlation
我国泌尿系结石发病率1%~5%,其中南方人高达5%~10%,3%~15%成年人一生中经历肾绞痛[1,2]。目前公认的金标准多层螺旋CT诊断结石敏感性及特异性接近100%[1],但其价格昂贵、辐射剂量大,一些基层医院缺乏相关设备。相对而言B超检查价格便宜,无放射线损害,其敏感性高于腹部卧位片[2,3],且多数基层医院不缺乏相关设备。随设备更新及操作人员技术不断提高,B超敏感性及特异性较以往提高,目前体外震波碎石术(ESWL)设备大多用B超定位,临床医师更希望B超在发现结石的基础上提供更多信息以指导下一步治疗,而结石大小是决定治疗方式的重要因素[4],国外T Kanno等[5]研究发现输尿管结石在B超与CT大小的Pearson相关系数为0.773,国内尚缺乏这方面研究。本文选择2014年8月~2015年9月肾绞痛患者,以CT为金标准,研究B超检出结石大小与CT符合程度,并探讨B超敏感性与结石大小、位置及肾积水的关系,现报道如下。
1 资料与方法
1.1一般资料
回顾研究2014年8月~2015年9月行B超检查的392例肾绞痛患者,男208例,女184例,年龄24~78岁,平均(48.6±13.6)岁,结石最小2.5 mm,最大20 mm,平均(10.15±4.64)mm,其中228例行CT检查。
1.2结石大小判定方法
结石大小均取自CT与B超测量的结石最长径,B超结果随机由急诊B超医师判定,CT结果由两位有经验的放射科医师共同判定。设备信息:德国SIEMENS公司生产的 SOMATOM Spirit双排螺旋CT,荷兰PHILIPS公司生产PHILIPS HDI5000彩色超声诊断仪。
1.3观察指标
综合B超与CT检查结果,评价B超敏感性与结石大小、位置、积水程度的关系。在228例中,排除多发结石、结石位置改变、治疗后复查CT、假阳性等特殊情况,进一步比较余145例患者B超与CT结石大小符合程度。
1.4统计学处理
所有数据均采用SPSS 18.0统计学软件进行统计分析,其中计量资料以均数±标准差(x±s)表示,计数资料采用χ2检验或Fisher确切概率法,B超结石大小与CT的符合程度运用Pearson双变量相关分析研究,P<0.05为差异有统计学意义。
2 结果
2.1B敏感性与结石位置的关系
在随机选取的392例患者中,B超提示356例结石阳性,其中6例假阳性,6例多发,予排除,B超检测输尿管结石敏感性为90.5%,其中上、中、下段结石敏感性依次下降,分别为98.5%、83.8%、81.9%差异有统计学意义(Fisher精确检验,P<0.05)。见表1。
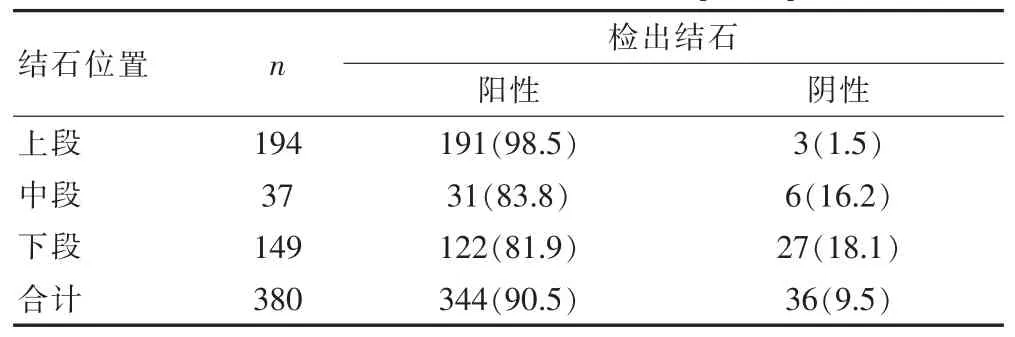
表1 B超敏感性与结石位置关系[n(%)]
2.2B超敏感性与结石大小的关系
结石大小也影响B超敏感性,<6 mm的光滑结石通常可自行排除体外,而>10 mm的结石很难排出[1],接受CT检查的228例中,按CT所示分为4组(表2):X≤6mm、6mm<X<10mm、10mm≤X<20mm、X≥20 mm,四组B超结石检测敏感性依次增加,分别为73.9%、93.9%、95.7%、100.0%,差异有统计学意义(Fisher精确检验,P<0.05)。见表2。

表2 B超敏感性与结石大小的关系[n(%)]
2.3B超敏感性与肾积水的关系
