
前交叉韧带前嵴与前交叉韧带下止点关系的核磁影像学研究
2017-05-03 12:04崔国庆刘玉雷蒋艳芳敖英芳
中国运动医学杂志 2017年4期
崔国庆 刘玉雷 蒋艳芳 敖英芳
北京大学第三医院运动医学研究所,北京市运动医学关节伤病重点实验室(北京 100191)
前交叉韧带前嵴与前交叉韧带下止点关系的核磁影像学研究
崔国庆 刘玉雷 蒋艳芳 敖英芳
北京大学第三医院运动医学研究所,北京市运动医学关节伤病重点实验室(北京 100191)
目的:测量观察研究正常人膝关节核磁(magnetic resonance imaging,MRI)上前交叉韧带(an⁃terior cruciate ligament,ACL)前嵴与ACL胫骨止点的位置及其相对关系,探讨ACL前嵴对于重建ACL手术下止点定位和术后影像学评估的临床意义。方法:对2015年1月至2016年12月间因膝关节不适就诊于北医三院门诊的年轻患者(18~40岁,平均25.1岁)的膝关节MRI进行回顾性测量观察研究。患者均在同一台核磁共振仪器膝关节完全伸直位时做检查。从Pets终端调出图像,分析未见明显异常的MRI影像共计100例。测量和计算矢状面上胫骨前后径、ACL前嵴距离、ACL前缘距离、ACL后缘距离和ACL中心点距离。结果:矢状面上ACL中心点位于整个胫骨平台的百分比为42.21%±4.3%(28.43%~50.94%),有58例小于43.3%。ACL前嵴距离为13.61±2.17mm(8.03~18.65mm),占整个胫骨平台的百分比为26.80%±3.89%(17.74%~33.94%)。ACL前嵴距离与ACL前缘距离高度相关(P<0.001,ICC= 0.954)。ACL前嵴与ACL前缘的间距为0.56±0.68mm(-0.28~2.71mm)。如果以ACL前嵴定位骨道前缘,假设移植物直径8mm,55度定位,前缘与ACL前嵴间距0.5mm,则有96例患者重建ACL的移植物中心点在原ACL胫骨止点中心点之前。结论:在MRI矢状面上,ACL前嵴与ACL前缘的位置相距平均0.56mm,ACL前嵴的位置与ACL胫骨止点前缘具有高度相关性。本研究提示,ACL重建术中,在矢状面上按照ACL前嵴定位的前缘定位法定位胫骨骨道可以比传统的中心点定位法获得更好的靠前定位的结果。
膝关节;前交叉韧带;核磁;胫骨;前交叉韧带前嵴
1 前言
目前,前交叉韧带(anterior cruciate ligament,ACL)重建手术广泛开展,已取得了显著的成效,但是ACL重建仍有7%~10%的失败率[1]。有研究表明,胫骨骨道的位置差是导致手术失败最主要的原因之一,且它对稳定性的贡献比股骨骨道更重要[2,3]。然而目前定位于ACL胫骨止点足迹的中心点还是靠前的位置尚存在争议,而且指导术中定位的理想的解剖标志尚未形成共识。
传统上,在重建ACL的胫骨骨道选择上,通常以移植物在胫骨中心点作为术中的定位依据,同时术后以是否骨道中心点位于正常ACL中心点平均值为评价重建骨道优劣的标准。Staubli和Rauschning对5例尸体膝关节进行矢状面冰冻切片,测算出ACL胫骨止点中心点距离胫骨前缘占整个胫骨平台比例平均为43.3%(24.6%~62.1%)[4]。此后,此比例在临床上术中定位和术后评价ACL胫骨骨道时被广泛引用。同时有学者在研究髁间窝与ACL移植物位置关系时提倡将ACL胫骨骨道向后移以避免髁间窝撞击[5-8]。然而,近年来,越来越多的学者认为理想的胫骨骨道是在不与髁间窝顶发生撞击的前提下尽量位于ACL足印区的靠前部分,从而可以获得更好的膝关节稳定性和关节活动度[9-13]。这一观点从尸体实验和临床实践中均得到证实。为了获得靠前而又不撞击的胫骨骨道,术中以骨道前缘定位更为准确可靠。然而,目前的文献中,很少有学者在术中定位时按照以移植物前缘为标准的定位方法[11,12,14]。
