
Challengesand opportunitiesof applying P4 medicineand traditional Chinese medicinefor cancer treatment and prevention in the21st century:A medical oncologist’sperspectives
2016-09-14 09:11EdwardLin
Traditional Medicine Research 2016年4期
Edward H.Lin
Introduction
For decades,three main pillars of cancer therapy are chemotherapy,radiation and surgery.Many of the cancer prevention and treatment researches were driven by six hallmarks of cancer elegantly summarized by Hanahan and Weinberg[1].Cancer researchers quickly realized that targeting cancer cells were not adequate and had turned their attentions to cancer genomics,immune evasion and cancer microenvironment which were added as new cancer hallmarks that will drive next generation cancer prevention and treatment clinical trials[2].Given the space limitations,we highlight achievements and pitfalls of the current colorectal cancer prevention and treatment strategies to argue for a new integrated principle-based P4 medicine and traditional Chinese medicine(TCM)guides driving next generation of global cancer prevention and treatment strategies.
5FU had been used to treat colorectal cancer for five decades.Only till recently did we witness FDA approvals of nine targeted agents for colorectal cancer treatment now endorsed by National Cancer Center Network guidelines and more of the new agents are coming[3].However,none of these new agents has ever challenged supreme position of 5-FU,or fluoropyrimidine,which remain as the backbone agent for colorectal cancer treatment.Some of the new agents even have had difficulties in global marketing thanks to asymmetric global regulatory policy on staggering cost and most importantly,lack of clinically meaningful gain in overall survival[4-7].Completion of whole human genome sequencing and cancer genome atlas provided much of the hopes as well as hypes for the so-called precision medicine initiatives and cancer moonshot program by major cancer centers in the US[8-10]and in China.
National Cancer Institute had to increase the power of the NCI Match Trial from 3,000 cancer patients to 5,000 cancer patients’trial in order to find mutations match through next generation sequencing(NGS)to the selected targeted drugs and so far about 9%of the mutations had resulted in matched drugs which may or may not lead to therapeutic benefits[11].This industrial approach makes an assumption that mutation(s)are static driver mutations and targeting these mutation(s)could lead to therapeutic benefits.Such reductionist approaches overlook the importance of dynamic genes mutations and their networks of interactions possibilities that can affect efficacies as well astoxicitiesof such interventions.
To address the fact that no one genome or mutations can be equally randomized and ever-increasing cost of reactive care with limited survival gain,Dr.Lee Hood,a founding figure of immunology,biotechnology,and systems biology foresee the integration of sophisticated biological instrumentation,the human genome,systems biology;and digital and consumer health revolution to new frontier of medicine:P4 medicine which stands for Predictive,Preventive,Personalized and Participatory medicine,contrary to today’s reactive guideline driven medical practices[12].P4 medicine did not gain much traction since it was first pitched to the medical community eight years ago when the use genomic technology has yet to prove that it can change standard of care and save lives.P4 medicinepromotesthe integration of systems medicine technology(omics),digital revolution,and consumer directed health initiatives to drive health care need.With crowd source funding,Dr.Hood and his institute for Systems Biology launched 100 pioneer study two years ago utilizing fitbit to track sleep and physical activity,whole genome sequencing,inflammation,microbiome,and metabolome,nutrition along with routine medical examination along counseling support[13].
