骨水泥强化椎弓根螺钉技术应用于脊柱肿瘤外科治疗的临床疗效探究
2016-09-07 03:24钟南哲严望军魏海峰刘铁龙肖建如杨兴海
中国骨与关节杂志 2016年8期
钟南哲 严望军 魏海峰 刘铁龙 肖建如 杨兴海
骨水泥强化椎弓根螺钉技术应用于脊柱肿瘤外科治疗的临床疗效探究
钟南哲 严望军 魏海峰 刘铁龙 肖建如 杨兴海
目的 探究骨水泥强化椎弓根螺钉技术应用于脊柱肿瘤合并邻近椎节骨质量不佳患者术后脊柱稳定性重建的有效性和安全性。方法 回顾分析 2012 年 12 月至 2014 年 11 月,于我科采用骨水泥强化椎弓根螺钉技术治疗脊柱肿瘤合并邻近椎节骨质量不佳的 35 例患者术后脊柱稳定性重建的临床资料,其中男22 例,女 13 例;年龄 40~76 岁,平均(58.1±8.5)岁。对术后骨水泥在椎体内的弥散情况及与椎体和螺钉的相对位置行具体探究。结果 本组随访时间为 14~37 个月,平均(28.3±4.6)个月。随访时美国脊髓损伤协会(American spinal cord injury association,ASIA)、视觉模拟疼痛评分(visual analogue scale,VAS)较术前均有显著改善。后凸平均矫正率为 54.8%,末次随访平均丢失角为 0.6°,侧凸平均矫正率为 71%,末次随访平均丢失角为 0.3°。术前及术后冠状位 Cobb’s 角分别为(6.0±6.4)° 和(1.5±2.3)°,术前及术后矢状位 Cobb’s 角分别为(14.1±12.8)° 和(11.2±8.1)°,差异均有统计学意义;术后 3 个月与末次随访冠状位及矢状位 Cobb’s 角无明显改变。随访复查影像学显示所有患者椎间植骨融合情况良好,未发现手术相关并发症。无内固定失败事件发生。骨水泥多对称分布在螺钉尖端及钉道旁。骨水泥分布于前柱占 73.4%,分布于前柱及中柱前部占26.6%。骨水泥弥散-钉道半径比 95% CI:1.80~3.14,骨水泥弥散-钉道深度比 95% CI:64.6%~92.2%,钉道-骨水泥弥散体积比 95% CI:10.1%~40.6%,骨水泥弥散-椎体体积比 95% CI:2.0%~20.2%,骨水泥弥散长度-椎体直径比 95% CI:43.3%~66.1%。结论 骨水泥强化椎弓根螺钉技术可安全有效地实现脊柱肿瘤合并邻近椎节骨质量不佳患者接受病灶切除术后脊柱的稳定性。有助于缓解患者局部疼痛、恢复脊髓神经功能及维持脊柱稳定性。而该内固定方法成功操作的关键在于获得合理的骨水泥弥散分布方式。
骨水泥成形术;椎弓根钉;骨肿瘤;脊柱
随着脊柱外科水平的提高及对脊柱肿瘤认识的深入,外科手术为主的综合治疗已成为脊柱肿瘤治疗的主要手段。而脊柱肿瘤外科治疗的稳定性重建要求明显高于常规脊柱疾病,其中涉及多种因素,包括:部分脊柱肿瘤高发年龄段为 40 岁以上,而很多高龄脊柱肿瘤患者常合并有老年性骨质疏松[1-2];许多原发性脊柱肿瘤以及转移性脊柱肿瘤可通过影响肿瘤局部乃至全身骨稳态,引发脊柱肿瘤邻近椎节甚至全脊柱骨密度下降[3-5],导致椎骨对椎弓根螺钉的把持力下降,易发生螺钉松动而造成内固定失败。骨水泥强化椎弓根螺钉技术作为增强螺钉把持力的有效手段,近年来已成功应用于退行性脊柱疾患的手术治疗[6],但该项技术应用于脊柱肿瘤治疗的临床研究尚未见报道。2012 年 11 月至 2014 年11 月,我科对 35 例脊柱肿瘤合并邻近椎节骨质量不佳患者采用骨水泥强化椎弓根螺钉技术重建,获得较好疗效,总结报告如下。
资料与方法