若结石梗阻部位以上肾及输尿管积水,容易发现梗阻处。6例多发结石也纳入研究。B超在有肾积水与无肾积水条件下检测结石敏感性分别为92.0%、72.0%,差异有统计学意义(χ2=11.022,P<0.05)。见表3。
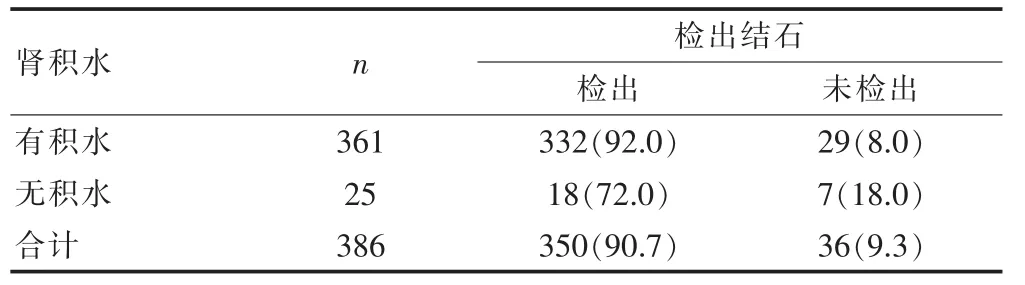
表3 B超敏感性与肾积水的关系系[n(%)]
2.4B超与CT结石大小相关性
228例行CT检查的患者,排除多发结石、结石位置改变、治疗后复查CT、假阳性等特殊情况,纳入研究145例,我们发现B超检测结石大小与CT数据高度相关(Pearson相关系数0.781,P<0.05)。按结石大小分为4组,观察分组后B超与CT结果是否仍符合:X≤6 mm、6 mm<X<10 mm、10 mm≤X<20 mm、X≥20 mm,其Pearson相关系数分别为0.146(P>0.05)、0.475(P<0.05)、0.360(P<0.05)、0.585(P<0.05),其中6 mm<X<10 mm与X≥20 mm两组相关程度较高。
3 讨论
既往研究认为B超诊断输尿管结石的价值有限,其敏感性波动于19%~93%之间[6],而我们的数据提示B超敏感性为90.5%。最新指南认为对于>5 mm的上段结石,其敏感性可达96%,而所有部位结石,敏感性仅为78%[1],研究发现使用彩色多普勒B超联合腹部卧位片检查可提高敏感性[7],彩色多普勒B超的“闪烁征(twinkling sign)”可发现<5 mm结石,其敏感性高于传统超声[8,9]。我们纳入研究患者均为肾绞痛患者,大多数患者伴有肾积水,引起B超医师仔细观察输尿管各段,加之使用彩色多普勒,这可能是我们B超敏感性较高的原因。
研究表明B超敏感性随结石增大相应提高[5,10]。上段、中段结石B超敏感性较高,而下段结石敏感性较低[11],这与我们的结果一致,其原因可能为多数人行B超检查时膀胱未充盈或因尿频、尿急、肾绞痛而充盈困难。Moesbergen等[12]研究发现如B超检查时膀胱容量>110 mL,漏诊率可由16%减少至1%,因此如怀疑输尿管结石,可于止痛治疗后督促患饮足量水,充盈膀胱后行B超检查,若是女性患者,经阴道检查也能提高敏感性[13]。
有研究显示[14],超声诊断肾积水的敏感性为72.6%,特异性为73.3%,我们研究发现肾积水可为B超医师提供明确参考,B超在有肾积水的条件下检测结石敏感性为92.0%。虽然肾绞痛结合梗阻病理征象“肾积水”间接提示输尿管结石,但近50%腰腹痛并非由输尿管结石引起,单纯通过肾积水和腰腹痛判断输尿管结石不可靠,容易引起误诊[5,15]。
结石大小是输尿管结石治疗决策的最重要依据[16-19],通过多饮水及适量运动,98%<5 mm的光滑结石可自行排除体外,结石>6 mm时可以考虑外科治疗,但对<10 mm的结石,观察等待仍可首选,>10 cm的结石通常需要外科治疗[1,20]。我们研究发现B超检测结石大小与CT高度相符(Pearson相关系数0.781),但分组后各相关系数偏低,可能与样本量减小有关,其中6~10 mm组及≥20 mm组符合程度仍然较高,且假阳性只有2例(0.017%)。目前大多数ESWL使用B超定位,我们的结果提示对于6~10 mm组体外震波碎石患者,可根据B超检查结果决定碎石;少数肾功能不全、孤立肾、多发结石、双侧结石、无肾积水、输尿管狭窄患者,或自行排石及ESWL失败患者,CT检查仍是必须的;对于结石10~20 mm患者,因Pearson相关系数小,建议CT检查明确结石大小后决定下一步治疗方式。