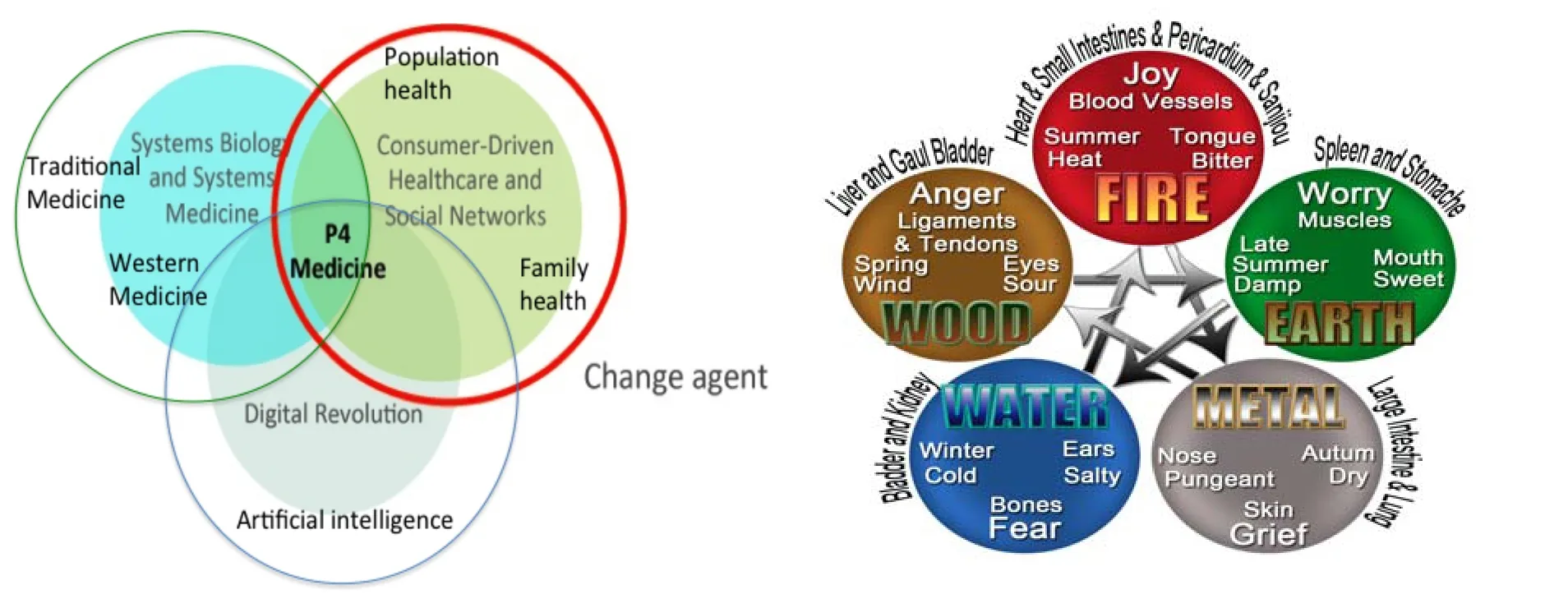
Figure 1.P4 medicine represents convergence of consumer driven health movement,Digital revolution that lead to ready access of information and systems medicine and TCM medicine as governed by five health elements which is linked to internal organsand psychosocial and emotional wellbeing.
As one of the research subjects(participatory),Iwas among afew physician volunteers who tasted first dose of P4 medicine diagnostics and interventions.Like all other“healthy”volunteers,we all harbor some form of subclinical imperfections in area of metabolism,nutrition,inflammation akin to “pre-illness” that traditional Chinese medicine(TCM)practitioners may be more adept in devising an integrated,least toxic and proven effective interventions including acupuncture,herbal remedies, and physical therapy beside application of large scale public health databases.In this review,we propose a principle based P4 medicine practice integrating best of eastern and western medicine in devising a new generation of personalized diagnostics,prevention and treatment protocols(Figure 1).
Ten Hallmarks of cancers and lessons from colorectal cancer treatment and preventions narrowsto immune angle
Cancer researchers took almost a decade shifting from six hallmarks of cancer i.e.limitless cell proliferation;Invasion;evasion of death;immortality;metastasis;and tumor angiogenesis[1]to immune evasion,and tumor microenvironment[2]driven by the clinical success of applying the checkpoint inhibitors[14-17].The level of enthusiasms for cancer immunotherapy was similar to the era when concept of targeting tumor angiogenesis was first reported[18].In fact,the first phase I clinical trial evaluating endostatin,the first anti-angiogenic agent was met with such enthusiasm that thousands more cancer patients signed up only to find that they needed to go through a lottery system to enroll in this clinical trial.In the end,endostatin was abandoned altogether for development in the US.Anti-angiogenesis therapy in cancer led to a moderate two monthsgain in overall survival ascompared to standard of care across all solid tumors and bevacizumab was first approved by the FDA which then voted later on to remove breast cancer from In the ensuing decades,researchers learned that these cancer cells are genomicallly unstable,and quickly evades various treatments through energy reprogramming as the tumors can survive in much harsher microenvironments to evade effects of chemotherapy,radiation and immune surveillance[2].This positional cancer hallmark paper will have a profound impact for this generation of cancer researchers on their treatment and prevention strategies;For space reasons,we will limit this overview to colorectal cancer prevention and treatment only.Colorectal cancer carcinogenesis takes two to three decades to evolve from precancerous polyp through a series of mutations to invasive cancer.Long-term regular use of aspirin or NSAIDs significantly reduce CRC recurrence risks[21],so will vitamin D,exercise,and control of colon cancer risk factors(obesity,diabetes,smoking and alcohol)could reduce colorectal cancer risks[22,23].Unlike aspirin,several large-scale cancer prevention trials using singular nutritional intervention i.e.Vitamin E,selenium and calcium did not demonstrate the reduction of colon polyp or cancer incidence despites strong preclinical rationales.It is interesting that aspirin is derived from plant hormone salicylic acid,which governs wide range of cellular functions including immune response,thermogenesis,respiration,fruit yield,seed germination and DNA repair immune modulation with strong parallel to cell biology found in mammalian cells where aspirin,a synthetic acetyl salicylic acid have properties in mammalian cells and functions as antipyretic,anti-inflammatory,prevention of pre-cancer and cancer,anti-platelets aggregation,ovulation,thrombosis and prevention of cardiovascular events and stroke.There are toxicitiesrelated to aspirin i.e.GI ulcer and serious CNS bleeding which is dose related(Figure 2).
