
Therapeutic observation of cranial suture acupuncture in treating depression
2018-06-28 09:27AiChunqi艾春启WangQinbo王钦波WangXi王熙WangYu汪宇ChenShengmei陈生梅ChenXiong陈雄
Ai Chun-qi (艾春启), Wang Qin-bo (王钦波), Wang Xi (王熙), Wang Yu (汪宇), Chen Sheng-mei (陈生梅), Chen Xiong (陈雄)
1 Department of Mental Health Center, Taihe Hospital, Hubei University of Medicine, Shiyan 442000, China
2 Department of Pharmacy, The Sixth Hospital Affiliated to Sun Yat-sen University, Guangzhou 510655, China
3 Department of Comprehensive Traditional Chinese Medicine Mental Health Center, Taihe Hospital, Hubei University of Medicine,Shiyan 442000, China
4 Department of Information Resources, Taihe Hospital, Hubei University of Medicine, Shiyan 442000, China
Depression is a common mood disorder with high relapse and disability rates, causing heavy burden to family and society[1-2]. The global burden of disease study launched by the World Health Organization(WHO) estimated that the prevalence of depression would arise to the second place among all the disabling diseases in 2020[3].
Currently, depression is treated with medication,psychotherapy and physical therapy, of which,antidepressant medication is predominantly used[4].However, in may cause adverse reactions, take longer time to produce effect and poor compliance. With regard to psychotherapy, it is difficult for patients to stick to it due to the long treatment cycle. Traditional Chinese medicine (TCM) holds that depression belongs to the scope of depression syndrome and it is mainly caused by disordered flow of qi and blood and disharmony between yin and yang, which bring about disturbed primordial spirit, eventually manifesting pessimism, low mood and irritability. Acupuncturemoxibustion has a long history of being used to treat affective disorders, and its efficacy in treatment of depression has been verified by numerous clinical studies in modern medicine. Besides, it costs less and causes fewer adverse effects.
Cranial suture acupuncture is a novel acupuncture method based on skull anatomy and TCM theory. It selects acupoints according to the surface projections of cranial sutures and thus has a definite anatomical basis.This study observed the efficacy of combining cranial suture acupuncture and paroxetine in treating depression, and the report is given as follows.
1 Clinical Materials
1.1 Diagnostic criteria
By referring to the diagnostic criteria of depression in the fifth edition ofDiagnostic and Statistical Manual of Mental Disorders(DSM-5)[5].
1.2 Inclusion criteria
Conforming to the above-mentioned diagnostic criteria of depression, with stable vital signs; disease duration ≥4 weeks but ≤1 year; age ≥15 years but≤60 years; with clear consciousness and able to comprehend the content of the adopted scale, capable of expressing and cooperating in the treatment; willing to participate in the current trial and having signed the informed consent.
1.3 Exclusion criteria
Not conforming to the aforementioned diagnostic and inclusion criteria; coupled with dangerous acts or significant mental disorders; head trauma or infected skin lesion in the topical area; coupled with fatal diseases involving heart, liver or kidney; with a history of acupuncture or paroxetine allergy; fainting during acupuncture; poor compliance.
1.4 Drop-out criteria
Those who withdrew halfway due to intolerable adverse reactions; aggravated condition during the treatment and other treatments were necessary to be adopted; unwilling to continue the treatment due to either subjective or objective reasons.
1.5 Statistical method
The SPSS version 19.0 statistical software was used.Normal distribution and homogeneity of variance were first checked. According to the results, the data all conformed to normal distribution and homogeneity of variance. The measurement data were expressed as mean ± standard deviation (x±s): the intra-group comparisons were processed by pairedt-test, and the inter-group comparisons were analyzed by independent samplet-test. The enumeration data were compared by adopting Chi-square test.P<0.05 was indicative of statistical significance.
1.6 General data
One hundred patients were recruited from the Department of Mental Health Center, Taihe Hospital,Hubei University of Medicine, between August 2016 and June 2017. This trial had been approved by the Ethics Committee of Taihe Hospital, Hubei University of Medicine, and the informed consent had been obtained from each subject.
The subjects were numbered according to their visiting sequence and then divided into either an observation group or a control group by using the random number table, with 50 cases in each group.There were no significant differences in gender, age or disease duration between the two groups (allP>0.05),indicating the comparability (Table 1).