近年来,随着越来越多的学者注意到Parson’s knob(帕森氏结节)对于指导ACL重建中胫骨骨道定位的作用,关于Parson’s knob的大体与镜下解剖、影像学评估和指导手术重建的临床意义已逐渐成为研究热点[14-18]。在解剖研究中,多位学者认为ACL胫骨止点的前界就是Parson’s knob,或者叫“L型嵴”[14]、前嵴(ante⁃rior ridge)[15]、“鸭掌样”或“C”型结构[16,17]。在ACL重建术中,有学者以前嵴作为ACL胫骨骨道的前缘定位并获得很好的临床效果[11,14]。在影像学研究中,有学者在3D CT检查中发现96.6%的患者可以观察到前嵴。然而,由于是CT检查,他们无法测量前嵴与ACL胫骨止点的位置关系[15]。尽管核磁(magnetic resonance imag⁃ing,MRI)能够测量ACL前嵴与ACL胫骨止点的位置关系,但相关文献仅有1篇。2014年,Ichiba以Parsons’Knob作为ACL胫骨止点窝的前界,在100例膝关节MRI矢状面上测量了ACL窝前缘距离胫骨前缘11.4±1.6mm。然而,他们也没有进一步测量Parsons’Knob与ACL胫骨止点前缘的位置关系[18]。
本研究目的是通过测量正常人膝关节MRI上ACL前嵴和ACL胫骨止点的位置及其相对关系,探讨ACL前嵴对于指导手术重建时下止点定位和术后影像学评估的临床意义。
2 对象和方法
对2015年1月至 2016年12月间因膝关节不适就诊于北京大学第三医院门诊的年轻患者(男性45例,女性43例,18~40岁,平均25.1岁)的膝关节MRI进行回顾性研究。患者均在同一台核磁共振机器(超导磁共振Optima MR430s 1.5T四肢骨关节检查专用成像系统,GE公司,美国)上做检查。在这个设备中患者膝关节必须完全伸直,位置变化较小,便于测量。从Pets终端调出图像,分析未见明显异常的MRI影像共计100例。标准MRI的层面包括T1和T2相的矢状位、T2相的冠状位和横断位。冠状面定义为沿着股骨髁后界切面做的平行于大腿纵轴的平面。矢状面定义为垂直于冠状面的平面。入组标准:(1)MRI影像清晰;(2)膝关节完全伸直;(3)膝关节未见明显异常;(4)能够找到最大程度包括ACL胫骨止点的矢状面和冠状面进行分析。排除标准:(1)ACL病变;(2)明显骨关节炎;(3)既往做过膝关节手术;(4)膝关节无法伸直;(5)拍片不清晰;(6)膝关节左右位置不正。本文研究者在不同时间和另一位经过影像科医生培训的医师分别用Pets软件按照同样的方法随机选取其中20例膝关节MRI影像进行观察和测量,以评估测量方法的观察者本身和观察者间的可靠性。
在MRI矢状面上观察ACL前嵴的形态,并参考Pećina[19]在X线上对ACL前嵴的分型,将其按形态分为4型,见图1。1型:明显隆起(上坡下坡均明显);2型:上坡稍隆起且下坡明显,或者上坡明显且下坡不明显;3型:上坡和下坡均不明显但可辨认;4型:基本平坦不易辨认。
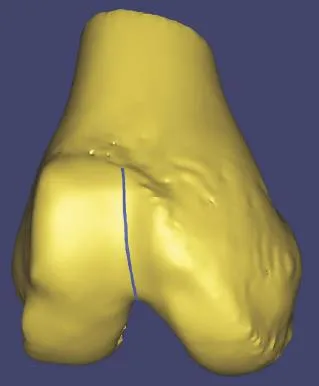
图1 ACL前嵴形态分型
根据Staubli和Rauschning法[4]观察和测量如下指标。以后交叉韧带胫骨止点后缘为后界,通过此点做胫骨纵轴垂线,该垂线与胫骨前皮质交界点为前界,测量胫骨前后界的距离即为胫骨前后径。以胫骨前界为起点做胫骨前后径的垂线,分别测量各个解剖标志距此线的垂直距离,分别命名为ACL前嵴距离、ACL前缘距离和ACL后缘距离。ACL中心点距离即是计算ACL前缘距离与ACL后缘距离的平均值。测量方法见图2。
根据每例患者实际ACL中心点距离与本组患者ACL中心点距离平均值的差值分为3组。分别是差值≤3mm组,差值大于3≤5mm组和差值大于5mm组,计算各组病例数。