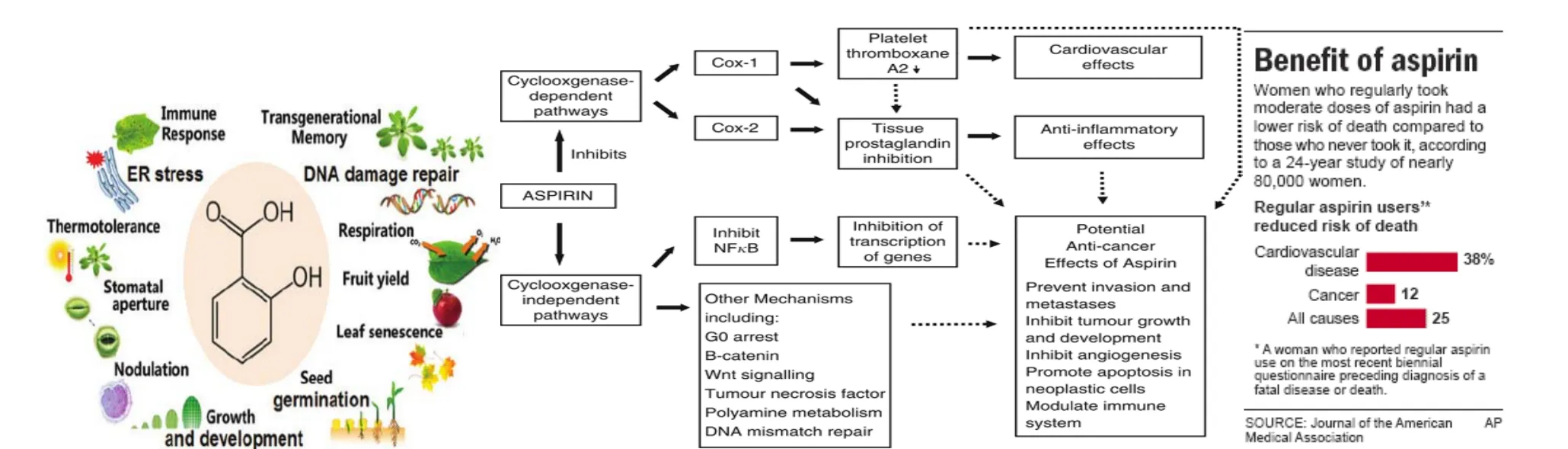
Figure 2.Versatile functions of plant hormone salicylic acid(a derivative to aspirin)in regulating plants’immune response,thermogenesis,respiration,fruit yield,seed germination and DNA repair.Striking parallel of these plant functions were found aspirin,acetyl salicylic acid which inhibits both COX-1 and COX-2 in mammalian cells and functions as antipyretic,anti-inflammatory,prevention of pre-cancer and cancer distant metastases,anti-platelets aggregation,ovulation,thrombosis and prevention of cardiovascular events and stroke.Side effects include GI ulcer,CNSbleeding diathesis,and renal injuries.
On the therapeutic front,FDA had approved nine agents for colorectal cancer,however,5-FU or fluoropyrimidine still remain as the backbone of chemotherapy alone or in combination with other chemotherapy agents or radiation[3].Most of these novel targeted agents are making incremental 1.4-2 months gain in median survival as compared to the control.As directed by the cancer hallmarks,there are three agents that target tumor DNA directly i.e.5FU irinotecan and oxaliplatin,while rests bevacizumab and aflibercept,regorafenib are targeting vascular endothelial growth factor(VEGF)pathways,and panitumumab and cetuximab,are targeting epidermal growth factor receptor(EGFR)pathways[4-7].While some of the agents e.g.bevacizumab or oxaliplatin do not have activities in the absence of 5FU,none of the agents were able to challenge the 5FU backbone.Interestingly,5FU is largely ineffective against a small subset of colorectal cancers that harbor microsatellite instability(MSI-H).In contrast,a checkpoint inhibitor,pembrolizumab resulted in promising high rate of tumor responses in MSI-H colorectal cancers as the response correlate with their high mutation loads,which may in turn have elicited inherent anti-tumor immune responses[14].Interestingly,the observed anti-tumor effects of aspirin in colorectal cancer polyp and cancer prevention is also stemming from its immune and inflammatory modulation through PD-1 and PGE2 respectively[24].Likewise,5-FU also has anti-cancer properties through its immune modulatory activitiesto bediscussed in thelater section.