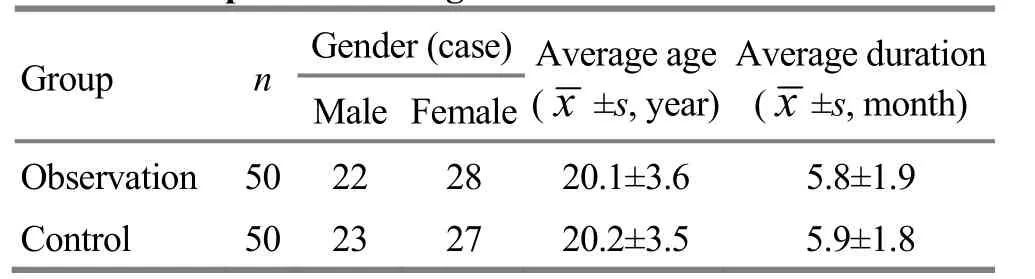
Table 1. Comparison of the general data
2 Methods
The two groups of patients were prescribed with paroxetine tablets for oral administration (lot number:H10950043, Sino-American Tianjin-Smith Kline and French Lab., Ltd., China), 20 mg each time, once per day.One-week treatment made up 1 course and the treatment successively lasted 6 courses.
During the treatment, the patients were asked to take sufficient rest, stay away from other medications, and maintain a good mood and healthy habits, as well as a regular daily living.
2.1 Observation group
In addition to paroxetine, the observation group was intervened by cranial suture acupuncture.
Relevant literatures were referred to locate the cranial suture acupoints[6].
Acupuncture at coronal suture: Yin Guan point, the midpoint of coronal suture, is taken as the top point,and the length between this point and Yintang (GV 29)is approximately 10 cm (about 5.5 cun by the individual cun measurement, L1 in Figure 1). Taking Yin Guan point as the midpoint, the coronal suture was punctured on both sides, one needle every 3-4 cm. The needles were inserted 2-3 cm by forming 18° with the coronal plane[6], and this is also the angle between the coronal suture and coronal plane (angle-α, Figure 2),(Figure 3).
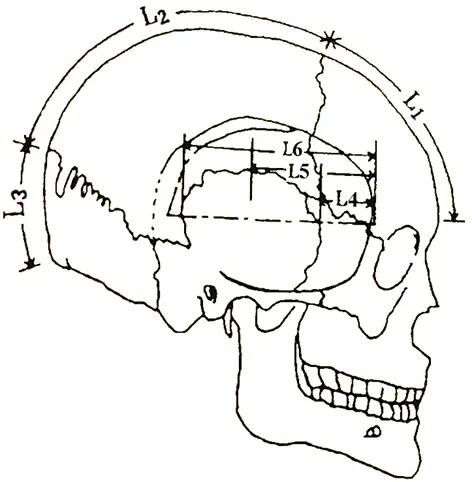
Figure 1. Lateral view of cranial suture anatomy
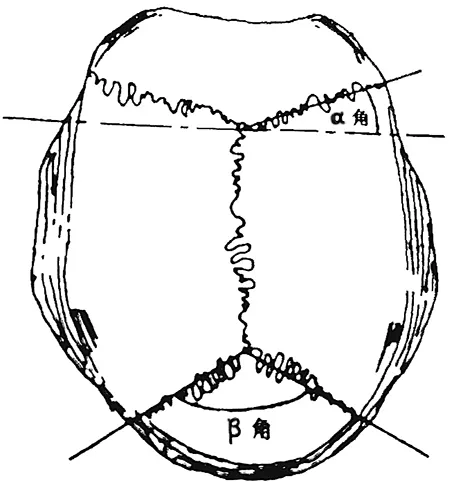
Figure 2. Vertical view of included angles of cranial sutures

Figure 3. Acupuncture at coronal suture
Acupuncture at Guan Ren point (L2 in Figure 1): Yin Guan point is taken as one end. The other end is superior to the crossing point of the Governor Vessel and the occipital protuberance, 6.5 cm away (about 3.5 cun by the individual cun measurement). The line between the two ends was punctured, one needle every 3 cm. The needles were inserted 2 cm horizontally(Figure 4).

Figure 4. Acupuncture at Guan Ren point
Acupuncture at Zhen Ren point (L3 in Figure 1): The line between the lower end of Guan Ren point and occipital protuberance was punctured, one needle every 3 cm. The needles were inserted 2 cm horizontally.(Figure 5).