一、一般资料
本组 35 例,其中男 22 例,女 13 例;年龄40~76 岁,平均(58.1±8.5)岁。转移性脊柱肿瘤27 例,其中肺癌转移 14 例,结肠癌转移 6 例,肝癌转移 3 例,子宫内膜癌转移 2 例,乳腺癌转移2 例;原发性脊柱肿瘤 8 例,其中骨肉瘤 2 例,多发性骨髓瘤 5 例,浆细胞性骨髓瘤 1 例。27 例转移癌患者的 Tomita 评分 6~8 分,平均(7.2±0.6)分,中位评分为 7 分。所有患者视觉模拟疼痛评分(visual analogue scale,VAS)1~9 分,平均(5.2± 2.3)分。美国脊髓损伤协会(American spinal cord injury association,ASIA)评分详见表 1。患者术前均有不同程度腰背疼痛,其中 6 例伴单侧下肢麻痛,19 例伴双侧下肢麻痛,14 例伴间歇性跛行,患者均经系统保守治疗无效。所有患者评价心肺功能均正常,可耐受肿瘤切除及内固定手术。手术目标区邻近椎节骨质量不佳原因:骨质疏松 23 例 [ 平均 T 分数为(-2.77±0.32)SD ],因肿瘤破坏所致 12 例。
二、术前处理及评估
患者入院后接受常规术前检查。术前对患者行影像学检查,包括:胸腰椎正侧位 X 线、CT 以及 MRI 检查,结合血常规及肿瘤标志物结果明确诊断及骨累及范围,同时对患者腰椎行双能 X 线骨密度测量(dual energy X-ray absorptiometry,DXA)评估脊柱骨质疏松情况。对骨髓瘤患者行骨穿刺以明确,其余患者病理类型待术后病理结果评估。全面评估患者的全身情况,对合并内科基础疾病的患者进行必要的治疗。
三、手术方法及术后处理
患者取俯卧位,全身麻醉并注意保护受压部位。后正中手术入路,透视定位病椎后常规暴露需手术切除固定节段椎体的棘突、双侧椎板、关节突关节。术中透视定位,并对邻近骨质量不佳节段椎弓根依次行开口、开路、置入导针,C 型臂 X 线机透视确定针位置及方向正确后,预置攻丝。调制骨水泥,当其至面团前期时将其灌入骨水泥推杆,在透视监视下,每个钉道缓慢地注入约 1.5~2.0 ml 骨水泥,观察骨水泥在椎体内的弥散情况,植入椎弓根螺钉,透视确定螺钉位置及骨水泥在椎体内的弥散情况。根据术前计划实施肿瘤的切除与重建,后连接棒预弯,双侧螺钉上棒并锁定,安装横连接、锁定。常规放置引流,关闭切口。引流管常规术后1 周拔除。所有患者卧床休息,防止褥疮,术后均戴支架保护半年以上,每半年定期复查 X 线,了解植骨融合的情况。并根据患者实际情况行相应放化疗等辅助治疗。
四、评估标准
分别于术前及随访时复查和评估以下观察指标:(1)单个椎体的平均骨水泥注入量;(2)骨水泥分布情况;(3)骨水泥渗漏率;(4)椎间植骨融合的成功率;(5)内固定失败率;(6)VAS 评分;(7)ASIA 神经功能分级;(8)脊柱后凸及侧凸角度(Cobb’s 角);(9)椎体压缩率及恢复率。
其中,笔者设计骨水泥分布情况按如下方法评估:(1)骨水泥是否均匀分布于螺钉周围;(2)骨水泥分布较椎体三柱位置;(3)测量侧位 X 线植入螺钉椎体椎体高度(H)、椎体直径(D)、椎体内钉道长度(h)、钉道直径(d)、骨水泥弥散长度(h’)、骨水泥弥散直径(d’)(图 1)。骨水泥弥散-钉道半径比=d’ / d,骨水泥弥散-钉道长度比=h’ / h,钉道-骨水泥弥散体积比=[(d’ / 2)2×h’ ] / [(d / 2)2×h ],骨水泥弥散-椎体体积比=[(d’/2)2× h’]/[(D/2)2×H],骨水泥弥散长度-椎体直径比=h’/D。