Immune is the ultimate link to modern anti-cancer therapies and opportunities for TCM
Scientists from the reductionist camp also long recognized over simplifications of complex,intricately interconnected biological organism rather than a“one gene or one protein”function in a vacuum.For a complex disease like cancer,there are ever-evolving molecular mutations or targets beside some of the high profiles that have been successfully exploited for targeted therapy:CD20,[25]Her2/Neu,[26]Bcl-abl[27]c-kit[28]and Bruton tyrosine Kinase(BTK)[29].Finding similar one-on-one molecular switches or targeting for high mutation load solid tumors would not be an easy feat.Clues from the ancient Chinese remedy book had yielded the FDA approval of arsenic trioxide as the main treatment of acute promyelocytic leukemia[30].The part of the anti-tumor mechanisms with arsenic trioxide is related at least in part to the its immune toxicities in the immunosuppressive network and boost in innate immunity.More recently,checkpoint inhibitors yielded 20%durable responsesin tumorsthat are otherwise unresponsiveto the cytotoxic chemotherapy such as5FU in colorectal cancer[14].In fact,responses to checkpoint inhibitors correlate with the underlying high mutation load of the tumor.It is no surprise that only repertoires of T cells immunity can rival high mutation load of tumors.So far the toxicities with theuse checkpoint point inhibitorshave been very manageable but toxicities for combination immunotherapy began to mount especially in recent use of CAR-T[14-17].In fact,chronic arsenic trioxide are toxic to immune systems and its anti-leukemic effects were through eliminate immune suppressive component will in turn boost of immune surveillance function through a complex molecular mechanism[31].
Therefore,future global cancer treatment and prevention efforts will need to examine best strategies to mobilize one’s inactivated anti-cancer immune systems without suffering any major side effects.Immune systems and inflammation are double edge swords and harnessing their awesome healing power within for cancer treatment and prevention dealt a right card into the hands of TCM as it founding principle are all about homeostasis and five health element balance and activating one internal healing powers without major disruption of the host health ecosystems.TCM practitioners are now presented with unprecedented opportunities to work with forward thinking reductionist trained physicians,cancer immunologists and specialists,and system biologist and scientists to form a new research alliance to charter a new path of TCM principle based P4 system medicine practice,in charge of designing and implementing a series of highly personalized cancer prevention and treatment protocols that become standard of care for the ensuing decades.
In the area of pre-illness,simple cost-effective TCM disease-screening tools may help streamline the diagnostic supremacy of omics technology to be used in population disease screening.Conversely,the depth of diagnostic accuracy with omics technology will greatly boost the predictive power,which in turn can be used to validate some of TCM examination tools and practice pearls.For example,“omics”tools have made blood a window into health and disease and accurate stratification of illnesses or pre-illness for the opportunities to validate pre and post TCM intervention efficacies as they have often been criticized for not being able to ascertain efficacies in the absence of treatment randomization. One alternative to study randomization is through testing and stratification in large patient cohorts managed with different TCM interventions over long period of time and population based health outcomes were then recorded.TCM could also play ever increasing role in helping patients alleviate treatment related side effects or symptoms from these emerging immune based treatment.Some of the randomized trials had clearly validated the role of acupuncture in relieving cancer or cancer treatment related fatigue[32].Convergence of patient-activated social networks,big data and their analytics,and systems medicine diagnostic tools will provide adequate power to modernize,standardize and quantify the impact of personalized TCM treatment approaches versus reactive interventions.Physicians are also patients and engaging a stronger patient and physicians alliance will build greater trust,spread of digital health for greater information sharing and care process improvement.Past physicians giants all had experimented medicines on themselves before they prescribed to others.One hundred Persons Pioneers Project is a comprehensive scientific wellness including whole genomics,microbiome,immune,metabolome nutrition along with routine laboratory examination,sleep and activity monitoring.While the study was not directed by physicians but designed to collect data on scientific wellness.As discussed previously,virtually all “healthy”participants have some form of subclinical illness varying