评价观察者本身和观察者间的可靠性用相关系数(intraclass correlation coefficient,ICC)度量[20]。ICC值大小的解释:小于0.75,一致性较差;0.75~0.9,中度一致性;大于0.9,高度一致性[21]。用相关性分析方法研究ACL前嵴与ACL胫骨中心点、前缘和内缘的关系,并计算相关系数。因方差不齐,故用非参数检验(Kruskal-Wallis检验)方法分析ACL前缘与前嵴间距对ACL中心点的影响因素。计量资料用均数±标准差表示。所有统计分析均采用Windows 7下的SPSS21.0进行。P<0.05被认为差异有统计学意义。
3 结果
3.1 观察者本身对各指标测量的可靠性
矢状面上,胫骨前后径:高度一致(ICC=0.994);ACL前嵴距离:中度一致(ICC=0.879);ACL前缘距离:中度一致(ICC=0.85);ACL后缘距离:中度一致(ICC= 0.846);ACL中心点距离:高度一致(ICC=0.907)。
3.2 ACL前嵴的形态学分型
1型40例,2型34例,3型23例,前三型合计97例,占97%。4型3例,占3%。
这种情况下,西王方面紧急行动,首先是用摒弃前嫌请来了落跑外援劳森,然后用“小詹姆斯”桑普森临时替换莫泰;针对本土球员战斗力不强的弱点,吴庆龙请来了自己的老搭档、辽宁老乡接君……
3.3 各径线的距离
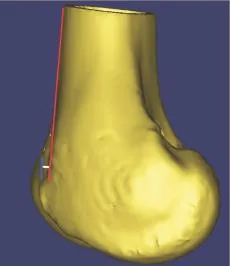
图2 各径线测量方法
矢状面上各径线的测量结果见表1。ACL前嵴距离为13.61±2.17mm(8.03~18.65mm),ACL前缘距离为14.17±2.25mm(8.03~19.77mm)。ACL中心点距离为21.43±2.54mm,占整个胫骨平台的百分比为42.21%±4.3%(28.43%~50.94%)。ACL前嵴与ACL中心点间距为8.85±0.79mm(7.63~9.51mm)。
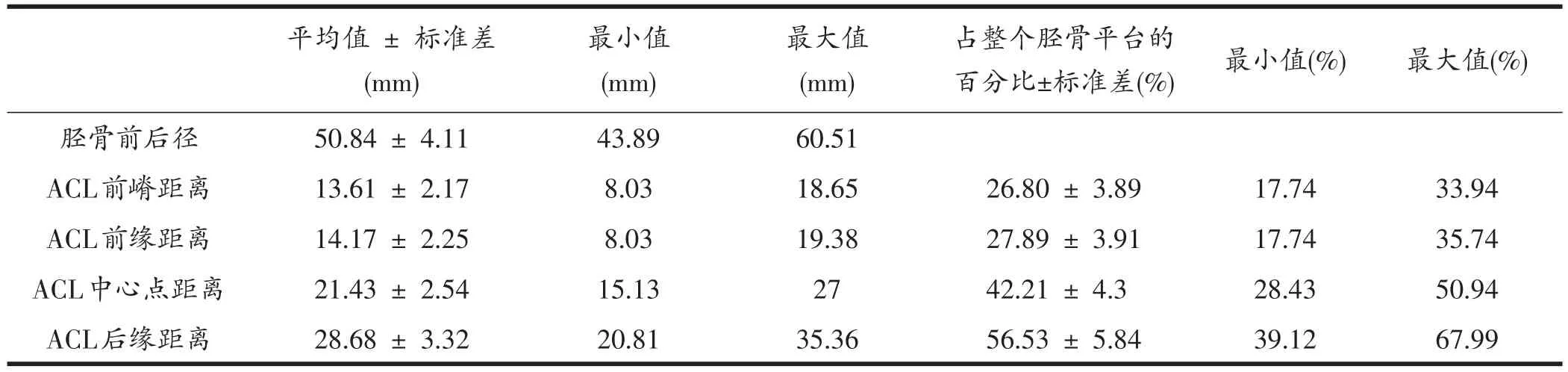
表1 MRI矢状面上各径线的测量结果
3.4 ACL前嵴与ACL胫骨止点的相关性
矢状面上,ACL前嵴距离与ACL中心点距离中度相关(P<0.001,ICC=0.838),ACL前嵴距离与ACL前缘距离高度相关(P<0.001,ICC=0.954)。
3.5 ACL前嵴与ACL前缘间距对ACL中心点的影响
矢状面上,ACL前嵴与ACL前缘的间距为0.56± 0.68mm,范围-0.28~2.71mm。小于等于2mm者96例,小于3mm者100例。将ACL前嵴与ACL前缘间距按0mm、0~1mm、>1mm分为3组,各组分别有50、23和27例。因方差不齐,故用非参数检验(Kruskal-Wallis检验),结果显示,各组胫骨前缘距ACL中心点的距离差异不显著(P=0.067),认为ACL前嵴与ACL前缘的间距与胫骨前缘距ACL中心点的距离无关。
3.6 胫骨前缘与ACL中心点不同距离的病例分布
矢状面上,本组患者胫骨前缘与ACL中心点平均距离为21.43±2.54mm。我们计算每例患者实际ACL中心点距离与本组所有患者ACL中心点距离平均值的差值,发现差值≤3mm(18.43mm≤ACL中心点距离≤24.43mm)的有78例,差值>3且≤5mm(16.43mm≤ACL中心点距离≤18.43mm或者24.43mm≤ACL中心点距离≤26.43mm)的有16例,差值>5mm(ACL中心点距离<16.43或者ACL中心点距离>26.43)的有6例。见图3。
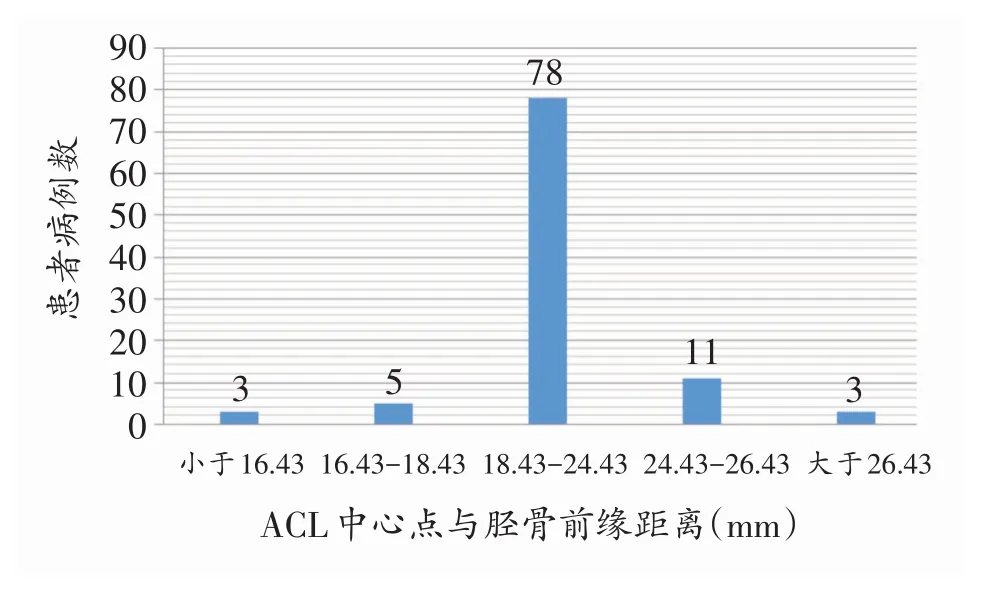
图3 胫骨前缘与ACL中心点不同距离的病例分布
假定骨道与平台夹角是55°,移植物直径(直角边)为8mm,则矢状面骨道内口纵径9.77mm(假设排除冠状位角度对骨道出口径线偏移的影响)[22]。如图4。
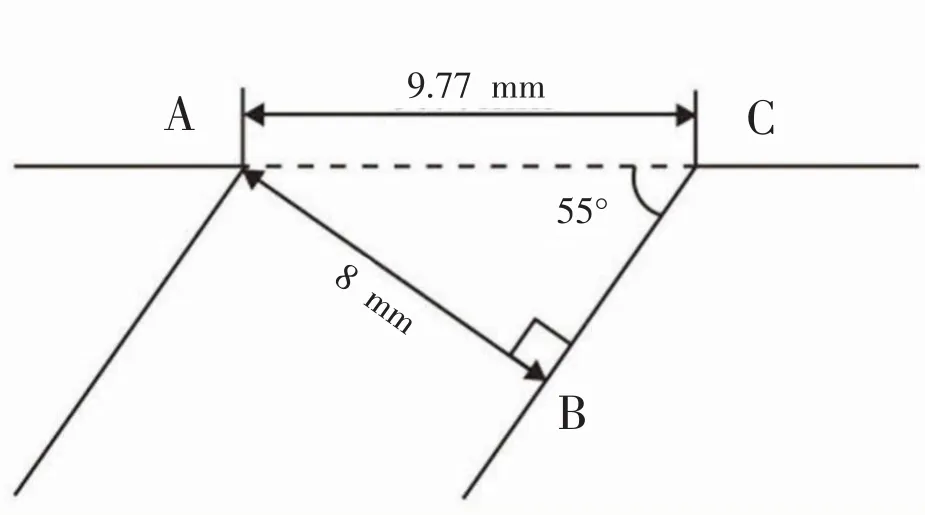
图4 根据移植物大小计算骨道内口直径示意图
如果以矢状面43.3%为最佳中心点定位,拟定中心点与实测中心点比较,仅有42例拟定中心点在实测中心点前方,而58例均在实测中心点后侧。计算拟定韧带前缘位置与实测ACL前棘的间距,其中:小于等于2mm者28例,小于3mm者49例,大于3mm而小于等于5mm者28例,大于5mm者25例。