五、统计学处理
采用 SPSS 18.0 软件行统计学分析。计量资料采用± s 表示。组间各项指标通过配对 t 检验进行比较。P<0.05 为差异有统计学意义。
结 果
本组 35 例手术过程平稳,其中采用后方入路 33 例,后外方入路 2 例;刮除 5 例,分块切除19 例,en bloc 切除 11 例;单节段切除重建 34 例,双节段切除重建 1 例;内固定节段,2 节段 1 例,3 节段 4 例,4 节段 24 例,5 节段 1 例,6 节段4 例;8 节段 1 例。使用骨水泥强化椎弓根螺钉钉道技术共置入螺钉 143 枚;单一钉道注入骨水泥量 1.2~3.5 ml,平均(1.69±0.41)ml;手术时间90~420 min,平均(242.1±70.3)min;术中出血量600~4000 ml,平均(1951.4±1002.8)ml。无椎管内渗漏发生,2 例术中透视发现节段静脉少量渗漏,未引起临床症状。

图1 测定骨水泥椎体内分布情况示意图 [ 椎体高度(H)、椎体直径(D)、椎体内钉道长度(h)、钉道直径(d)、骨水泥弥散长度(h’)、骨水泥弥散直径(d’)]Fig.1 Illustration for the measurement of the bone cement distribution inside the vertebrae(H: the height of the vertebrae,D: the diameter of the vertebrae, h: the length of the screw inside the vertebrae, d: the diameter of the screw, h’: the length of bone cement distributing in the vertebrae, d’: the diameter of bone cement distributing in the vertebrae)
患者术后随访时间为 8~31 个月,平均(28.3± 4.6)个月。其中 20 例转移癌患者因疾病进展死亡,中位生存时间 27 个月。使用 ASIA、VAS 评分对患者术前及随访状况行评价(表 1、2)。随访时两项指标均较术前有显著改善,差异有统计学意义(P<0.0001)。后凸平均矫正率为 54.8%,末次随访平均丢失角为 0.6°,侧凸平均矫正率为 71%,平均末次随访丢失角为 0.3°。术前及术后冠状位 Cobb’s 角分别为(6.0±6.4)° 和(1.5±2.3)°,术前及术后矢状位 Cobb’s 角分别为(14.1±12.8)° 和(11.2±8.1)°,相比差异均有统计意义(P<0.0001),术后 3 个月与末次随访冠状位及矢状位 Cobb’s 角无明显改变,差异无统计学意义(P=0.083;P=0.081)(表 2)。
随访复查影像学显示所有患者椎间植骨融合情况良好,未发现手术相关并发症。无断钉、断棒、内固定移位等内固定失败事件发生。骨水泥多对称分布在螺钉尖端及钉道旁(图 2、3)。骨水泥分布于前柱占 73.4%,分布于前柱及中柱前部占 26.6%。骨水泥弥散-钉道半径比 95% CI:1.80~3.14,骨水泥弥散-钉道深度比 95% CI:64.6%~92.2%,钉道-骨水泥弥散体积比 95% CI:10.1%~40.6%,骨水泥弥散-椎体体积比 95% CI:2.0%~20.2%,骨水泥弥散长度-椎体直径比 95% CI:43.3%~66.1%(图 4)。