from nutrition,inflammation,to metabolism [13].P4 medicine especially in the area of pre-illness represents the holy grail of medicine and was recognized as superior form of medicine dating back 4,000 years ago(Nei Jing or Internal Wisdom).Ancient TCM practitioners were rewarded for preventing diseases,and punished severely for missing the disease,forcing TCM practitioners to treat pre-ailment in the absence of today’s laboratory and diagnostic tools for thousands of years.High profile media exposure of cupping for Michael Phelps in 2016 Olympic in Rio,dawn of cancer immunotherapy,genomic revolution and scientific diagnostics of pre-illness did not occur by co-incidence and will undoubtedly reinvigorate greater entry of P4 medicine with TCM practices into mainstream medicine.There are about 28,000 licensed TCM practitioners in the US and 400,000 TCM practitioners in China,a much smaller force as compared to the western based medical practitioners.Shifting to a proactive health care from reactive one will greatly boost the need for P4 medicine/TCM practitioners in the future.Collectively,we must then begin to test,interpret,upgrade and validate many of these long-held TCM tenets and principles,create and disseminate functional and system medicine curriculums to medical educators who can then bring back these new knowledge to next generation of physicians.TCM needs a universal scientifically interchangeable vocabulary to help implement future integrated research protocols on cancer treatment and prevention and reporting of disease outcomes per Good Clinical Practice Standard(GCP).For example,TCM long recognizes that cancer occurs as a result of energy imbalance in the blood particularly excessive or prolonged stress over long-term exposure to toxic chemicals in the form of pollutants in the air or water,toxins in food,and various drugs way before introduction of industrial alcohol and cigarettes production.TCM also believesthat all toxic substances ingested are first processed in the digestive system.If toxins begin to build up and accumulate in the digestive systems and will lead to “stagnant chi”leading to carcinogenesis.A stagnant Chi in the modern medicine would indicate disrupted homeostasis in metabolism,immune surveillance,host inflammation,and neural hormonal regulation and there are simple Chinese vocabularies for each of the disrupted Chi recorded in the ancient TCM guidebook.Emergence of gut microbiome as one of the key driver for immune systems and disease representsa new tools for P4 medicine to partner with TCM practitioner to learn and test balance in host inflammation,immunes surveillanceand psychosocial health.
For long time,stress and psycho-immunology is a new emerging field[32].However,five elementary principles of TCM also recognize such important psychosocial link to the immune systems and define its links to internal organs and emotions centuries ago(Figure 1).Depressions are quite common in cancer patients especially in those with pancreatic cancer[34].One of my favorite patients Melanie who had advanced pancreatic cancer is now a 10-year cancer free survivor.One of the key factors driving her survival may be in part due to our ever-positive psychosocial interactions in this wonderful ten-year doctor-patient journey. Cancer prevention and treatment that integrate depth of psychosocial interventions would for sure yield most impactful outcomes and author urges more in-depth testing and implementation of five healthy elements to tackle psychosocial aspectsof healing process.
Simplified “Seed and Soil” theory in cancer prevention and treatment?
Ten cancer hallmarkscan besummed up in a“seed and soil”theory proposed by Paget decades ago[35].A small proportion of the cancer stem cells and its tumor microenvironment are responsible for cancer progression and death[36,37].Seed and soil theory has its simple element of truth when certain cancer traits were categorized into ten hallmarks:limitlesscell proliferation and cell immortality(stemness),invasion metastasis and angiogenesis(epithelial mesenchymal transition seed-soil interface),and evasion of cell death through metabolism reprogramming,and immune destruction(soil)[38].When one examine the seed and in soil in terms of five health elements(fire,vitality,energy oxygen),metal(immune shield and dormancy),wood (roots)earth (nutrient stroma)and water(nutrient,stroma)and these five elements are interconnected to internal organs as well as psychosocial aspect of one health(Figure1).
A deeper understanding seed and soil theory and its ultimate to link to five basic health elements lead us to implement ADAPT(activating cancer stem cells from dormancy and potentiate targeting)strategy for patients with metastatic colorectal cancer using two agents capecitabine and celecoxib which had more than doubled median overall survival to 78.5 months from 33 months)in patients with metastatic colorectal cancer also likely derived from reactivation of the immunesurveillancemechanism[39].