本文研究B超在诊断泌尿系结石中的作用,重点研究B超检出结石大小与CT符合程度,并探讨B超检出率与结石大小、位置及肾积水的关系,样本量较大,但作为回顾性研究仍有许多不足之处:①患者经分诊后大多因肾绞痛就诊,符合输尿管结石典型症状,容易造成入院偏倚,人为增加B超敏感性;②多数行CT检查的患者因B超未检出结石,需住院进一步诊治,在比较CT与B超结石大小符合程度时这部分患者占很大比例,也是偏倚因素之一;③资料统计完全依赖病历,信息偏倚较前瞻性研究与随机对照研究更大。
综上所述,B超价格低廉,无放射污染,敏感性高,诊断肾绞痛患者的病因非常有效,特别对于>6 mm的结石,B超与CT有较高符合率。因此,我们建议B超作为肾绞痛患者及输尿管结石随访的首选检查。
[1]那彦群,叶章群,孙颖浩,等.中国泌尿外科疾病诊断治疗指南[J].北京:人民卫生出版社,2014:267-329.
[2]PJ Dalziel,VE Noble.Bedside ultrasound and the assessment of renal colic:A review[J].Emerg Med J,2013,30(1):3-8.
[3]Nicolau C,Claudon M,Derchi LE,et al.Imaging patients with renal colic-consider ultrasound first[J].Insights Into Imaging,2015,6(4):1-7.
[4]Sahin C,Cetinel AC,Eryildirim B,et al.Stone size and quality of life:A critical evaluation after extracorporeal shock wave lithotripsy[J].Arch Ital Urol Androl,2015,87 (3):227-232.
[5]Kanno T,Kubota M,Sakamoto H,et al.Determining the efficacy of ultrasonography for the detection of ureteral stone[J].Urology,2014,84(3):533-537.
[6]Viprakasit DP,Sawyer MD,Herrell SD,et al.Limitations of ultrasonography in the evaluation of urolithiasis:A correlation with computed tomography[J].J Endourol,2012,26(3):209-213.
[7]Abdel-Gawad M,Kadasne R,Anjikar C,et al.Value of Color Doppler ultrasound,kub and urinalysis in diagnosis of renal colic due to ureteral stones[J].Int Braz J Urol,2014,40(4):513-519.