如果按照以ACL前嵴定位的前缘定位法定位,我们推荐临床上定位ACL移植物前缘与ACL前嵴的间距为0.5mm(鉴于矢状面上,ACL前嵴与ACL前缘间距平均值为0.56mm),则重建韧带的中心点为ACL前嵴往后5.4mm(0.5+9.77÷2mm)。经计算,本组患者重建ACL的移植物中心点在原ACL胫骨止点中心点之前的病例为96例,在原ACL胫骨止点中心点之后的病例为4例。
比较两种定位方法获得骨道位置位于ACL中心点之前的病例数,发现差异有统计学意义(χ2=68.16,P<0.001)。
4 讨论
目前,关于指导术中胫骨骨道定位的理想的解剖标志尚未形成共识,且定位于ACL胫骨止点足迹的中心点还是靠前的位置尚存在争议。近年来,越来越多的学者对Parson’s knob指导ACL重建中胫骨骨道定位的解剖和临床意义进行研究,然而却没有在MRI上研究其与正常ACL胫骨止点位置关系的报道。本研究通过测量正常人膝关节MRI上ACL前嵴和ACL胫骨止点的位置及其相对关系,为探讨ACL前嵴的临床意义奠定了影像学基础。
本MRI观察研究获得的数据与既往的解剖和影像学研究基本相符。在对胫骨前后径的测量方面,有解剖研究报道51±5.8mm[4]和52±5mm[23],MRI研究报道49.2±3.7mm[18]。我们在MRI上测量的胫骨前后径为50.84±4.11mm,与文献中的解剖研究相符,且测量的观察者自身和观察者间的一致性均高度相关(ICC均大于0.95)。在矢状面ACL前缘、中心点和后缘的距离测量方面,有解剖研究报道ACL前缘、中心点和后缘与胫骨平台前缘的距离分别为14±4.2mm、21±2.6mm和29±4.1mm[4],其中前内束和后外束中心点分别距胫骨平台软骨前缘13±2.3mm和14.7±2.8mm[24]。MRI研究的文献中,ACL前缘、中心点和后缘距胫骨前缘的平均距离分别为13.4~15.2mm,21.4~23.7mm和29.4~32.1mm。我们的研究发现:ACL前缘、中心点和后缘与胫骨平台前缘的距离分别为14.17±2.25mm、21.43±2.54mm 和28.68± 3.32mm,与既往报道类似。关于ACL中心点占胫骨前后径的百分比的测量,虽然各个解剖研究报道不一,但大多数参考Staubli和Rauschning1994年对5例尸体测量计算得出的43.3%的结果[4]。在MRI研究中,Schef⁃fel测量了138例健康人,得到的比例为44.1%[26]。我们的MRI测量结果为42.21%,较文献略小,这可能与人种或者样本差异有关。
关于ACL前嵴的MRI测量的文献很少,目前仅见1篇报道。2014年,Ichiba以Parsons’Knob作为ACL胫骨止点窝的前界,在100例膝关节MRI矢状面上测量了ACL窝前缘距离胫骨前缘11.4±1.6mm[18]。我们的MRI研究中,100例患者ACL前嵴距离为13.61± 2.17mm,比文献报道略大(2mm)。分析原因可能与测量方法有关。虽然同样采用Staubli和Rauschning方法,但Ichiba的图示中显示:他们对胫骨前后径测量时没有包括皮质部分,这可能导致测量的距离偏小[14,18]。
传统上,在重建ACL的胫骨骨道定位方法上,通常以Staubli和Rauschning提出的43.3%在矢状面上作为骨道中心点进行定位,同时术后以此比例作为评价骨道优劣的标准[4]。然而,近年来,越来越多的学者认为理想的胫骨骨道是在不与髁间窝顶发生撞击的前提下尽量位于ACL足印区的靠前部分,从而可以获得更好的膝关节稳定性和关节活动度。这一观点从尸体实验和临床实践中均得到证实。Voos[9]和Bedi[10]的生物力学研究发现,胫骨骨道置于胫骨足印偏前的位置可以改善Lachman和轴移试验时胫骨前移和旋转稳定性。Ohsawa[11]、Hatayama[12]和PaDua[13]对单束或者双束ACL重建术后进行2年随访,发现胫骨骨道位置靠前的患者术后IKDC、Lysholm和KT1000结果更好。本MRI研究发现:正常ACL胫骨止点中心点占整个胫骨平台比例范围从28.43%到50.94%,其中有58例小于43.3%。这提示,如果按照传统的43.3%的比例重建胫骨骨道,有58%的患者在原ACL足印区中心点的靠后位置,可能会不利于术后的前后和旋转稳定性。
