
Dynamic changesof circulating Th1 and Th17 cellsin psoriasispatients:a report of 3 cases treated by Chineseherbal medicine
2016-09-14 09:11YaJunLiTaoZhouJingZhangYanBaiCangZhangPingLi
Traditional Medicine Research 2016年4期
Ya-Jun Li,Tao Zhou,Jing Zhang,Yan Bai,Cang Zhang*,Ping Li
1Beijing Hospital of Traditional Chinese Medicineaffiliated to Capital Medical University,100010,Beijing,China.2Beijing Institute of Traditional Chinese Medicine,100010,Beijing,China.3Beijing Key Laboratory of Clinic and Basic Research with Traditional Chinese Medicineon Psoriasis,100010,Beijing,China.
Introduction
Psoriasis is a common chronic recurrent inflammatory disease of the skin.Recent studies have demonstrated that immunological process,especially T-helper(Th)cell mediated immune-responses,involved in the development of the disease[1].Besides the red,scaly and itchy patches,Th1 and Th17 cells were found increased in the peripheral blood of psoriasis patients[2].Cytokines secreted from these cells may attack the skin and result in psoriatic lesions.In addition to systemic therapies,many biologics,such as Infliximab,Ustekinumab and Secukinumab,have been developed to target the specific inflammatory cascade to cure plaque psoriasis[3-5].However,there are potential unidentified side effects[6-8],and their using is limited due to high cost in many countries,including China.
In China,it is conventional to treat psoriasis with Chinese herbal medicine.According to the theory of Traditional Chinese Medicine (TCM),psoriasis vulgaris can be differentiated into various types based on lesions,symptoms and progress of the disease.Different formulas would be applied to different types.Liang-Xue-Jie-Du decoction(LXJD)is one of the classic formulas for blood-heat type,which is characterized by fresh,red papula and thicken-plaques covered with white squamae,and the plaques are in progressing and keep bursting.How LXJD play itsrole isstill a mystery.
In this report,we present 3 patients who were differentiated as blood-heat type and were treated with LXJD decoction alone.It was found that circulating Th1 and Th17 cells were lowered along with skin recovering.One of the cases showed that LXJD decoction overcame infection induced Th1 and Th17 increasing and ameliorated psoriatic lesions.
Case presentation
Patient 1
This 28-year-old male has suffered from psoriasis vulgaris for 9 years without systemic treatment.It recurred two months ago with increasing papula all over the body surface.The patient felt itchy dramatically for one month.Ketoconazole Lotion was applied on the scalp,and QinBai ointment,a Chinese herbal preparation,was applied on plaques.The topical treatment could remove dandruff and relief itch,but could not stop progressing.He had no family history of psoriasis,and no remarkablehistory of medication.
On his first visit,numerous well marginated red,thick and scaly plaques were seen on the scalp,torso,legs and arms,accompanied by sore throat and bad temper.The squamae on plaques were dry and in white color.There was no scar,exudation,erosion or blister on theskin.
The patient was treated with LXJD decoction,which was composed of Smilacis Glabrae Rhizoma,Sophorae Flos,Rehmanniae Radix, Arnebiae Radix,Paeoniae Radix Rubra,Dictamni Cortex and Bistort Rhizome (Table 1). During the treatment,CD3+CD8-IFNr+and CD3+CD4+IL17A+cell subsets(antibodies were purchased from BD Biosciences,California,USA),which represent Th1 and Th17 lymphocytes in circulating T-helper cells,respectively,were detected with fluorescent activated cell sorting(FACS,by BD FACSVerse).After 2 weeks administration of LXJD,impairment on the patient’s scalp started diminishing,rush color of his face started calming down,but the plaque area on torso did not change(Fig.1a,week2).The patient complained of distracting itching on the abdomen and legs.Thus,the herbal decoction made from Broussonetia Papeyrifera Folium(Chu Tao Ye)was applied topically.We thought that the decreaseof Th1 and Th17 subsets(Fig.2c,points of week 2)might predict a good outcome.As expected,at week 4,the thickness of plaques reduced clearly,the redness of plaque became much lighter than before(Fig.1a,week 4),and itching relieved gradually.PASI lowered from 28.8 to 5,achieving 75%improvement(PASI75)by day 30.