表1 患者术前及末次随访时 ASIA 分级(例)Tab.1 The comparison of ASIA staging preoperatively and in the last follow-up(case)
表2 患者术前及随访时各临床指标比较(± s)Tab.2 The comparison between pre- and post-operative clinical parameters(± s)

表2 患者术前及随访时各临床指标比较(± s)Tab.2 The comparison between pre- and post-operative clinical parameters(± s)
指标 术前 术后 3 个月 末次随访 术前与末次随访比较 P 值 术后 3 个月与末次随访比较 P 值VAS 评分(分) 5.2± 2.3 - 2.9±1.6 <0.0001 -冠状位 Cobb’s 角(°) 6.0± 6.4 1.5±2.3 1.7±2.5 <0.0001 0.0832矢状位 Cobb’s 角(°) 19.7±11.9 13.1±7.7 12.7±7.8 0.0008 0.0674

图2 术后 CT 平扫影像示骨水泥对称分布在螺钉尖端及钉道旁Fig.2 Postoperative CT scan revealed an even distribution of bone cement around the tips and the tracts of screws
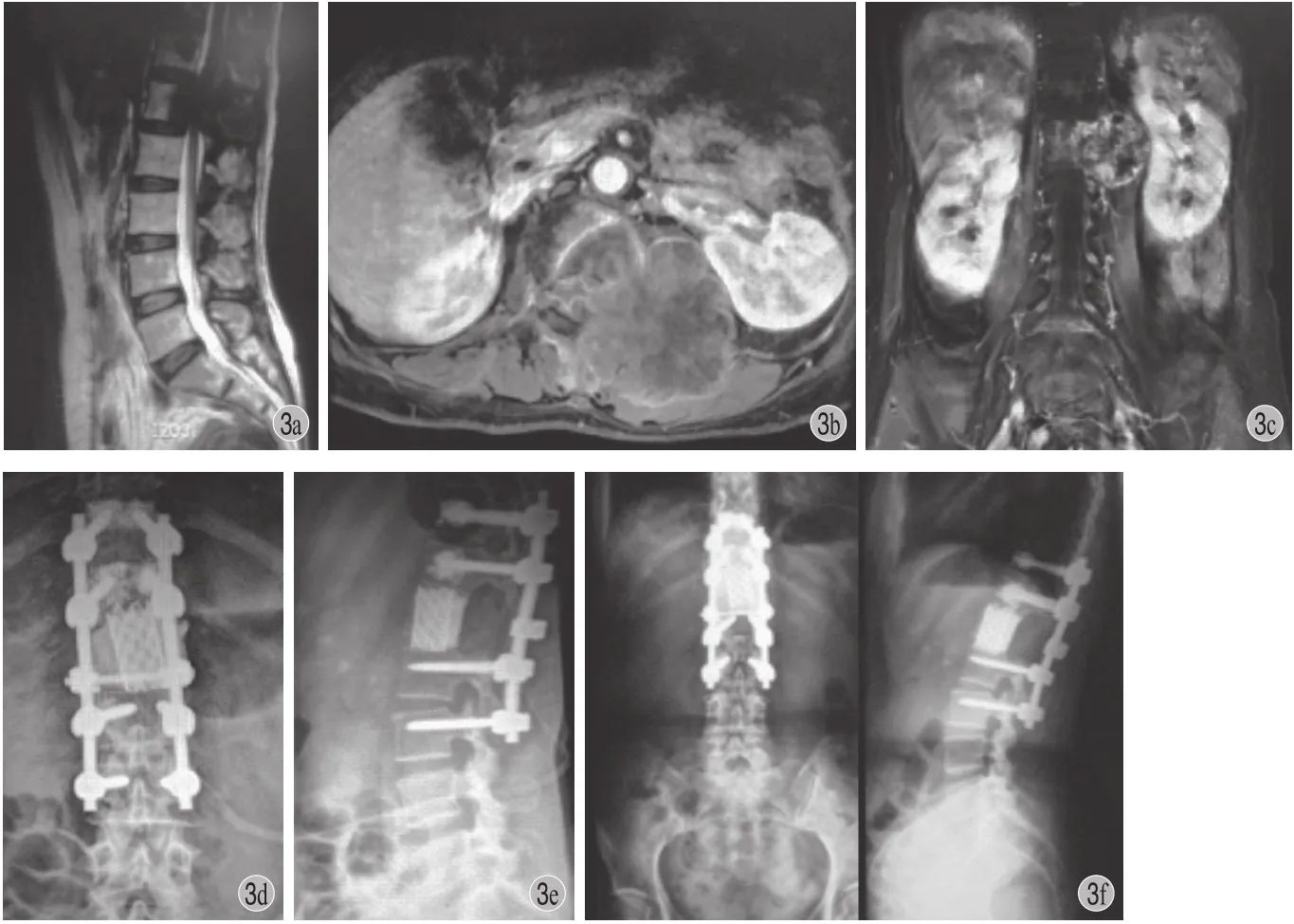
图3 患者,女,55 岁,结直肠癌脊柱转移,行骨水泥强化椎弓根螺钉技术重建 a~c:术前 MRI 示 L1椎体附件及椎旁肿瘤,邻近 T11~12椎体信号异常,骨质破坏;d~e:术后 1 个月 X 线片;f:术后26 个月随访 X 线片示内固定在位良好Fig.3 A 55-year-old female with metastatic colorectal carcinoma of the spine. The pedicle screw cement augmentation was performed after tumor resection a - c: The preoperative MRI images illustrated the tumor located at the appendix of L1with abnormal MRI signals in T11and T12; d - e: The X-ray image of instrumentation 1 month after the surgery; f: The X-ray image of instrumentation 26 months after the surgery showed no failures of the internal fixation
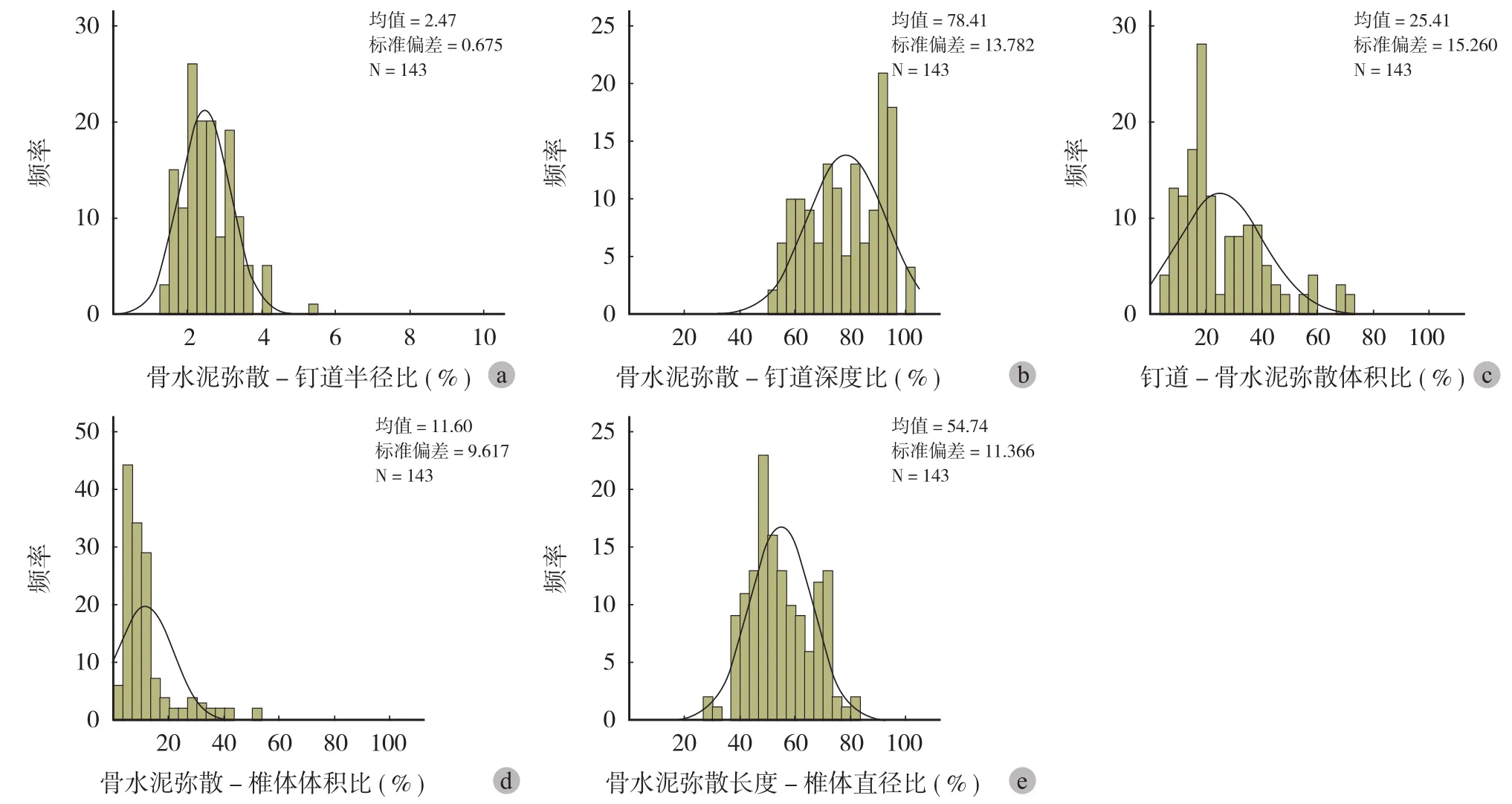
