
Observation on clinical efficacy of warm needling therapy for chronic lumbar strain
2018-06-28 09:27GuFangfang顾芳芳ZhuGaofeng朱高峰LuoKaitao罗开涛
Gu Fang-fang (顾芳芳), Zhu Gao-feng (朱高峰), Luo Kai-tao (罗开涛)
Acupuncture and Tuina Department, Jiaxing Hospital of Traditional Chinese Medicine Affiliated to Zhejiang Chinese Medical University, Jiaxing 314001, China
Lumbar strain is the general term for strains of lumbar soft tissues. It is also known as functional low back pain, lumbar dorsal myofascitis, lumbar tissue fibrosis, lumbar myofascial pain syndrome, etc. Main clinical manifestation is chronic low back pain with recurrent attacks. It is a common and frequentlyoccurring disease[1]. The lumbar strain belongs to Biimpediment syndrome in traditional Chinese medicine.Internally, it is caused by failure of the liver, spleen and kidney to nourish and warm muscles and tendoms.Externally, it is cuased by chronic strain or wind, cold or dampness obstructing the flow of qi and blood[2].External treatment of traditional Chinese medicine has a certain effect for lumbar strain[3-4]. As one of external treatments, warm needling therapy has the effect of both acupuncture and moxibustion. This study observed the clinical efficacy of warm needling therapy in treating lumbar strain.
1 Clinical Materials
1.1 Diagnostic criteria
This study referred to the diagnostic criteria of lumbar strain in theCriteria of Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine[5]: there is a long history of low back pain with recurrent attacks; pain and discomfort in one or both sides of the lumbosacral region, sometimes mild and sometimes severe,lingering unhealed, aggravated after exertion and eased after rest; mild tenderness on one or both sides of sacrospinalis muscle, generally no obvious obstacles of lumbar and leg activities.
1.2 Inclusion criteria
Those who met the above diagnostic criteria of lumbar strain; aged 20 to 70 years old; with duration more than 1 month; who ever had accepted other external treatment or conservative treatment before should taken a washout period for more than 7 d; able to receive the warm needling therapy and complete the treatment; agreed to participate in this clinical trial and signed informed consent.
1.3 Exclusion criteria
Those with lumbar disc herniation, or spinal stenosis;low back pain due to bone or joint tuberculosis,osteomyelitis, ureter or bladder disease; unclear diagnosis of spinal injury with spinal cord injury;patients with severe heart, lung, brain, or blood system disease; diabetics; had severe skin lesions or skin disease in the area to be treated; those who had received lumbar surgery; lumbar deformity;hemorrhagic blood disease patients.
1.4 Elimination and dropout criteria
Drop out because of accidents during evaluation, or poor compliance during treatment.
1.5 Adverse events
Any adverse events such as faint during acupuncture treatment, stuck needle, needle breakage, or burns occurred during the clinical study were observed.
1.6 Statistical method
1.7 General data
A total of 60 cases were selected from Acupuncture and Tuina Department of Jiaxing Hospital of Traditional Chinese Medicine Affiliated to Zhejiang Chinese Medical University, between January 2016 and December 2016.They were randomly divided into a treatment group and a control group by the random number table, with 30 cases in each group. There were no statistically significant differences in the general data between the two groups (allP>0.05), indicating that they were comparable (Table 1).
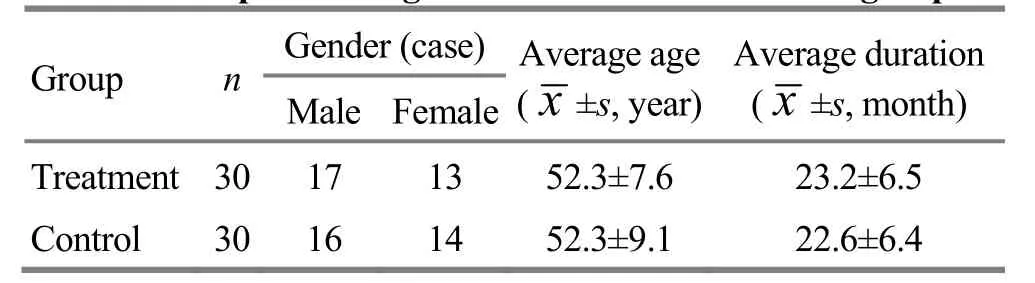
Table 1. Comparison of general data between the two groups
2 Treatment Methods
2.1 Treatment group
Acupoints: lumbar Jiaji (EX-B 2) points, Mingmen(GV 4), Yaoyangguan (GV 3), and bilateral Houxi (SI 3),Shenshu (BL 23), Pangguangshu (BL 28), Ciliao (BL 32)and Weizhong (BL 40).