To be noted,at week 6,the patient complained of a light sore on histhroat.On examination,the throat was red again due to congestion.Meanwhile,FACS examination showed a rebound of Th1 and Th17 cells in peripheral blood but theplaquewas kept fading.The reduction of PASI achieved 90%(PASI90)from baseline at the end of week 8,regardless of high Th1 and Th17 level(Fig.2c).
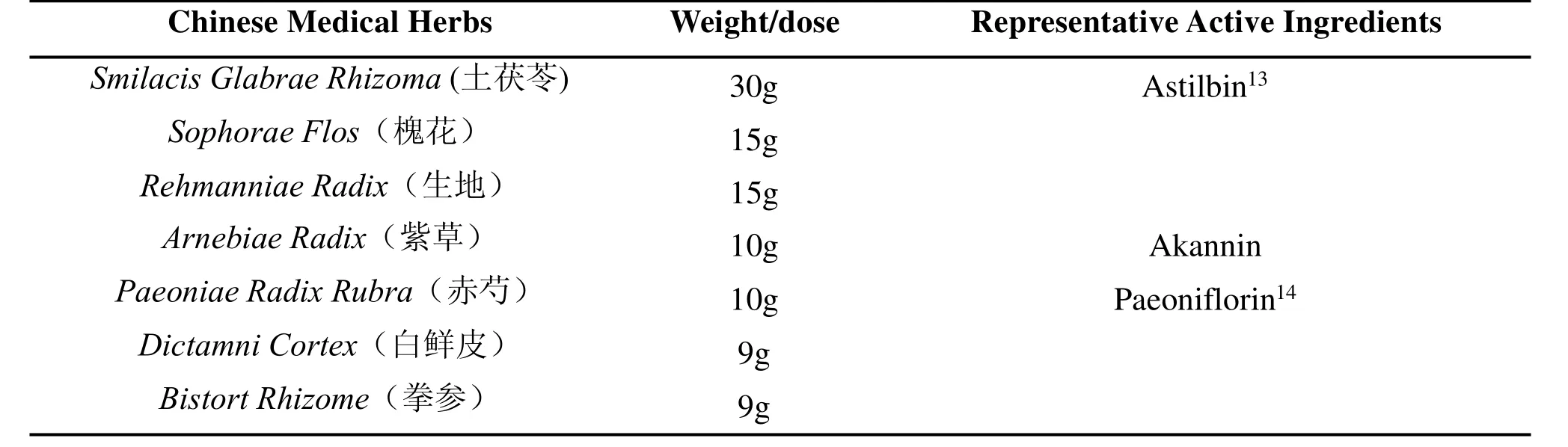
Table1.Prescription of Liang-Xue-Jie-Du Decoction.
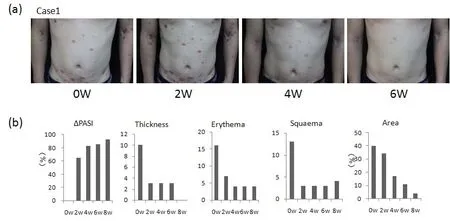
Figure 1 Representative pictures of psoriasis plaques.(a)Pictures of patient 1,which showing the plaques on the chest and abdomen.(b)Evaluation of the lesions of patient 1 on PASI changes,plaque thickness,erythema,squaema and affected area.
Patient 2 and Patient 3
Patient 2 is a 25-year-old male who has a 10-year history of psoriasis vulgaris.The lesions enlarged year by year.It relapsed half a month ago dueto spicy foods.He was not treated systemically before,except for topical application of a TCM ointment.
Patient 3 is a 28-year-old male with a 3-year history of psoriasis vulgaris.It relapsed two months ago after staying up late for months.Calcipotriol Ointment had been topically used occasionally without system treatment.