图4 骨水泥强化椎弓根螺钉技术应用于脊柱肿瘤手术治疗稳定性和安全性的评估指标 a:骨水泥弥散-钉道半径比;b:骨水泥弥散-钉道深度比;c:钉道-骨水泥弥散体积比;d:骨水泥弥散-椎体体积比;e:骨水泥弥散长度-椎体直径比Fig.4 The parameters evaluating the safety and stability of pedicle screw cement augmentation on spine tumor surgery a: The ratio of the diameter of bone cement distribution versus the diameter of the screw; b: The ratio of the length of bone cement distribution versus the length of the screw; c: The ratio of the volume of the screw versus that of bone cement distribution; d: The ratio of the volume of bone cement distribution and that of the vertebrae; e: The ratio of the length of bone cement distribution and the diameter of the vertebrae
讨 论
脊柱肿瘤按其来源可以分为原发脊柱肿瘤和转移性脊柱肿瘤,对于此类患者,手术治疗可有效控制疾病进展,改善患者生活质量,延长生存时间。然而,由于脊柱肿瘤转移患者年龄较高[7],常患有老年性骨质疏松,且脊柱肿瘤可造成邻近椎节的骨质破坏,这就使得脊柱肿瘤合并有邻近椎节骨质量不佳的情况并不少见。此外,相较于其它脊柱手术而言,对脊柱稳定性多造成更大的破坏。因而,脊柱肿瘤手术对术后脊柱稳定性重建有更高要求,如果椎弓根螺钉松动甚至脱出,进而造成内固定失败事件,可严重影响患者生活质量,甚至加速患者死亡,因此选择合理、安全及有效的内固定方式对脊柱肿瘤手术的成败至关重要。
骨水泥强化椎弓根螺钉技术近年已较广泛地应用于各种合并骨质量不佳的脊柱疾患的手术治疗中,包括先天畸形、外伤、脊柱退行性病变等,临床观察效果良好[6,8-9],但应用于脊柱肿瘤治疗是否有效尚未见报道。椎弓根螺钉经骨水泥强化后,能有效地提高其固定强度,防止脊柱固定节段发生螺钉松动拔出的情况,满足患者坚强脊柱内固定的要求,相关力学实验也证实了该技术确可改善骨质不良椎体对螺钉握持力不足的情况[1]。笔者体会,该技术应用于脊柱肿瘤合并有邻近椎节骨质量不佳的手术治疗的参考性适应证主要包括:(1)骨密度检测骨质疏松:骨密度检测较峰值骨量减少2.5 SD[10];(2)固定节段骨质被肿瘤破坏。此类患者的术中探查特点为骨质松软,甚至呈海绵状改变。本研究通过评估患者 VAS、ASIA 评分等指标,发现接受骨水泥强化椎弓根螺钉内固定患者术后随访症状及神经功能情况较术前有显著改善。此外,通过比较分析,患者术前与术后 3 个月冠状位及矢状位Cobb’s 角有显著差异,术后 3 个月与末次随访冠状位及矢状位 Cobb’s 角无明显改变(图 3),提示骨水泥强化椎弓根螺钉技术应用于邻近椎节骨质量不佳的脊柱肿瘤切除后内固定有良好的稳定性,可有效纠正因肿瘤导致脊柱畸形。
