
Effects of acupuncture on ovarian blood supply and pregnancy outcomes in patients receiving assisted reproduction
2018-09-12 02:45XuZhengzheng徐铮铮GaoYing高颖
Xu Zheng-zheng (徐铮铮), Gao Ying (高颖)
Abstract Objective: To observe the effects of acupuncture at the follicular phase on ovarian blood supply and pregnancy outcomes in patients who received in vitro fertilization/intracytoplasmic sperm injection-embry transfer (IVF/ICSI-ET) of assisted reproductive technology (ART).Methods: A total of 169 IVF/ICSI-ET female recipients from the Reproductive Center of Xiehe Hospital, Tongji Medical College, Huazhong University of Science & Technology were randomized into an observation group (57 cases), a placebo group (54 cases) and a control group (58 cases). The observation group received acupuncture during the follicular phase,meanwhile the placebo group received placebo-acupuncture, and the control group did not receive acupuncture. The hemodynamic index, biochemical pregnancy rate and clinical pregnancy rate of each group were observed, respectively.Results: As to the ovarian arterial hemodynamic index, the pulsatility index (PI), resistance index (RI), and the systolic-to-diastolic peak velocity ratio (S/D) of the observation group were (0.819±0.131), (0.552±0.055) and (2.306±0.512),respectively, obviously lower than those in the placebo group and the control group, and the differences were statistically significant (all P<0.05), but there were no statistically significant differences between the placebo group and the control group (all P>0.05). As to the biochemical pregnancy rate and clinical pregnancy rate, the biochemical pregnancy rate in the observation group was 64.9% and the clinical pregnancy rate was 52.6%, which were significantly higher than those in the placebo group and the control group, and the differences were statistically significant (all P<0.05), while there were no significant differences between the placebo group and the control group (both P>0.05).Conclusion: Acupuncture treatment during the follicular phase can improve ovarian blood supply and pregnancy rate in those receiving IVF/ICSI-ET.
Keywords: Acupuncture Therapy; Infertility, Female; Reproductive Technology, Assisted; Fertilization in Vitro; Sperm Injections, Intracytoplasmic; Embryo Transfer; Pregnancy Rate
In recent years, the incidence of infertility has increased due to the deteriorating environment, and the delay of marriage and childbearing age. The assisted reproductive technology (ART), in vitro fertilization/intracytoplasmic sperm injection-embryo transfer (IVF/ICSI-ET) has become the most effective method to treat infertility. Currently, the increase in pregnancy rate and the decrease in complications are achieved by improving the superovulation program, developing the laboratory culture systems, and developing molecular biology techniques. At present, the embryo transfer pregnancy rate is still only about 40%. Therefore,people are trying to improve the success rate of assisted reproduction through various means.
Acupuncture and moxibustion therapy of traditional Chinese medicine has a long history in treating infertility,with the advantage of safety and low cost, and reliable efficacy. Great progress has been made by combining acupuncture and modern obstetrics and gynaecology in treating infertility[1-3], such as that electroacupuncture(EA) can reduce the blood flow impedance of infertility women's uterine artery[3], directly influencing endocrine and ovulation. Dieterle S, et al[4]from Witten University in Dortmund, Germany, performed a study of the effect of acupuncture during luteal phase on IVF/ICSI outcomes in 225 cases of IVF/ICSI recipients grouped by traditional Chinese medicine theory. The results showed that the clinical pregnancy rate and the continuing pregnancy rate in the acupuncture group were significantly higher than those in the placebo acupuncture group, indicating that acupuncture during luteal phase had a positive effect on the outcomes of IVF/ICSI.
By the use of transvaginal color Doppler ultrasound to observe the ovarian arterial blood flow, the direct and dynamic monitoring of the size, morphology, and blood supply of the follicle can indirectly reflect the periodic changes in sex hormone levels. This method is widely used in the examination of the etiology of female reproductive system diseases, and can guide the selection of ovulation induction project in the treatment of infertility, and the adjustment of drugs and dosages.
The hemodynamic parameters include peak systolic flow velocity (PSV), resistance index (RI), and pulsatility index (PI), all of which can be read directly by the built-in software of the ultrasound. The decrease in RI and PI reflects the reduction in vascular resistance and the increase in ovarian blood flow velocity in the presence of dominant follicles or corpus luteum. The RI around the follicles is the lowest during the ovulation period, and more blood flow is supplied to the dominant follicles[5]. In the same period of ovulation and luteal phase, the RI of ovulatory ovarian arteries is significantly lower than that of non-ovulatory side,indicating that the ovulatory ovarian arteries has higher blood flow than the non-ovulatory side, and the blood flow supply is more abundant.