Figure 5. Acupuncture at Zhen Ren point
Acupuncture at the anterior, superior and posterior zygomaticotemporal sutures (L4-L6 in Figure 1): Needle was inserted to the anterior zygomaticotemporal suture 2-3 cm vertically (L4 in Figure 1); the superior zygomaticotemporal suture was punctured by 2 cm either towards left or right horizontally (L5 in Figure 1);the posterior zygomaticotemporal suture was punctured by 2-3 cm vertically (L6 in Figure 1). When puncturing the above points, the needles were all moved between galea and periosteum until the needle tip reached the required depth (Figure 6).
Acupuncture at lambdoid suture: Two needles were respectively punctured towards left and right by 110-150°. The needles were inserted 2-3 cm along this suture between galea and periosteum (Figure 7).

Figure 6. Acupuncture at the anterior, superior and posterior zygomaticotemporal sutures

Figure 7. Acupuncture at lambdoid suture
Operation: The patient took a sitting position and exposed the head thoroughly. After sterilization by 0.2%iodine, the needles were swiftly inserted 1.0-1.3 cun by an angle of 15°, with twirling manipulation applied at 180-200 times per minute till the patient felt distending or numb. The needles were retained for 50 min and the needling manipulation was performed once every 10 min for the duration.
Adjunct acupoints based on syndrome differentiation:Guanyuan (CV 4) and Qihai (CV 6) were added for yang deficiency; Qimen (LR 14), Hegu (LI 4) and Taichong(LR 3) were added for liver depression and qi stagnation;Fenglong (ST 40) and Danzhong (CV 17) were added for phlegm and dampness blocking. Proper reinforcing or reducing manipulations were applied according to syndrome differentiation to enhance the efficacy.
Treatment course: Each session lasted 50 min, once a day for 6 weeks.

Table 2. Comparison of the clinical efficacy (case)
2.2 Control group
The control group only received Western medication treatment.
3 Observation of Therapeutic Efficacy
The patients all completed the treatment and observation, so there were no dropouts.
3.1 Observation items
Depression: The depression severity was evaluated by Hamilton depression scale-17 (HAMD-17)[7].
Safety: General examination was conducted as well as the routine blood, urine and stool tests, liver and kidney function tests and electrocardiogram (ECG).
The HAMD was observed before the treatment and respectively after 1-week, 2-week, 4-week and 6-week treatment. The safety evaluation was run before the treatment and after 6-week treatment.
3.2 Criteria of the therapeutic efficacy
Two attending physicians who were not involved in the treatment and blinded to the grouping were trained to use HAMD-17 in a consistent manner to observe the clinical efficacy.
The reduction rate of HAMD-17 score was taken to determine the clinical efficacy. The reduction rate of HAMD-17 score = (Pre-treatment score – Posttreatment score) ÷ Pre-treatment score × 100%.
Recovered: The reduction rate of HAMD-17 score≥75%.
Markedly improved: The reduction rate of HAMD-17 score ≥50% but <75%.
Improved: The reduction rate of HAMD-17 score≥25% but <50%.
Invalid: The reduction rate of HAMD-17 score <25%.
3.3 Results
3.3.1 Comparison of clinical efficacy
After the intervention, the total effective rate was 94.0% in the observation group versus 78.0% in the control group, and the between-group difference was statistically significant (χ2=8.3156,P=0.0039), (Table 2).
3.3.2 Comparison of HAMD score
Compared with the baseline score, the HAMD scores were significantly lower in both groups respectively after 1-week, 2-week, 4-week and 6-week treatment(P<0.05). The HAMD scores after 4-week and 6-week treatment in the observation group were significantly different from those in the control group (P<0.05),(Table 3).

Table 3. Comparison of the HAMD score (x±s, point)
3.3.3 Safety evaluation
During the intervention, one patient in the observation group had nausea, vomit and abdominal bloating, and another patient had dry bitter mouth and dizziness. After symptomatic treatment, the symptoms were gone. In the control group, four patients showed nausea, vomit and abdominal bloating, one patient had increased heart rate, and one patient had dry bitter mouth and dizziness. After symptomatic treatment, the symptoms were partially gone.
4 Discussion
Depression is featured by significant persistent low mood which makes a person unable to cope with the environment, often accompanied by slow reaction, loss of interest, low self-esteem, sleep disorders, and even suicidal attempt[8]. So far, it is still unclear what causes depression, but generally, depression is believed to be associated with sociopsychological and genetic factors,human biochemical changes and neuroendocrine system. For example, a study held that the development of depression should be related to the hypofunction of certain monoamine neurotransmitters such as 5-hydroxytryptamine (5-HT) receptor and norepinephrine (NE) receptor[9]. Most of the current antidepressant drugs all target 5-HT or NE, working through regulating the contents of monoamine neurotransmitters from the synaptic cleft of the brain as well as their function.