本研究还发现,如果以我们测量的ACL胫骨止点中心点平均比例42.21%为定位标准,仅有78%的患者ACL中心点距离平均值小于3mm,而分别有16%和6%的患者距离为3~5mm和大于5mm。虽然文献中多位作者以术后KT1000膝关节松弛程度大于3mm或5mm作为诊断ACL断裂[27,28]或者ACL重建术后失败[8,29-31]的标准,但目前还没有文献报道术后松弛程度与胫骨骨道偏离距离的具体对应关系[32,33]。尽管如此,本研究结果至少表明,如果按照传统的中心点定位法定位胫骨骨道,会有22%的患者重建的胫骨骨道偏离原ACL解剖中心点超过3mm(靠前8例,靠后14例)。
本研究提示,按照ACL前嵴定位的前缘定位法是一种可靠的胫骨骨道定位方法。首先,在矢状面上,ACL前嵴距离与ACL前缘距离和中心点距离相关性很好(ICC分别为0.954和0.838),这提示ACL前嵴与正常ACL的相对距离相对恒定,能够反映正常ACL的止点变异程度。Sullivan[36]和Provencher[37]指出,基于人群的解剖数据平均百分比定位ACL胫骨骨道仅供参考,而不能代表某一患者个体。我们的MRI研究提示,ACL前嵴可以作为反映个体变异的解剖标志。
其次,矢状面上,ACL前嵴与ACL前缘间距平均为0.56mm,最大值2.71mm,且其变化对ACL中心点的影响无统计学意义。也就是说,ACL前嵴与ACL前缘间距较小,其个体的变异程度不会影响ACL移植物的位置。这在临床上很有意义,如果按照ACL前嵴定位移植物前缘,因为其相对距离很小,术中相对好定位,而且定位的前后相对不容易影响骨道位置的成败。这增加了手术中胫骨骨道定位的稳定性,能够明显提高骨道定位定点的正确率。
最后,根据ACL前嵴与ACL前缘间距的平均值0.56mm,我们建议临床上以ACL前嵴向后0.5mm进行移植物前缘定位。为了模拟临床实际情况,我们假定移植物直径为8mm,以55°在拟定位点做8mm骨道。考虑到倾斜角度,我们参考文献[22]根据移植物粗细和角度精确计算了骨道内口的实际直径为9.77mm。如果按照ACL前嵴定位的前缘定位法计算移植物中心点与原正常ACL中心点的相对位置关系,则发现有96例患者的移植物中心点在原正常ACL中心点靠前的位置。而如果按照传统的43.3%中心点定位法,仅有42例在原正常ACL中心点靠前的位置,两者差别显著。因此,理论上按照ACL前嵴定位的前缘定位法可以使重建的胫骨骨道在原ACL足印的位置上比传统的43.3%中心点定位法更加靠前。
本研究的不足之处是:(1)MRI只能选择最大程度的包括ACL胫骨止点,由于是二维平面,不能全面立体地评估ACL止点和ACL前嵴,可能存在一定误差。(2)我们采用1.5T核磁设备以保证膝关节伸直。如果在3.0T核磁下伸直膝关节检查,更能提高影像的精确度,进一步提高测量的可靠性。(3)MRI观察兼顾评估韧带和骨结构,但对于骨性结构的分辨率不如CT,今后需要技术的进步,更好地同时评估两种结构。
5 小结
本研究首次在MRI上测量了正常人ACL胫骨止点和ACL前嵴的位置关系,发现ACL前嵴与ACL前缘的距离平均为0.56mm,ACL前嵴的位置与ACL胫骨止点前缘具有高度相关性。研究提示,ACL重建术中,按照ACL前嵴定位的前缘定位法定位胫骨骨道可以比传统的中心点定位法获得更好的靠前定位的结果。