The aim of this study was to observe the effect of acupuncture treatment during follicular phase on ovarian blood supply and pregnancy outcomes in patients receiving IVF/ICSI-ET.
1 Clinical Materials
1.1 Diagnostic criteria
The World Health Organization defines infertility as those who do not have contraception, have normal sexual life, and have lived together with the partner for one year but fail to be pregnant. In vitro fertilizationembry transfer (IVF-ET) is the technique to achieve pregnancy by removal of eggs and sperm from infertile couples, fertilization and development of embryos in an in vitro culture system, and transfer of high-quality embryos into the patient's uterine. Intracytoplasmic sperm injection (ICSI) is to directly infuse the single sperm into the oocyte cytoplasm in vitro to make it fertilized with the help of a microscope operating system.
1.2 Inclusion criteria
Female with gamete transport obstacles, ovulatory disorders, or endometriosis due to various factors;infertility of unclear causes; immunological infertility with no indication of surgery; aged 18 to 45 years old;planned to receive IVF/ICSI-ET; signed informed consent.
1.3 Exclusion criteria
Those with cardiovascular, liver, kidney, or hematopoietic system disease; had significant infections in one part of the body (such as obvious throat infections); osteoporosis; pregnant and lactating women; took five or more Western medicines one time which lasted more than 3 years.
1.4 Elimination and dropout criteria
Dropout because of poor compliance or any other reasons.
1.5 Statistical methods
All data were statistically analyzed by the SPSS version 19.0 statistical software. Measurement data in normal distribution were expressed as mean ± standard deviation (±s). Variance analysis was applied to the comparison of general data. Least significant difference(LSD) t-test was applied to the comparison of ovarian hemodynamic index in each group. Chi-square test was applied to the comparison of non-ranked data. P<0.05 was considered to indicate a statistically significant difference.
1.6 General data
A total of 169 IVF/ICSI-ET recipients were collected from the Reproductive Center of Xiehe Hospital, Tongji Medical College, Huazhong University of Science &Technology. The random number was generated by computer and the random cards were sealed in envelopes with the serial random number, under dedicated management. The envelopes were opened according to the order of inclusion, and the case number and group were obtained. The patients were divided into an observation group (57 cases), a placebo group (54 cases) and a control group (58 cases). The observation group received acupuncture during the follicular phase, meanwhile the placebo group received placebo-acupuncture, and the control group did not receive acupuncture. This study was a predicting randomized controlled trial that had been reviewed by the Ethics Committee of Tongji Medical College,Huazhong University of Science & Technology. Each participant was voluntary and had signed formal informed consent. All patients participated in this study only once. The grouping was confidential to doctors who operated egg retrieval and transplantation.Acupuncture was performed by one same doctor. There were no statistically significant differences in the general data of age, body mass index (BMI), infertility time, infertility causes, test-tube cycles, treatment methods (IVF/ICSI-ET), time of ovulation induction,count of egg retrieval and fertilization rate (all P>0.05),indicating that the three groups were comparable(Table 1).

Table 1. Comparison of the general data of the three groups
2 Treatment Methods
The three groups all received IVF/ICSI-ET and a long regimen of ovulation induction. Down regulation started on the 21st day of the previous menstrual cycle.Triptorelin acetate injection (decapeptyl) 0.05 mg was injected subcutaneous daily until the day of the injection of human chorionic gonadotropin (HCG). The down regulation was considered qualified if the serum levels of follicle stimulating hormone (FSH) <5 mU/mL,luteinizing hormone (LH) <5 mU/mL, estradiol (E2)<50 pg/mL, and bilateral follicle diameters <10 mm on the second day after menstruation. Recombinant human follitropin for injection (gonal-f) 2-3 units were applied starting from the third day of menstruation to stimulate ovulation. The dosage was individualized and prescribed according to previous reactions. During the period of ovulation induction, the size of the follicles was measured by transvaginal ultrasound, and the dose of hormones was adjusted accordingly. HCG (10 000 IU)was injected when at least 3 leading follicles with an average diameter ≥18 mm were observed by ultrasound,and serum E2level of each large follicle was sufficient.Thirty-six hours after the injection of HCG, the eggs were retrieved under vaginal ultrasound guidance. 2-3 d after the retrieval, the embryos was transplanted into the uterus. Two embryos for transplantation were routine, three would be transplanted if the patient was aged ≥35 years old. The corpus luteum support started on the day of egg retrieval. Intramuscular injection of progesterone 60 mg/d, oral estradiol valerate tablets(progynova) and dydrogesterone tablets (duphaston)were performed until the 14th day after the transplantation. Then the blood β-HCG was examined, if the patient was pregnant, the prescription was continued. On the 30th day after the transplantation,intrauterine gestational sac and heart beat were observed by vaginal ultrasound, which suggested clinical pregnancy, then the medication was reduced gradually and lasted till 2-3 months of pregnancy.