合理的骨水泥分布是保证骨水泥强化椎弓根螺钉最终强度的关键因素之一,从而获得最大的骨水泥-螺钉接触面积。以往研究普遍认为骨水泥对称分布于螺钉周围骨水泥强化效果较佳[11-12]。Liu 等[13]通过有限元方法对椎弓根螺钉植入后模拟骨质疏松骨块抗拔出力的应力分布情况行生物力学分析后发现,根据骨质疏松程度的不同,在螺钉周围半径为 4.73~5.40 mm 的范围内存在一个环形区域,其所受应力最大,是抗螺钉拔出的关键区域,因此,使用骨水泥强化椎弓根螺钉时骨水泥弥散分布于该区域时可有效提高其抗拔出力。Hu 等[14]通过 CT 影像,将椎体及椎弓根分成 4 个区域(椎体前 1 / 3、椎体中 1 / 3、椎体后 1 / 3 和椎弓根)后,对接受骨水泥强化椎弓根螺钉内固定患者的固定效果行回顾性分析,认为弥散分布于前 3 个区域可获得最佳生物力学强度且安全性良好。与之相似,Shih 等[15]的研究表明,骨水泥分布于椎体后 2 / 3 可显著提高螺钉的抗拔出力。为实现该分布特点,可在椎体中部行骨水泥注入,由于目前临床实践中,尚缺乏可有效评估骨水泥强化椎弓根螺钉技术应用于脊柱肿瘤手术治疗稳定性和安全性的相关指标,本研究对接受骨水泥强化椎弓根螺钉内固定后稳定性良好的病例的影像学资料进行分析,总结其骨水泥分布特点。结果显示骨水泥分布于前柱占 73.4%。骨水泥弥散-钉道半径比 95% CI:1.80~3.14,骨水泥弥散-钉道深度比 95% CI:64.6%~92.2%,钉道-骨水泥弥散体积比 95% CI:10.1%~40.6%,骨水泥弥散-椎体体积比 95% CI:2.0%~20.2%,骨水泥弥散长度-椎体直径比 95% CI:43.3%~66.1%,提示符合上述骨水泥弥散范围的骨水泥强化椎弓根螺钉操作可获得较良好稳定性和安全性。从大体弥散形态而言,骨水泥在弥散螺钉周围弥散呈圆柱形可提供更好的抗拔出力[16]。
此外,PMMA 骨水泥强化钉道技术可能造成的并发症也应引起足够的重视,其中主要包括神经损伤、骨水泥毒性、肺栓塞和骨水泥渗漏等[17-20]。预防骨水泥强化椎弓根螺钉中出现骨水泥渗漏的要点较多,其中骨水泥用量的安全范围为众多研究所关注。部分研究认为每一钉道可注入 3 ml 骨水泥[14,17,21],而其它研究结果提示每一钉道注入 1.0~2.5 ml 较为安全[11,22]。本研究实践中平均单一钉道注入骨水泥量(1.69±0.41)ml,术后稳定性佳,并发症少,提示该骨水泥用量可实现内固定有效性和安全性的最佳平衡。同时,骨水泥的分布也和骨水泥渗漏的发生有密切关系。尽管有研究显示使骨水泥最大程度上分布于钉道全长周围可提供最大的抗拔出力[23],即骨水泥分布于椎体和椎弓根的所有区域为理想的骨水泥分布方式,但在实际操作中该方法会大大提高骨水泥渗漏的发生率[14]。笔者通过本组病例的观察也证实使骨水泥主要分布于前柱有较好的手术安全性。此外,骨水泥黏稠度、导针置入的方向和深度及推入骨水泥的力度和速度也需进一步推敲,以从各个环节预防骨水泥渗漏的发生。
综上所述,骨水泥强化椎弓根螺钉技术可有效实现脊柱肿瘤合并邻近椎节骨质量不佳患者接受病灶切除术后脊柱的稳定性,是一种安全性较高并且行之有效的内固定方式。本组病例局部疼痛缓解、脊髓神经功能恢复及脊柱稳定性良好,无椎弓根螺钉位置不良、断裂等内固定并发症。而该内固定方法成功操作的关键之处在于获得合理的骨水泥弥散分布方式。
[1] Zadnik PL, Goodwin CR, Karami KJ, et al. Outcomes following surgical intervention for impending and gross instability caused by multiple myeloma in the spinal column. J Neurosurg Spine,2015, 22(3):301-309.