[1] Grossman MG,ElAttrache NS,Shields CL,et al.Revision anterior cruciate ligament reconstruction:three-to nineyear follow-up.Arthroscopy 2005;21:418-423.
[2] Mall NA,Matava MJ,Wright RW,et al.Relation between anterior cruciate ligament graft obliquity and knee laxity in elite athletes at the National Football League com⁃bine.Arthroscopy,2012,28(8):1104-1113.
[3] Matava MJ,Arciero RA,Baumgarten KM,et al.Multirater agreement of the causes of anterior cruciate ligament re⁃construction failure:a radiographic and video analysis of the MARS cohort.Am J Sports Med,2015,43(2):310-319.
[4] Staubli HU,Rauschning W.Tibial attachment area of the anterior cruciate ligament in the extended knee position:anatomy and cryosections in vitro complemented by mag⁃netic resonance arthrography in vivo.Knee Surg Sports Traumatol Arthrosc,1994,2:138-146.
[5] Amis AA,Jakob RP.Anterior cruciate ligament graft po⁃sitioning,tensioning and twisting.Knee Surg Sports Trau⁃matol Arthrosc,1998,6 Suppl 1:S2-12.
[6] Howell SM,Clark JA.Tibial tunnel placement in anterior cruciate ligament reconstructions and graft impingement. Clin Orthop Relat Res,1992,283:187-195.
[7] Romano VM,Graf BK,Keene JS,et al.Anterior cruciate ligament reconstruction.The effect of tibial tunnel place⁃ment on range of motion.Am J Sports Med,1993,21(3):415-418.
[8] Almekinders LC,Chiavetta JB,Clarke JP.Radiograph⁃ic evaluation of anterior cruciate ligament graft failure with special reference to tibial tunnelplacement.Arthrosco⁃py,1998,14(2):206-211.
[9] Voos JE,Musahl V,Maak TG,et al.Comparison of tun⁃nel positions in single-bundle anterior cruciate ligament reconstructions using computer navigation.Knee Surg Sports Traumatol Arthrosc,2010,18:1282-1289.