2.1 Observation group
Acupuncture treatment was applied during the follicular phase.
Acupoints: Guanyuan (CV 4), Zhongji (CV 3), Zigong(EX-CA 1), Guilai (ST 29), Sanyinjiao (SP 6) and Xuehai(SP 10).
Method: Disposable stainless steel filiform needles of 0.30 mm in diameter and 40 mm in length were used.
Acupuncture treatment began on the 7th day of menstruation. Before the needling, the patient was required to empty the bladder. According to the different locations of these acupoints, the physician perpendicularly punctured by 0.5-1.2 cun in depth.After insertion of the needles, the twirling manipulation was performed to induce the feeling of obtaining qi as soreness, numbness, distension, heaviness. And twirling manipulation was performed once again after 15 min to maintain the feeling. The needles were retained for 30 min. The treatment was performed daily till the day of HCG injection.
2.2 Placebo group
Acupoints: Acupoints that were not related to infertility treatment including Fengshi (GB 31),Yanglingquan (GB 34), Waiguan (TE 5) and Sidu (TE 9).
The operation and treatment course were same as those in the observation group.
2.3 Control group
No acupuncture treatment was applied to patients in the control group.
3 Observation of Therapeutic Efficacy
3.1 Observation items
3.1.1 Ovarian hemodynamic index
Ovarian arterial hemodynamic index was measured at the same time (8:00 a.m. to 12:00 a.m.) on the day of HCG injection.
Operation: The patient took a lithotomy position. The vaginal probe was covered with a disposable latex cover or condom. Insider the cover was coated with the disinfecting coupling agent, and the probe was placed at posterior fornix. Doppler probe was used for blood flow measurement with a frequency of 5 MHz. The ovarian blood flow signal was located on the side of the ovary,and the direction of the blood flow was at an angle of 0-15° with the sound beam. The sampling frame was placed at the ovarian artery to obtain a satisfactory blood flow spectrum, and measurements were made after at least 5 stable waveforms appeared. The operation was performed by the same physician to avoid operation error.
Test items: RI, PI and systolic-to-diastolic peak velocity ratio (S/D) could all be read directly by built-in software of ultrasonic system. Each item was measured 3 times and the average value was taken. After bilateral ovarian were measured, the mean value was taken as the final value.
3.1.2 Biochemical pregnancy rate and clinical pregnancy rate
On the 14th day after the transplantation, the blood β-HCG was >2.0 mIU/mL, indicating biochemical pregnancy. On the 30th day after the transplantation,intrauterine gestational sac and heart beat were observed by transvaginal ultrasound, suggesting clinical pregnancy.
3.2 Results
In this study, a total of 169 patients had at least one embryo implanted, including 57 cases in the observation group, 54 cases in the placebo group, and 58 cases in the control group. No dropout or lost follow-up cases occurred during the treatment.
3.2.1 Comparison of ovarian hemodynamic indexes
The PI, RI and S/D of the ovarian hemodynamic indexes of the observation group were (0.819±0.131),(0.552±0.055) and (2.306±0.512), respectively,significantly lower than those of the placebo group and the control group. The differences were statistically significant (all P<0.05). There were no significant differences in hemodynamic items between the placebo group and the control group (all P>0.05),(Table 2).
Table 2. Comparison of ovarian hemodynamic indexes (±s)
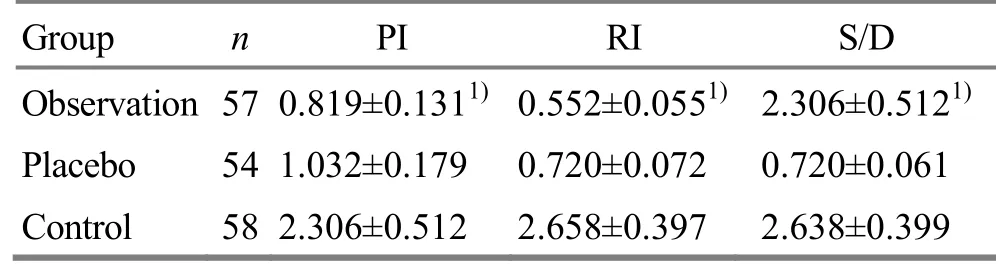
Table 2. Comparison of ovarian hemodynamic indexes (±s)
Note: Compared with the placebo group and the control group, 1)P<0.05
Group n PⅠ RⅠ S/D Observation 57 0.819±0.1311) 0.552±0.0551) 2.306±0.5121)Placebo 54 1.032±0.179 0.720±0.072 0.720±0.061 Control 58 2.306±0.512 2.658±0.397 2.638±0.399
3.2.2 Comparison of biochemical pregnancy rate and clinical pregnancy rate
The biochemical pregnancy rate and clinical pregnancy rate of the observation group were 64.9%and 52.6%, respectively, significantly higher than those of the placebo group and the control group. The differences were statistically significant (all P<0.05). The biochemical pregnancy rate and clinical pregnancy rate of the placebo group were higher than those of the control group, but the differences were not statistically significant (both P>0.05), (Table 3).