Celecoxib is a designer drug targeting only COX-2 while sparing COX-1 for management of inflammation.Like aspirin,celecoxib can also prevent colorectal polyp in sporadic cases[40]as well as in patient with familial adenomatosis polyposis(FAP)in which patients suffered to have hundred of polyp during teenage years thanks to a dominant mutations in the APC genes[41].This colon polyp prevention strategy led to uncovering of the cardiovascular toxicities related to the agent which can be predicted by examining five-health element(fire,angiogenesis or heart)which acts upstream of metal element(i.e.immune systems).Celecoxib like aspirin mediate cancer prevention through PGE2 and PD-1 pathway in the tumor microenvironment [24]. Following five-health element principles (Figure 1), P4 physicians and TCM practitioners can design and implement next generation personalized colorectal cancer prevention studies stratifying against known colorectal cancer risk factors (personal history,diabetes, inactivity, alcohol and smoking) in conjunction with genomic prediction tools and population based TCM screening and intervention tools against no personalized interventions.Combining the power of reductionist approaches,and systems principles of “seed and soil”and five elements may yield pleasant surprises in cancer prevention and treatment in thefuture.
Opportunities and Challenges of P4 medicine and TCM
We are living in an exciting era where power of immunotherapy,system medicine tools,and modern TCM tools and strategy and scientific wellness have now finally converged and is poised to transform future of cancer prevention and treatment.From the business perspective,this new health care network will be more integrative,cross disciplinary,and has in-depth knowhow of P4 systems medicine and TCM departing from the mainstream medicine disciplinethat continues to be one-on-one encounter to addressed reactively to a know ailment or illness.Time is ripe to devise a new generation TCM based Framingham style personalized cancer prevention program ideally assisted by artificial intelligence programming that can assimilate literatures cancer immunology,predictive diagnostics,and TCM intervention tools leading to industrialization of treatment standard that be duplicated despite the genetic and phenotypic diversities of the health care consumers and heterogeneities of physicians and TCM workforce[42].
Transformation of medicine will not occur overnight as stakeholders in the established medical systems have been entrenched in these reactive medical systems for decades.Two major challenges to achieving P4 medicine--technical and societal barriers--and the societal barriers will prove the most challenging.How do we bring patients,physicians and members of the health-care community into alignment with the enormous opportunities of P4 medicine?In part,this will be done by the creation of new types of strategic partnerships--between patients,large clinical centers, consortia of clinical centers and patient-advocate groups.For some clinical trials it will be necessary to recruit very large numbers of patients--and one powerful approach to this challenge is the crowd-sourced recruitment of patients by bringing large clinical centers together with patient-advocategroups.
We are in a historical moment to bring “omics”technology for early pre-illness and pre-cancer detection and intervention.We will need challenge and revise and improve and validate the previously established TCM principles through the use “omics”technology and knowledge from stem cellsbiology and cancer immunology.Many legitimate questionsremain:1).Will interventions of these actionable items improve health and quality of life and ultimately longevity?2).Can nutrition or none drug intervention be impactful for the long-term health careoutcomes?3)How do we approach certain genetic or enzymatic deficiencies 4)What are the best intervals for repeated laboratory testing and medical checkups?5).Will be people having information overload and created unnecessary fear when tested for their genomes and microbiome?6).How do we get more physicians to embrace the proactive living instead?7)Can this be used to prevent and diagnose deadliest disease like cancer or heart disease or Alzheimer disease?We believe that P4 medicine armed with diagnostic tools and best of TCM will be able to transform the medicine landscape especially in the area of pre-illnesses intervention.We propose to form a P4 medicine alliance combining the best of western medicine and TCM to zeroing in on pre-illness or disease risk factors for effective intervention.In the colorectal cancer risk factors,there are known genetic predisposition familial adenoma polyposis(FAP)and hereditary none polyposis syndrome(HNPCC)in a subset of individuals with family history but majority of the patients at risks are those with associated risk factors includes diabetes,obesity,inactivity,excessive alcohol,smoking,poor dietary habit and consumption of smoke products,raceand poor socioeconomic status.Human as well as animal kingdom all desire for longevity free of illnesses or suffering.Animal kingdom does it by natural selection and by ensuring that best genes and behavioral trait are passed to the next generation Mankind has greater freedom and luxury to indulge in many of our good and risky behaviors ranging from consuming “bad” versus healthy food products to cigarette or alcohol consumption that ultimately threaten our health on many different dimensions.