Similar to patient 1,both of them were suffered by growing plaques,which were distributed on their scalps,torsos,legs and arms.The lesions were red,thick,covered with squamae,and itchy.Both of them were accompanied with dysphoria and sore throat.The baselines of PASIwere 23.5 and 14.6 for patient 2 and 3(Fig.2d,2e),respectively.They were diagnosed as blood-heat psoriasis,and treated with LXJD decoction as well.The lower of Th1 and Th17 cells was found 6 weeks later(Fig.2d,2e).The reduction of PASI,one is over 70%,the other achieved 90%(PASI90)after 8 weeks treatment.None of them showed detectable side effectson their kidneys,liversand hearts.
Discussion
According to TCM,psoriasis can be differentiated into distinct types.The efficiency of various TCM treatment has been proven by random blind case reports[9].LXJD is one of the classic formulae for blood-heat type,and is recommended by the Guidelines of Psoriasis Treatment in TCM[10].Here,we present 3 cases of blood-heat type who visited the clinic at the same day.All of them had no serious complications,apart from sore throats and dysphoria.By 8-weeks treatment of LXJD decoction,two of them were cured (PASI90),and one achieved 70%improvement in PASI(Fig.2c,2d,2e).
Psoriasis is a T cell associated inflammatory skin disease.Th1 and Th17 cells were found increased not only in the skin but also in the blood of psoriasis patients[2,11].Meanwhile,it was reported that Th1 helper cells were increased in blood-heat psoriasis[12].In this report,we found that with the treatment of LXJD,both Th1 and Th17 cells were lowered in parallel,accompanied with amelioration of psoriatic plaques(Fig.2c,2d,2e).The percentage of these cells got lowered clearly at week 2 for patient 1,at week 6 for patient 2 and 3.Though distinct individuals responded to treatment differently,LXJD might play its role partially through regulating the differentiation of T-helper cells.Several components of the herbs in LXJD have been tested in psoriasis-like mice models.For instances,Astilbin and Paeoniflorin,the active component of Smilacis Glabrae Rhizoma and Paeoniae Radix Rubra,respectively,could inhibit Th17 differentiation via inhibiting Stat3 phosphorylation[13,14].In patient,LXJD might regulate the differentiation of T lymphocytes through similar mechanisms.
To be noted,the increase of Th1 and Th17 cell subsets is not specific to psoriasis.They could also be found increased in various inflammatory diseases[15].In this report,patient 1 caught an upper respiratory infection characterized by sore throat at week 6.His Th1 and Th17 rebounded to a high level again.To our surprise,with ongoing LXJD therapy,the additional inflammatory circumstance did not disturb the recovery from skin lesions.The PASI level achieved 90%improvement at week 8.Recruitment of immune cells to the skin is important for the development of psoriatic lesions.It is possible that LXJD protected the skin by inhibiting the recruitment of circulating immune cellsto plaques.Meanwhile,LXJD is a 7-herb formula with hundreds of unidentified active components.Thus,in addition to immune system,it is also possible that LXJD functions on other psoriasis associated tissues,such as the vascular and the skin,to curethe lesionsinduced by inflammatory cytokines.
This is the first report observing TCM treatment in psoriasis vulgaris with FACSmonitoring of circulating lymphocytes every two weeks.It showed that circulating Th1 and Th17 cells lowered following with the fading of psoriatic lesions.In clinic,individuals may present various symptoms,respond to treatment differently.Thus,clinical trials with more cases included,together with delicate designed experiments would be necessary to set up the relationship between LXJD and T cell response in psoriasis.Understanding the role by which LXJD played may benefit the patientsin thelong run.
Acknowledgments
The work is supported by Beijing Natural Science Foundation(No.715205).
Consents
Written informed consents were obtained from the patients.
Competing interests
The authors declared that they have no competing interests.
1.Nestle FO,Kaplan DH,et al.Psoriasis.N Engl J Med 2009,361(5):496–509.