[2] Perrin RG, Laxton AW. Metastatic spine disease: epidemiology,pathophysiology, and evaluation of patients. Neurosurg Clin N Am, 2004, 15(4):365-373.
[3] Lou Z, Yang Y, Ren T, et al. Smad3 is the key to transforming growth factor-β1-induced osteoclast differentiation in giant cell tumor of bone. Med Oncol, 2013, 30(3):606.
[4] Costa-Rodrigues J, Fernandes A, Fernandes MH. Reciprocal osteoblastic and osteoclastic modulation in co-cultured MG63 osteosarcoma cells and human osteoclast precursors. J Cell Biochem, 2011, 112(12):3704-3713.
[5] Roato I, Grano M, Brunetti G, et al. Mechanisms of spontaneous osteoclastogenesis in cancer with bone involvement. FASEB J,2005, 19(2):228-230.
[6] Lehman RA Jr, Kang DG, Wagner SC. Management of osteoporosis in spine surgery. J Am Acad Orthop Surg, 2015,23(4):253-263.
[7] 郑伟, 吴娟, 杨立利, 等. 脊柱肿瘤患者流行病学及术后生存状况分析. 中国矫形外科杂志, 2011, 19(19):1649-1653.
[8] Bu BX, Wang MJ, Liu WF, et al. Short-segment posterior instrumentation combined with calcium sulfate cement vertebroplasty for thoracolumbar compression fractures:Radiographic outcomes including nonunion and other complications. Orthop Traumatol Surg Res, 2015, 101(2):227-233.
[9] Yilmaz G, Hwang S, Oto M, et al. Surgical treatment of scoliosis in osteogenesis imperfecta with cement-augmented pedicle screw instrumentation. J Spinal Disord Tech, 2014,27(3):174-180.
[10] 李军涛, 张恒伟, 郭旭辉, 等. 高糖对人乳腺癌细胞体外侵袭能力的影响. 中华医学杂志, 2013, 93(2):89-92.
[11] 罗斌, 梅锦荣, 王国荣, 等. 椎弓根螺钉骨水泥强化固定治疗腰椎退行性变的临床效果. 临床骨科杂志, 2013, 16(6):633-635.
[12] 樊仕才, 金大地, 张忠民, 等. 骨水泥强化椎弓根螺钉固定治疗老年退行性腰椎不稳的临床疗效分析. 中国脊柱脊髓杂志, 2010, 20(9):741-744.
[13] Liu S, Qi W, Zhang Y, et al. Effect of bone material properties on effective region in screw-bone model: an experimental and finite element study. Biomed Eng Online, 2014, 13(1):83.
[14] Hu MH, Wu HT, Chang MC, et al. Polymethylmethacrylate augmentation of the pedicle screw: the cement distribution in the vertebral body. Eur Spine J, 2011, 20(8):1281-1288.
[15] Shih KS, Hsu CC, Hou SM, et al. Comparison of the bending performance of solid and cannulated spinal pedicle screws using finite element analyses and biomechanical tests. Med Eng Phys, 2015, 37(9):879-884.
[16] Wang W, Wu F, Cong Z, et al. The secretion of IL-22 from mucosal NKp44+NK cells is associated with microbial translocation and virus infection in SIV/SHIV-infected Chinese macaques. J Immunol Res, 2014, 2014:387950.
[17] Folsch C, Goost H, Figiel J, et al. Correlation of pull-out strength of cement-augmented pedicle screws with CT-volumetric measurement of cement. Biomed Tech(Berl), 2012,57(6):473-480.
[18] Kerry G, Ruedinger C, Steiner HH. Cement embolism into the venous system after pedicle screw fixation: case report,literature review, and prevention tips. Orthop Rev(Pavia),2013, 5(3):e24.