[10]Bedi A,Maak T,Musahl V,et al.Effect of tibial tunnel position on stability of the knee after anterior cruciate ligament reconstruction:Is the tibial tunnel position most important?Am J Sports Med,2011,39:366-373.
[11]Ohsawa T,Kimura M,Hagiwara K,et al.Clinical and sec⁃ond-look arthroscopic study comparing 2 tibialland⁃marks for tunnel insertions during double-bundle ACL re⁃construction with a minimum 2-year follow-up.Am J Sports Med,2012,40:2479-2486.
[12]Hatayama K,Terauchi M,Saito K,et al.The impor⁃tance of tibial tunnel placement in anatomic double-bun⁃dle anterior cruciate ligament reconstruction. Arthrosco⁃py,2013,29(6):1072-1078.
[13]Padua R,Alviti F,Venosa M.The influence of graft placement on clinical outcomein anterior cruciate liga⁃ment reconstruction.Joints,2016,4(1):12-16.
[14]Shimodaira H,Tensho K,Akaoka Y.Remnant-Preserv⁃ing Tibial Tunnel Positioning Using Anatomic Landmarks in Double-Bundle Anterior Cruciate Ligament Reconstruc⁃tion.Arthroscopy,2016,32(9):1822-1830.
[15]Tensho K,Shimodaira H,Aoki T,et al.Bony landmarks of the anterior cruciate ligament tibial footprint:A de⁃tailed analysis comparing 3-dimensional computed tomog⁃raphy images to visual and histological evaluations.Am J Sports Med,2014,42:1433-1440.
[16]Siebold R,Schuhmacher P,Fernandez F,et al.Flat mid⁃substanceoftheanteriorcruciateligamentwith tibial“C”-shaped insertion site.Knee Surg Sports Traumatol Arthrosc,2015,23:3136-3142.
[17]Oka S,Schuhmacher P,Brehmer A,et al.Histological analysis of the tibial anterior cruciate ligament insertion Knee Surg Sports Traumatol Arthrosc,2016,24(3):747-753.
[18]Ichiba A,Kido H,Tokuyama F.Sagittal view of the tib⁃ial attachment of the anterior cruciate ligament on mag⁃netic resonance imaging and the relationship between an⁃terior cruciate ligament size and the physical characteris⁃tics of patients.J Orthop Sci,2014,19(1):97-103.
[19]Pećina M,Bajok I,Pećina HI.Tuberculum intercondy⁃lare tibiae tertium as a predictive factor for anterior cru⁃ciate ligament injury.Am J Sports Med,2001,29(6):709-711.
[20]Shrout PE,Fleiss JL.Intraclass correlations:uses in as⁃sessing rater reliability.PsycholBull,1979,86:420-428.
[21]Portney LG,WatkinsMP.Foundationsofclinicalre⁃search applications to practice.2nd ed.Upper Saddle Riv⁃er,NJ:Prentice Hall Health;2000.
[22]Kopf S,Martin DE,Tashman S,et al.Effect of tibial drill angles on bone tunnel aperture during anterior cruci⁃ate ligament reconstruction.J Bone Joint Surg Am,2010,92:871-881.
[23]Edwards A,BullAM,AmisAA. The attachments of the anteromedial and posterolateral fibre bundles of the anterior cruciate ligament:Part 1:tibial attachment.Knee Surg Sports Traumatol Arthrosc,2007,15(12):1414-1421.
[24]Takahashi M,Doi M,Abe M,et al.Anatomical study of the femoral and tibial insertions of the anteromedial and posterolateralbundlesofhuman anteriorcruciate liga⁃ment.Am J Sports Med,2006,34:787-792.
[25]Frank RM,Seroyer ST,Lewis PB,et al.MRI analysis of tibialposition oftheanteriorcruciateligament.Knee Surg Sports Traumatol Arthrosc,2010,18(11):1607-1611.
[26]Scheffel PT,Henninger HB,Burks RT.Relationship of the intercondylar roof and the tibial footprint of the ACL:implications for ACLreconstruction.Am J Sports Med,2013,41(2):396-401.
[27]DanielDM,Stone ML,Sachs R,etal.Instrument⁃ ed measurement of anterior knee laxity in patients with acute anterior cruciate ligament disruption.Am J Sports Med,1985,13(6):401-407.
[28]Bach BR Jr,Warren RF,Flynn WM,et al.Arthromet⁃ric evaluation of knees that have a torn anterior cruciate ligament.J Bone Joint Surg Am,1990,72(9):1299-1306.
[29]Rijke AM,Perrin DH,Goitz HT,et al.Instrumented ar⁃thrometry for diagnosing partial versus complete anterior cruciate ligament tears.Am J Sports Med,1994,22(2):294-298.
[30]Pinczewski LA,Salmon LJ,Jackson WF,et Radiological al.landmarks for placement of the tunnels in single-bundle reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br,2008,90(2):172-179.