2.Kagami S,Rizzo HL,Lee JJ,et al.Circulating Th17,Th22,and Th1 cells are increased in psoriasis.J Invest Dermatol 2010,130(5):1373-1383.
3.Brezinski EA,Armstrong AW.Off-label biologic regimens in psoriasis:a systematic review of efficacy and safety of dose escalation,reduction,and interrupted biologic therapy.PLoS One 2012,7(4):e33486.
4.Langley RG,Elewski BE,Lebwohl M,et al.ERASURE Study Group;FIXTURE Study Group.Secukinumab in plaque psoriasis--results of two phase 3 trials.N Engl JMed 2014,371(4):326-338.
5.Sofen H,Smith S,Matheson RT,et al.Guselkumab (an IL-23-specific mAb)demonstrates clinical and molecular response in patients with moderate-to-severe psoriasis.J Allergy Clin Immunol 2014,133(4):1032-1040.
6.Onel KB,Onel K.Anti–Tumor Necrosis Factor Therapy and Cancer Risk in Patients With Autoimmune Disorders.Arthritis Care Res 2010,62(7):1024–1028
7.Mansouri B, Patel M, Menter A.Biological therapies for psoriasis.Expert Opin Biol Ther 2013,13(12):1715-1730.
8.Souza A de,Ali-Shaw T,Reddy SM,et al.Inflammatory arthritis following ustekinumab treatment for psoriasis:a report of two cases.Br J Dermatol 2013,168(1):210–212.
9.Zhou DM,Chen WW,Wang P,et al.Clinical Therapeutic Observation of 200 Cases of Psoriasis Vulgaris Treated with Standardized Syndrome Differentiation.WJITWM 2010,5(7):593-596.
10.Dermatologist Branch of China Association of Chinese Medicine, Expert Committee of Dermatology of Beijing Association of Chinese Medicine,Expert Committee of Dermatology Venereology of Beijing Association of Integrative Medicine.The evidence based clinical guidelines of psoriasis vulgaris in TCM treatment(2013 Edition).Journal of Traditional Chinese Medicine 2014,55:76-82.
11.Benham H,Norris P,Goodall J,et al.Th17 and Th22 cells in psoriatic arthritis and psoriasis.Arthritis Res Ther 2013,15(5):R136.
12.Chen J,Cao XX,Xu R,et al.Research on different expressions of peripheral blood Th1/Th2 cells in psoriasis patients of blood heat syndrome and of blood stasis syndrome.CJITWM 2014,34(1):46-50.
13.Di TT,Ruan ZT,Zhao JX,et al.Astilbin inhibits Th17 cell differentiation and ameliorates imiquimod-induced psoriasis-like skin lesions in BALB/c mice via Jak3/Stat3 signaling pathway.Int Immunopharmacol 2016,32:32-38.
14.Zhao JX,Di TT,Wang Y,et al.Paeoniflorin inhibits imiquimod-induced psoriasis in mice by regulating Th17 cell response and cytokine secretion.Eur JPharmacol 2016,772:131-143.
15.Liu Y,Zeng M,Liu Z.Th17 response and its regulation in inflammatory upper airway diseases.Clin Exp Allergy 2015,45(3):602-612.
 Traditional Medicine Research2016年4期
Traditional Medicine Research2016年4期
- Traditional Medicine Research的其它文章
- Challengesand opportunitiesof applying P4 medicineand traditional Chinese medicinefor cancer treatment and prevention in the21st century:A medical oncologist’sperspectives
- A new idea of electro-acupuncturetreatment for peripheral facial paralysis and thenerve-endocrinehypothesis
- Effectsof acupuncture treatment for irritablebowel syndrome:a systematic review and meta-analysis
- A Literature Review of the Acupoint Plaster Therapy for Asthma in Summer
- A prospective,randomized controlled trial of sanguisorba oil in the treatment of tamoxifen-related vaginitisin breast cancer patients
- Pharmacokinetic study of dl-tetrahydropalmatinepatchesby UPLC–MS/MSin rabbits