Methods:The patient took a prone position. The physician perpendicularly punctured the points listed above using Hwato brand disposable sterile acupuncture needles of 0.25 mm in diameter and 40 mm in length. After arrival of qi, the even reinforcing-reducing manipulation was performed for 1 min. Then the physician applied warm needling therapy to 2-3 lumbar Jiaji (EX-B 2) points, Mingmen(GV 4), Yaoyangguan (GV 3), and Shenshu (BL 23) or Pangguangshu (BL 28), that is to slub moxa floss of about 2 cm in diameter (about 0.6 g in weight) on the needle handle, 3 cm away from the skin, and to ignite it after fixed. It was replaced with a new moxa ball after burnt out, twice for each acupoint every time. The needles were retained for 30 min. The treatment was performed once every other day, 7 times as a course of treatment, for 3 courses in total.
2.2 Control group
Acupoints: Same as those in the treatment group.
Methods:The acupuncture method, needle size,needle retention time, and course of treatment were all the same as those in the treatment group, but without warm needling moxibustion after the acupuncture.
3 Observation of Curative Efficacy
3.1 Degree of pain
Visual analog scale (VAS)[6]score was used to assess the degree of low back pain. A 10 cm line was marked‘0’ and ‘10’ respectively on the left and right ends to represent no pain and unbearable pain. The patient was asked to mark on the line to represent the degree of the pain, and the doctor recorded the score of the degree of low back pain according to the patient's mark. The higher the VAS score, the more severe the pain.
3.2 Criteria of curative efficacy
According to theCriteria of Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine[5], the curative efficacy of lumbar strain was assessed.
Cured: The symptoms of low back pain disappeared and the movement was normal.
管井宜布局在平原、高原、山区、沙漠、阶地等地区,可用于开采各种埋藏深度的地下水。大口井是傍河取水方式中一种较为常见的取水方式,主要应用在以下几个方面:1)含水层薄、渗透性好、地下水补给丰富,河漫滩、山前浅层地下水洪积扇及一级阶地、干枯河床及古河道地段;2)地下水埋藏较浅、比较厚的基岩风化裂隙层、有丰富的补给源地段;3)含水层为中细砂、采用其他取水建筑物容易侵蚀沙地的地段;4)浅层地下水含有较高含量的铁、锰及腐蚀性二氧化碳等对井管高度腐蚀作用的地区。与其他取水方式相比,大口井具有水量稳定、水质保证、项目投资少、使用寿命长、运行费用低、耐腐蚀等优点,具有较大的优越性。
Improved: Low back pain relieved and the lumbar movement recovered basically.
Invalid: The symptoms did not improve.
3.3 Results
No adverse events or dropout cases occurred during the treatment.
3.3.1 Comparison of clinical efficacy
The total effective rate of the treatment group was higher than that of the control group. The comparison result of the curative effect of the two groups was presented asZ=–2.094,P=0.036 by non-parametric rank-sum test, which suggested that the difference in clinical efficacy between the two groups was statistically significant, and the treatment group was superior to the control group (Table 2).

Table 2. Comparison of clinical efficacy between the two groups (case)
3.3.2 Comparison of VAS score
There was no significant difference in VAS score between the two groups before treatment (P>0.05).After treatment, the VAS score of both groups decreased significantly, and the intra-group differences were statistically significant (bothP<0.05). The VAS score of the treatment group after treatment was lower than that of the control group, and the difference was statistically significant (P<0.05), (Table 3).
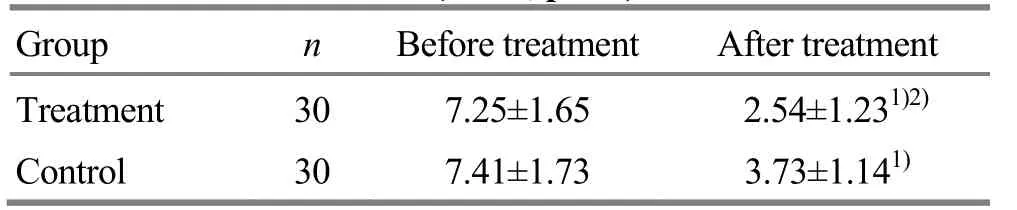
Table 3. Comparison of VAS scores between the two groups before and after treatment (x±s, point)
4 Discussion
The main clinical manifestation of chronic lumbar strain is pain and heaviness in the lumbar region. The pain will be relieved by slight activity, while aggravated by overexertion; relieved after rest but aggravated if the rest is too long. It recurrently attacks often. This disease is often caused by long-term exertion. Alternatively, it may develop from an acute lumbar sprain that was not cured in time[7-8]. Western medicine believes that the disease is a diffuse aseptic inflammation caused by chronic damage to the soft tissues of the lumbar and hips, so that it is also known as gluteal muscle fasciitis or functional low back pain, which is often the general term for chronic low back pain without organic change[9-11]. Chinese medicine believes that the low back is the house of the kidney, where the qi of the Kidney Meridian breeds. The kidney is exteriorly and interiorly related to the bladder, and the course of the Bladder Meridian goes through the lumbar region. In addition, the Conception Vessel, the Governor Vessel,the Thoroughfare Vessel, and the Belt Vessel are also distributed in lumbar region. Therefore, the internal causes of low back pain mostly are kidney deficiency,and the external causes are external contraction of wind-cold-dampness. The interaction between internal and external causes leads to this disease[12-13].