There is no such name for the disease of depression in traditional Chinese medicine (TCM). However,according to the manifestations, it can be covered by the scope of depression syndrome. TCM holds that this condition is caused by depressed or extreme emotions,or internal damage by emotions, loss of the charge of brain, and disordered qi-blood and yin-yang, which lead to depression and irritability. It majorly affects the brain,but the heart, liver and spleen are also influenced. Brain is the house of the primordial spirit and where yang energy gathers. It is also the material basis of thinking activity. Under the control of brain and via the cooperation of Zang-fu organs, human emotions are maintained normal. Any abnormal emotions should all be related to the damage to the brain or dysfunction of the brain.
The cranial suture acupuncture is based on the surface projection of the sutures and has a clear anatomical reference. Cranial sutures are made of strong fibrous tissues, where small vessels from the superior sagittal sinus pass by. Lu QL[10]has discovered that these sutures are channels linking the exterior and the interior and there distribute rich sympathetic nerve branches and complex receivers. Numerous literatures from both home and abroad have verified that acupuncture-moxibustion can produce certain efficacy in treating depression[11-14]. The sagittal suture travels along the Governor Vessel, covering many acupoints including Baihui (GV 20), Qianding (GV 21), Houding (GV 19) and Xinhui (GV 22). Therefore, it can regulate yang qi of the whole body, benefit the brain, and calm the heart and mind. The coronary and lambdoid sutures travel across the Bladder Meridian of Foot Taiyang and Gallbladder Meridian of Foot Shaoyang. The abovementioned sutures can cover most of the meridians and acupoints located on the head. Hence,cranial suture acupuncture is effective in treating emotional disorders because it can regulate and unblock the Governor Vessel, and modulate qi-blood of the whole body, subsequently restoring the balance between yin and yang. In this study, cranial suture acupuncture was adopted to harmonize qi-blood,balance yin-yang, and modulate the function of Zang-fu organs, for improving the symptoms of depression patients.
People suffer from depression present decreased brain perfusion in different locations to different degrees. There are two major clinical types. One affects the frontal lobe and temporal lobe and is the most common type in depression since the frontal and temporal lobes are known closely associated with the attention, memory, abstract generalization and audio-visual discrimination. The other one affects the prefrontal lobe and limbic system. The limbic system is the anatomical basis or central structure of emotional behaviors. Decreased blood flow in the prefrontal lobe and limbic system may be related to attention deficit,affective disorders and cognitive impairment[15]. It has been proved by a trial that cranial suture acupuncture can enhance the stimulation to amygdala in the temporal lobe, so as to regulate the metabolism and release of 5-HT and NE, increasing both their contents and functions, which may be one of the mechanisms of this acupuncture method in treating depression[16].
The results of the current study showed that cranial suture acupuncture plus paroxetine significantly reduced the HAMD score of depression patients, better than the use of paroxetine alone. The observation group already showed a significant change in the HAMD score only after 1 week of treatment, indicating that the intervention acted fast. During the intervention, the patients all showed good compliance and were willing to cooperate, and the rate of adverse reactions was also quite low, suggesting that this treatment should be worth promoting in the clinic. However, the action mechanism of cranial suture acupuncture in treating depression has not been well understood, and the current studies were all focused on the short-term efficacy. Therefore, its long-term efficacy, as well as its effect on the relapse of depression and cognitive function, should be observed in the future to better guide the clinical practice.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
Acknowledgments
This work was supported by Fund Project of Taihe Hospital, Hubei University of Medicine [太和医院(湖北医药学院附属医院)院级基金项目, No. 2017JJXM103].
Statement of Informed Consent
Informed consent was obtained from all individual participants or their relatives in this study.
Received: 12 September 2017/Accepted: 15 October 2017
[1] Kessler RC, Berglund P, Demler O, Jin R, Koretz D,Merikangas KR, Rush AJ, Walters EE, Wang PS; National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA, 2003,289(23): 3095-3105.