In summary,population based deafness screening program by Capitalbio in China had already reached a 1 million children milestone.This population based genetic screening program will eliminate iatrogenic deafness in children akin to the successful various vaccines program that had eliminated many of the deadly viruses such as smallpox or polio,hepatitis B.For cancer prevention,however,best strategies are to implement a individual initiated family based cancer prevention plans ideally starting in early age and through his or her adulthood.This would include a guided dietary and exercise program and life-long good behavior modifications.A team effort from Dr.Daniel Amen and reverend Rick Warren were able to help 30,000 Saddleback members collectively shedding~226,000 kg for in six-month with no medical intervention.With the alarming cancer epidemics in China,we will need to build a trans-disciplinary healthcare team to execute strategies that can go beyond the Saddleback success and turn physicians and TCM physicians to future pioneers in this consumers oriented health care movement,leading themselves and their families to a better wellness and health path of life time.AI that stored all relevant scientific data in an easily retrievable virtual health cloud[38]can produce real time actionable health solutions and plans for individuals and families continuously.The day that health conscious consumers will be shifting en mass to this innovative home-based health and wellness solutions from the current reactive health caremodel isupon usbefore weknow it.
Reference
1.Hanahan D,Weinberg RA.The hallmarks of cancer.Cell 2000,100(1):57-70.
2.Hanahan D,Weinberg RA.Hallmarks of cancer:thenext generation.Cell 2011,144(5):646-674.
3. Benson AB 3rd,Venook AP,Bekaii-Saab T,et al.Colon cancer,version 3.2014.JNatl Compr Canc Netw 2014,12(7):1028-1059.
4.Grothey A,Van Cutsem E,Sobrero A,et al.Regorafenib monotherapy for previously treated metastatic colorectal cancer(CORRECT):an international, multicentre, randomised,placebo-controlled,phase 3 trial.Lancet 2013,381(9863):303-312.
5.Van Cutsem E,Tabernero J,Lakomy R,et al.Addition of aflibercept to fluorouracil,leucovorin,and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen.J Clin Oncol 2012,30(28):3499-3506.
6.Fuchs CS,Tomasek J,Yong CJ,et al.Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma(REGARD):an international,randomised, multicentre, placebo-controlled,phase3 trial.Lancet 2014,383(9911):31-39.
7.Bach PB.Ramucirumab for Colon Cancer and the Problem of Rising Prices Independent of Benefits.Oncologist 2015,20(9):983-984.
8.Venter JC.Genome-sequencing anniversary.The human genome at 10:successes and challenges.Science2011,331(6017):546-547.
9.Venter JC,Adams MD,Sutton GG,et al.Shotgun sequencing of the human genome.Science 1998,280(5369):1540-1542.
10.Cancer Genome Atlas Research N,Weinstein JN,Collisson EA,et al.The Cancer Genome Atlas Pan-Cancer analysis project.Nat Genet 2013,45(10):1113-1120.
11.McNeil C.NCI-MATCH launch highlights new trial design in precision-medicine era.J Natl Cancer Inst 2015,107(7):pii:djv193.
12.Hood L.A personal journey of discovery:developing technology and changing biology.Annu Rev Anal Chem(Palo Alto Calif)2008,1:1-43.
13.Gibbs,Wayt W.Medicine gets up close and personal.Nature2014,506(7487):144-145.
14.Le DT,Uram JN,Wang H,et al.PD-1 Blockade in Tumors with Mismatch-Repair Deficiency.N Engl JMed 2015,372(26):2509-2520.
15.Wolchok JD,Kluger H,Callahan MK,et al.Nivolumab plus ipilimumab in advanced melanoma.N Engl JMed 2013,369(2):122-133.
16.Bordon Y.Immunotherapy:Checkpoint parley.Nat Rev Cancer 2015,15(1):3.
17.Pardoll DM.The blockade of immune checkpoints in cancer immunotherapy.Nat Rev Cancer 2012,12(4):252-264.
18.O'Reilly MS,Boehm T,Shing Y,et al.Endostatin:an endogenous inhibitor of angiogenesis and tumor growth.Cell 1997,88(2):277-285.
19.Hurwitz H,Fehrenbacher L,Novotny W,et al.Bevacizumab plus irinotecan,fluorouracil,and leucovorin for metastatic colorectal cancer.N Engl JMed 2004,350(23):2335-2342.
20.Chen HX.Expanding the clinical development of bevacizumab.Oncologist 2004,9 Suppl 1:27-35.
21.Fink SP,Yamauchi M,Nishihara R,et al.Aspirin and the risk of colorectal cancer in relation to the expression of 15-hydroxyprostaglandin dehydrogenase(HPGD).Sci Transl Med 2014,6(233):233re2.
22.Gross MD.Vitamin D and calcium in the prevention of prostate and colon cancer:new approaches for the identification of needs.J Nutr 2005,135(2):326-331.