The chronic lumbar strain is characterized by low back pain as the main clinical manifestation. The combined action of internal and external causes leads to its attack. It is a syndrome of essential deficiency and superficial excess, that is, the kidney deficiency is the core, traumatic injury and external contraction are the superficiality. The lumbar is the house of the kidney, the strains of the kidney or the original kidney deficiency makes the essence of the kidney unable to nourish the tendons, bones, meridians and collaterals. Therefore,the affected area is often accompanied by disharmony of qi and blood or blood stasis and stagnation. The blood is unable to nourish the tendons that the sinews are unable to stretch, which causes the hypertonicity of the sinews and pain in the lumbar region. Kidney deficiency makes the pathogenic wind-cold-dampness easy to invade in, blocking the meridians; or long-term bending work causing the static blood generating from inside. Therefore, the prior treatment of the disease is to tonify the kidney, and then treat according to the different syndrome of pathogenic wind-cold-dampness or blood stasis. Free and unblock the meridian and collateral for the first attack, and tonify the kidney and nourish the blood for patients suffering long-term pain[14]. Therefore, in this study, Shenshu (BL 23) and Pangguangshu (BL 28) were applied. Shenshu (BL 23) is the Back-Shu point of the kidney, with the effect of tonifying the kidney and replenishing essence.Pangguangshu (BL 28) is the Back-Shu point of the bladder, with the effect of clearing heat, resolving dampness, and tonifying the kidney essence. The combination of these two acupoints made the synergistic action work[15]. Houxi (SI 3) is one of the eight confluent points, connected with the Governor Vessel (GV), and is the key acupoint for lumbago and back pain. Weizhong (BL 40) is the key acupoint for all kinds of lumbago and back pain[16]. Lumbar Jiaji (EX-B 2)points and Ciliao (BL 32) are located at the psoas attachment, and were the application of local points.Mingmen (GV 4) and Yaoyangguan (GV 3) increase the effect of tonifying the kidney and strengthening the lumbar vertebrae. The combination of all the acupoints made the effect of tonifying the kidney and strengthening the lumbar vertebrae, activating blood and resolving stasis, freeing the collateral vessels and relieving pain[17]. In this study, warm needling therapy was applied, that is to slub the moxa floss onto the needle handle and ignite it for moxibustion. The moxa has the effect of warming the meridian to dissipate cold.The burning heat of the moxa can double the effect of moving qi to free the collaterals[18-19]. The results of this study indicated that warm needling therapy had a better curative effect than ordinary acupuncture in treating chronic lumbar strain.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
Acknowledgments
This work was supported by Science and Technology Planning Project of Traditional Chinese Medicine, Zhejiang Province (浙江省中医药科技计划项目, No. 2016ZT012).Statement of Informed Consent
Informed consent was obtained from all individual participants or their relatives in this study.
Received: 2 September 2017/Accepted: 8 October 2017
[1] Wang Y, Gao H, Qi XN, Zhi M, Yao XS. Meta-analysis of ironing therapy of TCM in treating lumbar muscle strain.Zhonghua Zhongyiyao Xuekan, 2016, 34(6): 1317-1319.
[2] Xi SY, Pan Y. Advances in research on adjustable regulation of lower back pain. Zhonghua Wuli Yixue Yu Kangfu Zazhi, 2013, 35(11): 901-904.
[3] Xiong YH, Chen F. Clinical observation on 43 cases of chronic lumbar muscle strain treated by traditional Chinese medicine. Zhongguo Yixue Gongcheng, 2011, 19(1): 67-68.
[4] Wang YQ. Observation on curative effect of lumbar muscle strain treated by bow-step-rotation walking training combined with ear point pressing. Zhonghua Wuli Yixue Yu Kangfu Zazhi, 2015, 37(4): 300-301.