[19] Sidhu GS, Kepler CK, Savage KE, et al. Neurological deficit due to cement extravasation following a vertebral augmentation procedure. J Neurosurg Spine, 2013, 19(1):61-70.
[20] Nicol JJ, Yarema MC, Jones GR, et al. Deaths from exposure to paramethoxymethamphetamine in Alberta and British Columbia, Canada: a case series. CMAJ Open, 2015, 3(1):E83-90.
[21] Yuan Q, Zhang G, Wu J, et al. Clinical evaluation of the polymethylmethacrylate-augmented thoracic and lumbar pedicle screw fixation guided by the three-dimensional navigation for the osteoporosis patients. Eur Spine J, 2015,24(5):1043-1050.
[22] Sawakami K, Yamazaki A, Ishikawa S, et al. Polymethylmethacrylate augmentation of pedicle screws increases the initial fixation in osteoporotic spine patients. J Spinal Disord Tech, 2012, 25(2):E28-35.
[23] McLain RF, McKinley TO, Yerby SA, et al. The effect of bone quality on pedicle screw loading in axial instability. A synthetic model. Spine, 1997, 22(13):1454-1460.
(本文编辑:王萌)
Effects of pedicle screw cement augmentation on spine tumor surgery
ZHONG Nan-zhe, YAN Wang-jun, WEI Hai-feng, LIU Tie-long, XIAO Jian-ru, YANG Xing-hai. Department of Orthopedic Oncology, Changzheng Hospital,Shanghai, 200003, PRC
YANG Xing-hai, Email: cnspineyang@163.com
Objective To evaluate the effectiveness and safety of cement-augmented pedicle screw fixation on spine tumor with osteoporotic adjacent vertebrae. Methods The medical records of 35 patients(22 males,13 females)with spine tumors combined with adjacent vertebral osteoporosis were retrospectively analyzed. All underwent operation and were reconstructed by cement-augmented pedicle screw fixation from December 2012 to November 2014. The mean age was(58.1 ± 8.5)years(range: 40 - 76 years). Characteristics of cement distribution,and the location of cement in the vertebrae and with screws were investigated. Results The mean follow-up time was(28.3 ± 4.6)months(range: 14 - 37 months). Scores of American spinal cord injury association(ASIA)and visual analogue scale(VAS)were all improved significantly at the last follow-up. The mean correction rate of kyphosis and scoliosis were 54.8% and 71% respectively with the average loss of angle 0.6° and 0.3° respectively. Preoperative and postoperative coronal Cobb’s angles were(6.0 ± 6.4)° and(1.5 ± 2.3)°, and preoperative and postoperative sagittal Cobb’s angles were(14.1 ± 12.8)° and(11.2 ± 8.1)°, with statistical significance. Coronal and sagittal Cobb’s angles showed no significant changes 3 months postoperatively and in the latest follow-up. No operative complications, nonunion or instrumental failure were detected during the follow-up. 73.4% of cement distributed in the anterior column and the rest 26.6% in the anterior column and the anterior part of the medial column. 95% confidential interval(CI)of the ratio between the diameter of cement distribution and screw:(1.80 - 3.14); the depth of cement distribution and screw:(64.6% - 92.2%); the volume of screw and cement distribution:(10.1% - 40.6%); the volume of cement distribution and vertebrae:(2.0% - 20.2%); the depth of cement distribution and the diameter of vertebrae:(43.3% -66.1%). Conclusions Cement-augmented pedicle screw fixation is an effective and save way to reconstruct the stability of spine after the surgery of spine tumor with osteoporotic adjacent vertebrae. This method can facilitate the relief of pain, recover of neural functions and remain the spinal stability. The key point to ensure the success lies in the appropriate cement distribution around the screw and in the vertebrae.
Cementoplasty; Pedicle screws; Bone neoplasms; Spine
10.3969/j.issn.2095-252X.2016.08.016 中图分类号:R738.1, R687.3
200003 上海,第二军医大学附属长征医院骨肿瘤科
杨兴海,Email: cnspineyang@163.com
(2016-02-13)
猜你喜欢
铁道建筑技术(2022年10期)2022-10-28
中国典型病例大全(2022年9期)2022-04-19
兵器装备工程学报(2021年12期)2022-01-11
中国中西医结合外科杂志(2020年6期)2020-12-31
中华养生保健(2020年4期)2020-11-16
中华骨与关节外科杂志(2016年6期)2016-05-17
科技资讯(2016年9期)2016-05-14
中国骨与关节杂志(2015年3期)2015-04-25
中国当代医药(2015年31期)2015-03-01
筑路机械与施工机械化(2014年3期)2014-03-01