[31]程聪,任士友,陈鹏,等.内侧半月板损伤对前交叉韧带重建后失效的诊断意义.中国修复重建外科杂志,2016,30(5):558-561.
[32]Waltz RA,Solomon DJ,Provencher MT.A radiographic assessment of failed anterior cruciate ligament reconstruc⁃tion:can magnetic resonance imaging predict graft integri⁃ty?Am J Sports Med,2014,42:1652-1660.
[33]Schillhammer CK,Reid JB 3rd,Rister J,et al.Arthros⁃copy up to date:anterior cruciate ligament anatomy.Ar⁃throscopy,2016,32(1):209-212.
[34]Politzer G,Pick J:Uber einen Rontgenologischwichtigen Knochenbefund am medialen Knodylus der Tibia.Fortsch Geb Rontgenstrahlen Nuklearmed,1937,56:649-653.
[35]Berg EE:Parsons’knob(tuberculum intercondylare terti⁃um):A guide to tibial anterior cruciate ligament insertion. Clin Orthop,1993,292:229-231.
[36]Sullivan JP,Cook S,Gao Y,et al.Radiographic anatomy of the native anterior cruciate ligament:a systematic re⁃view.HSS J.2015,11(2):154-165.
[37]ProvencherMT.EditorialCommentary:Anatomyofthe Anterior Cruciate Ligamentd Are We Up to Date?Arthros⁃copy,2016,32(1):213.
Research on the Relationship between the Anterior Ridge and the Tibial Attachment of the Anterior Cruciate Ligament on Magnetic Resonance Imaging
Cui Guoqing,Liu Yulei,Jiang Yanfang,Ao Yingfang
Institute of Sports Medicine,Peking University Third Hospital,Beijing Key Laboratory of Sports Injuries,Beijing 100191,China
Ao Yingfang,Email:yingfang.ao@vip.sina.com
ObjectiveTo measure and determine the position of the tibial attachment of the anterior cruciate ligament(ACL)in relation to its anterior ridge on the magnetic resonance imaging(MRI)of normal knee joints,and to explore the clinical role of the anterior ridge in guiding tunnel positioning during ACL reconstruction as well as in facilitating postoperative radiographic evaluation.MethodsThe knee MRI of one hundred young adult patients with an intact ACL and normal knee joint(mean age:25.1 years,range:18-40 years)was retrospectively reviewed.All MR images were obtained at full exten⁃sion of the knee on the same MRI machine.Using digital image software on MRI,the measurements in the sagittal view were taken,including the depth of the tibia,the distance from the anterior edge of the tibial plateau to the most anterior and posterior portions of the ACL insertion on the tibia and the ante⁃rior ridge according to Staubli and Rauschning’s method.ResultsThe center of the tibial insertion of the ACL is located between 28.43%and 50.94%of the total anterior–posterior depth of the tibia,which was less than 43.3%in 58 patients.The average distance from the anterior edge of the tibial plateau to the anterior ridge was 13.61± 2.17mm(ranging from 8.03 to 18.65mm),26.80% ± 3.89%(ranging from 17.74%to 33.94%)across the tibial plateau.There were significant positive corre⁃lations between the distance from the anterior edge of the tibial plateau to the most anterior portion of the ACL insertion and that to the anterior ridge.The distance from the most anterior portion of the ACL insertion to the anterior ridge was averaged 0.56±0.68mm(ranging from-0.28 to 2.71mm). During the ACL reconstruction,with the anterior edge of the tibial tunnel determined at posterior 0.5mm to the anterior ridge,the graft size as 8mm,and the tibial guider angle set as 55 degree,96 of the patients(96%)would have the center of the tibial tunnel located before the center of their na⁃tive ACL attachment.ConclusionsOn sagittal MR images,the location of the anterior ridge and the most anterior portion of the ACL insertion correlated well,with the average distance between them of 0.56mm.The study indicates that during ACL reconstruction,tibial tunnel drilling with the anterior edge of the ACL graft positioned at the anterior ridge can achieve a more anterior position than the traditional methods to orientate according to the center of the bone tunnel.
anterior cruciate ligament,knee joint,magnetic resonance imaging,tibia,anterior ridge of anterior cruciate ligament
2017.03.01
第1作者:崔国庆,Email:cgq3019@vip.163.com;
:敖英芳,Email:yingfang.ao@vip.sina.com
猜你喜欢
实用手外科杂志(2022年2期)2022-08-31
世界最新医学信息文摘(2021年12期)2021-06-09
计算机技术与发展(2020年8期)2020-08-12
电脑报(2020年12期)2020-06-30
民用飞机设计与研究(2020年1期)2020-05-21
中国运动医学杂志(2020年2期)2020-04-02
电脑报(2019年4期)2019-09-10
北京大学学报(医学版)(2019年3期)2019-06-18
宝藏(2019年6期)2019-01-15
南方文学(2016年4期)2016-06-12