[5] State Administration of Traditional Chinese Medicine.Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing:Nanjing University Press, 1994: 189-190, 213.
[6] Liu Q, Mai MQ, Xiao LJ, Wu SL. Responsiveness of Chinese version of Oswestry disability index in subjects with chronic low back pain. Zhongguo Kangfu Yixue Zazhi,2010, 25(7): 621-624.
[7] Song FJ, Zheng SL, Zhang H, Hu JF, Fang JH, Ye BH, Zou XJ, Zhang WY, Liu HF. Curative effect and serum levels of IL-6, TNF-α of Lijin Cutong technique combined with cupping therapy on Bladder Meridian on the treatment of acute attack of the strain of lumbar muscles. Zhongyi Xuebao, 2015, 30(10): 1515-1518.
[8] Xu SJ, Chen XM, Cui LB, Liu YD, Yuan X, Yu ZS.Clinical observation of lumbar muscle strain treated by Biqi capsule. Zhonghua Zhongyiyao Zazhi, 2010, 25(6):958-959.
[9] Guo XH. Clinical efficacy analysis of acupuncture therapy combined with drugs on lumbar muscle strain. Linchuang Yanjiu Yu Shijian, 2016, 1(7): 55.
[10] Sun BL, Zhu CL, Li L, Tan K. Observation on short and long term curative effect of different methods in treatment of lumbar muscle strain. Xinan Guofang Yiyao, 2015, 25(2):163-166.
[11] Li ZW, Li ZL, Li W. Therapeutic effect observation on tuina with moxibustion in treating chronic lumbar muscle strain. Zhongguo Linchuang Baojian Zazhi, 2015, 18(2):211-212.
[12] Liang Y, Li BW, Su J, Gao H. Analysis of Fang Jian-qiao’s experience in treating lumbar muscle strains with acupuncture and moxibustion. Zhejiang Zhongyi Zazhi,2017, 52(1): 11.
[13] Zhou ZY, Lu S. Clinical efficacy evaluation of Bushen Quyu acupuncture in the treatment of lumbar muscle strain.Zhenjiu Linchuang Zazhi, 2013, 29(5): 15-18.
[14] Ye P, Chen SY. Clinical observation on treatment of lumbar strain with acupuncture with Sanbi decoction. Shiyong Zhongyiyao Zazhi, 2017, 33(3): 241-242.
[15] Huang LF. Efficacy observation on 120 cases of lumbar strain treated by acupoint injection. Xin Zhongyi, 2004,36(5): 50-51.
[16] Ye WH. Efficacy observation on 50 cases of lumbar strain treated by fire needling. Zhongguo Yiyao Zhinan, 2013,11(17): 295-296.
[17] Chen BW. Treatment of 117 cases of chronic lumbar strain by sliding cupping and manipulations. Zhejiang Zhongyi Zazhi, 2009, 44(5): 368.
[18] Liu SJ, Wang BQ. Effect of needle warming moxibustion combined with blood-letting puncturing and cupping on patients with acute peripheral facial paralysis. Linchuang Yixue Yanjiu Yu Shijian, 2017, 2(13): 131-132.
[19] Zhang LF, Ma YX. Study on pricking blood combined with warming acupuncture in treatment of Hunt syndrome.Xiandai Zhongxiyi Jiehe Zazhi, 2017, 26(6): 577-578, 612.
猜你喜欢
水利建设与管理(2022年4期)2022-05-12
水文地质工程地质(2022年2期)2022-04-13
建材发展导向(2021年24期)2021-02-12
海河水利(2021年1期)2021-01-06
矿产勘查(2020年11期)2020-12-25
环境影响评价(2020年5期)2020-12-02
资源信息与工程(2019年3期)2019-07-01
天津建设科技(2019年6期)2019-03-08
中国氯碱(2014年11期)2014-02-28
资源环境与工程(2014年5期)2014-01-16
 Journal of Acupuncture and Tuina Science2018年3期
Journal of Acupuncture and Tuina Science2018年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Clinical observation on electroacupuncture plus hydro-acupuncture for low back pain caused by compression fractures
- Therapeutic observation of cranial suture acupuncture in treating depression
- Effect of acupoint sticking at Shenque (CV 8) for preventing spleen-stomach disharmony caused by venous analgesia pump
- Observation on clinical effects of acupuncture plus external medicine application forcervical radiculopathy
- Observation on lower-reinforcing and upperreducing acupuncture method for hyperplasia of mammary gland and its influence on estradiol and progesterone
- Influence of acupuncture on pulmonary function of patients with asthma: a review