23.McGowan EL,Prapavessis H,Campbell N,et al.The effect of a multifaceted efficacy intervention on exercise behavior in relatives of colon cancer patients.Int JBehav Med 2012,19(4):550-562.
24.Zelenav S,Van der Veen AG,Bottcher JP et al.Cyclooxygnease dependent tumor growth through evasion of immunity. Cell 2015, 162(6):1257-1270.
25.Coiffier B, Lepage E, Brieer J. CHOP chemotherapy plus rituximab compared with CHOPalone in elderly patients with diffuse large B cell lymphoma N Engl J Med 2002,346(4):235-242.
26.Piccart-Gebhart MJ,Procter M,Leyland-Jones B et al.Trastuzumab after adjuvant chemotherapy in HER-positive breast cancer N Engl J Med 2005,353(16):1659-1672.
27.O’Brien SG,Guilhot F,Larson RA et al.Imatinib compared with interferon and low dose cytarabine for newly diagnosed chronic phase chronic myeloid leukemia.N Engl J Med 2003,348(11):994-1004.
28.Demetri GD,von Mehren M,Blanke CD,et al.Efficay and safety of imatinib mesylate in advanced gastrointestinal stroma tumors.N Engl J Med 2002,347(7):472-480.
29.Wang ML,Rule S,Martin Pet al.Targeting BTK with ibrutinib in relapsed or refractory mantle cell lymphoma.N Engl JMed 2013,369(6):507-516.
30.Soignet SL,Maslak P,Wang ZG,et al.Complete remission after treatment of acute promyelocytic leukemia with arsenic trioxide.N Engl JMed 1998,339(19):1341-1348.
31.Yang XW,Wang P,Liu JQ et al.Oncogene Coordinated regulation of the immunoproteasome subunits by PML/RARalpha and PU.1 in acute promyelocytic leukemia2014 33(21):2700-2708.
32.Price S,Lewith G,Thomas K.Acupuncture care for breast cancer patients during chemotherapy:a feasibility study.Integr Cancer Ther 2006,5(4):308-314.
33.Nelson EL,Wenzel LB,Osann K et al.Stress,immunity,and cervical cancer:biobehavioral outcomes of a randomized clinical trial Clin Cancer Res2008,14(7):2111-2118.
34.Mayr M,Schmid RM,Pancreatic cancer and depression:myth and truth.BMCCancer 2010,10:569.
35.Fidler IJ.The pathogenesis of cancer metastasis:the'seed and soil'hypothesis revisited.Nat Rev Cancer 2003,3(6):453-458.
36.Reya T,Morrison SJ,Clarke MF,et al:Stem cells,cancer,and cancer stem cells.Nature 2001,414(6859):105-111
37.Eaves CJ.Cancer stem cells:Here,there,everywhere?Nature2008,456(7222):581-582.
38.Trumpp A,Wiestler OD.Mechanisms of Disease:cancer stem cells--targeting the evil twin.Nat Clin Pract Oncol 2008,5(6):337-347.
39.Lin EH,Kim E,Wang L et al.ADAPT therapy vs capecitabine bevacizumab in stage IV colorectal cancer:Pooled 10-year survival experience and a phase II study update.JClin Oncol 2016,34(15):e15046.
40.Bertagnolli MM,Eagle CJ,Zauber AG et al.Celecoxib for prevention of sporadic colorectal adenoma N Engl JMed 2006,355(9):873-884.
41.Steinbach G,Lynch PM,Phillips RK,et al.The effects of celecoxib,a cyclooxygenase-2 inhibitor in familial adenomatous polyposis.N Engl J Med 2000,342(26):1946-1952.
42.Kiefer B. [Watson, medicalized artificial intelligence].Rev Med Suisse 2015,11(492):2044.
 Traditional Medicine Research2016年4期
Traditional Medicine Research2016年4期
- Traditional Medicine Research的其它文章
- A new idea of electro-acupuncturetreatment for peripheral facial paralysis and thenerve-endocrinehypothesis
- Effectsof acupuncture treatment for irritablebowel syndrome:a systematic review and meta-analysis
- A Literature Review of the Acupoint Plaster Therapy for Asthma in Summer
- A prospective,randomized controlled trial of sanguisorba oil in the treatment of tamoxifen-related vaginitisin breast cancer patients
- Pharmacokinetic study of dl-tetrahydropalmatinepatchesby UPLC–MS/MSin rabbits
- Dynamic changesof circulating Th1 and Th17 cellsin psoriasispatients:a report of 3 cases treated by Chineseherbal medicine