[2] Li ZZ, Yu SY, Zhang C, Yuan CM, Hong W, Wang Y, Chen J, Huang J, Wang DX, Fang YR. Association of MTHFR gene C677T polymorphisms and depression in Han populations. Shanghai Jiaotong Daxue Xuebao (Yixue Ban),2010, 30(6): 624-627.
[3] Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause. 1990-2020: Global Burden of Disease Study. Lancet, 1997, 349(9064): 1498-1504.
[4] Li LJ, Ma X. Chinese Prevention and Treatment Guideline for Depression. 2nd Edition. Beijing: China Medical Digital and Imaging Press, 2015: 44.
[5] American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th Edition.Arlington: American Psychiatric Publishing, 2013.
[6] Yu CD, Wu BH, Chen Y, Liu C, Chen XJ, Zhang GF.Application anatomy of acupuncture at skull suture for treatment of cerebrovascular diseases. Zhongguo Zhen Jiu,2002, 22(3): 177-179.
[7] Cai XB, Yang ZX, Li Y, Zheng XB. Clinical observation on electroacupuncture plus tuina for chronic tension-type headache. J Acupunct Tuina Sci, 2017, 15(2): 120-125.
[8] Ma ZG, Jiang N, Yu MY, Xu XY, Cao DZ, Luo X.Research progress in etiology, pathogenesis and traditional Chinese medicine treatment of depression. Zhongguo Shiyan Dongwu Xuebao, 2011,19(6): 548-553.
[9] Zemlan FP, Garver DL. Depression and antidepressant therapy: receptor dynamics. Prog Neuropsyehopharmacol Biol Psychiatry, 1990, 14(4): 503-523.
[10] Lu QL. A discussion about the correlation between cranial coronal suture and point Hanyan (GB 4) to point Qubin(GB 7) of the Gallbladder Meridian. Zhonghua Zhenjiu Dianzi Zazhi, 2017, 6(1): 40-42.
[11] Wang GS, Jiang YP, Yu WL, Li CS, Yan XQ, Yu CD.Clinical observation of acupuncture at cranial sutures plus rehabilitation training for cerebral infarction. Shanghai Zhenjiu Zazhi, 2016, 35(8): 945-947.
[12] Kou RZ, Jiang Y, Xu TC, Yu ML, Wang XJ, Lu SF.Literature regarding clinical research of acupuncture for depression in the worldwide: comparison and discussion.Zhongguo Zhen Jiu, 2016, 36(9): 999-1004.
[13] Fan L, Fu WB, Chen Z, Xu NG, Liu JH, Lü AP, Li ZP, Su SY, Wu TX, Ou AH. Curative effect of acupuncture on quality of life in patient with depression: a clinical randomized single-blind placebo-controlled study. J Tradit Chin Med, 2016, 36(2): 151-159.
[14] Suzuki S, Tobe C. Effect of acupressure, acupuncture and moxibustion in women with pregnancy-related anxiety and previous depression: a preliminary study. J Clin Med Res,2017, 9(6): 525-527.
[15] Zhang YL. Textbook of Advanced Psychiatry. Changsha:Central South University Press, 2007: 414.
[16] Jin S, Peng L, Cheng JM. Clinical observation on cranial sutures acupuncture for depression after stroke. Shiyong Zhongyiyao Zazhi, 2014, 30(4): 312-313.
猜你喜欢
中国毕业后医学教育(2022年1期)2022-08-19
山东陶瓷(2021年5期)2022-01-17
教育教学论坛(2021年26期)2021-08-03
天一阁文丛(2020年0期)2020-11-05
西夏研究(2020年1期)2020-04-01
电脑知识与技术(2019年24期)2019-11-03
校园英语·中旬(2019年5期)2019-07-16
校园英语·上旬(2018年11期)2018-11-30
戏曲研究(2018年4期)2018-05-20
西藏研究(2016年6期)2016-02-28
 Journal of Acupuncture and Tuina Science2018年3期
Journal of Acupuncture and Tuina Science2018年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Clinical observation on electroacupuncture plus hydro-acupuncture for low back pain caused by compression fractures
- Effect of acupoint sticking at Shenque (CV 8) for preventing spleen-stomach disharmony caused by venous analgesia pump
- Observation on clinical effects of acupuncture plus external medicine application forcervical radiculopathy
- Observation on clinical efficacy of warm needling therapy for chronic lumbar strain
- Observation on lower-reinforcing and upperreducing acupuncture method for hyperplasia of mammary gland and its influence on estradiol and progesterone
- Influence of acupuncture on pulmonary function of patients with asthma: a review