[8]Vallone G,Napolitano G,Fonio P,et al.US detection of renal and ureteral calculi in patients with suspected renal colic[J].Crit Ultrasound J,2013,5(Suppl 1):S3.
[9]Sorensen MD,Harper JD,Hsi RS,et al.B-mode ultrasound versus color Doppler twinkling artifact in detecting kidney stones[J].Journal of Endourology,2013,27(2):149-153.
[10]Bader MJ,Eisner B,Porpiglia F,et al.Contemporary management of ureteral stones[J].Eur Urol,2012,61(4):764-772.
[11]Moore CL,Bomann S,Daniels B,et al.Derivation and validation of a clinical prediction rule for uncomplicated ureteral stone-the STONE score:Retrospective andprospective observational cohort studies[J].BMJ,2014,348:2191.
[12]Moesbergen TC,de Ryke RJ,Dunbar S,et al.Distal ureteral calculi:US follow-up[J].Radiology,2011,260(2):575-580.
[13]Mitterberger M,Pinggera GM,Maier E,et al.Value of 3-dimensional transrectal/transvaginal sonography in diagnosis of distal ureteral calculi[J].J Ultrasound Med,2007,26(1):19-27.
[14]Herbst MK,Rosenberg G,Daniels B,et al.Effect of provider experience on clinician-performed ultrasonography for hydronephrosis in patients with suspected renal colic[J].Ann Emerg Med,2014,64(3):269-276.
[15]Song Y,Hernandez N,Gee MS,et al.Can ureteral stones cause pain without causing hydronephrosis?[J].World Journal of Urology,2015,10:1-4.
[16]Nakasato T,Morita J,Ogawa Y.Evaluation of Hounsfield Units as a predictive factor for the outcome of extracorporeal shock wave lithotripsy and stone composition[J]. Urolithiasis,2015,43(1):69-75.
[17]Matlaga BR,Jansen JP,Meckley LM,et al.Treatment of ureteral and renal stones:A systematic review and metaanalysis of randomized,controlled trials[J].The Journal of Urology,2012,188(1):130-137.
[18]Castro EP,Osther PJ,Jinga V,et al.Differences in ureteroscopic stone treatment and outcomes for distal,mid,proximal,or multiple ureteral locations:The clinical research office of the endourological society ureteroscopy global study[J].European Urology,2014,66(1):102-109.
[19]Remer EM,Herts BR,Primak A,et al.Detection of urolithiasis:comparison of 100%tube exposure images reconstructed with filtered back projection and 50%tube exposure images reconstructed with sinogram-affirmed iterative reconstruction[J].Radiology,2014,272(3):749-756.
[20]Pearle MS,Goldfarb DS,Assimos DG,et al.Medical management of kidney stones:AUA guideline[J].J Urol,2014,192(2):316-324.
Diagnosis effect of emergency B ultrasound on the pathogenesis of renal colic
SHEN YuefanWANG NingLI HuiZHONG HuanWANG Rongjiang
Department of Urology,Huzhou First People's Hospital in Zhejiang Province,Huzhou313000,China
R691
B
1673-9701(2016)17-0077-04
浙江省医药卫生平台计划骨干人才项目(2016R CB019)
▲
(2015-10-19)
猜你喜欢
中国药学药品知识仓库(2022年10期)2022-05-29
实用医院临床杂志(2021年2期)2021-03-20
中国生殖健康(2020年7期)2021-01-18
世界最新医学信息文摘(2021年35期)2021-01-10
小雪花·初中高分作文(2019年11期)2019-02-12
作文周刊·小学一年级版(2018年25期)2018-10-20
初中生世界·九年级(2017年9期)2017-10-13
中外医疗(2016年15期)2016-12-01
济宁医学院学报(2014年4期)2014-08-16
河南医学研究(2014年4期)2014-02-27