4 Discussion
Good seeds can develop into good quality fruits.Therefore, in the course of assisted pregnancy by IVF/ICSI-ET, the growth of follicle after ovulation induction is one of the most critical factors determining the success of in vitro or not. Acosta TJ, et al[6]found that the PI of functional side of ovarian arteries was lowest at the time of ovulation through animal experiments. The change in PI was negatively correlated with the increase in follicular diameter, and the concentration of plasma E2as well. The lower the values of RI and PI, the more blood flow supplied to the dominant follicles, and the better the quality of the follicles. Zhang Y, et al[7]measured blood flow parameter around the follicles of >12 mm in diameter by vaginal color Doppler ultrasound in his working center on the day of HCG of 66 cycles (including IVF and ICSI). The RI and S/D values of non-pregnant group were significantly higher than those of the pregnant group. When RI ≤0.49, the pregnancy rate, fertilization rate, cleavage rate, and the amount of oocytes in M2 phase (That is, the oocyte of the second meiotic metaphase has already discharged the first polar body, which can be combined with sperm to discharge the second polar body to become fertilized egg) were all increased significantly, while there were no statistically significant differences in the dose of gonadotropin (Gn), time of cycle, year of infertility, age,concentration of E2on HCG injection day, amount of retrieved egg, and the rate of good embryos. There were no statistically significant differences in the values of follicular blood flow arteries end-systolic peak (S) and end-diastolic peak (D) between the pregnant and non-pregnant groups. There was no correlation between the follicular artery RI and the follicular diameter, indicating that the follicular artery RI was an effective indicator for pregnancy outcome prediction of IVF/ICSI-ET. The growth of follicles depends on the blood supply of the ovarian artery. In 1999, Coulam CB,et al[8]found that the more blood flow signal around the follicles, the more mature the follicles were. The strong color signals around the follicles indicated that there were more blood vessels formed around the follicles, and the follicular oxygen was richer in the fluid and the fertilization rate was higher. The decrease in ovarian arterial hemodynamic index reflected the reduction in vascular resistance and increase in blood flow velocity. The index of blood flow in the ovarian arteries of the functional side was lowest at ovulation,and its change was negatively correlated with the increase in the follicles in diameter[9]. The lower the values of these indices, the more blood flow supplied to the dominant follicles and the better the quality of the follicles. Li LM, et al[10]measured the PSV, RI, and PI of ovarian vessels in the controlled ovarian hyperstimulation (COH) in 54 women who received IVF/ICSI-ET at their Reproductive Center, and they found that the ovarian matrix vessel PI and RI maintained a high level on D1 (the first day of Gn use), decreased after then, and showed a trend to rise after the injection of HCG. There was no significant wave of vascular resistance during the entire period of COH,basically remaining stable and not showing a significant decrease before natural ovulation, which might be an important reason why natural ovulation did not occur easily during the COH cycle. The results showed that PI and RI were positively correlated with the Gn level on D1. There were significant differences in RI between groups with different days of medication indicating that the higher the PI and RI, the greater the dosage of Gn.There were statistically significant differences in ovarian matrix blood flow impedance and peak velocity among the groups of low, medium, and high ovarian reaction on D1. That is, a low-speed, high-resistance type was expressed in the low response group, while a high-speed, low-impedance type was showed in the blood flow of the high-response group. Some studies indicated that the ovarian blood flow index in the IVF pregnancy group was significantly decreased, and the ovarian blood flow was an effective indicator of pregnancy outcome prognosis positively correlated with the pregnancy outcome in vitro[11-15]. Sun ZG, et al[16]performed a study that showed the effect of acupuncture combined with intraluminal physical therapy in improving pre-retrieval oocytes and the endometrial blood supply, the promotion of egg quality,and optimization of plantation condition for endometria,which finally increased the clinical pregnancy rate.Zheng Y[17]found that transcutaneous electric acupoint stimulation could increase the number of antral follicle in patients with decreased ovarian reserve function and improve the ovarian function. It could also reduce the dosage and course of gonadotropin application in the IVF process, and increase the number of retrieval egg and the high- quality embryos, which improved the therapeutic effect of IVF.
In this study, Guanyuan (CV 4), Zhongji (CV 3), Zigong(EX-CA 1), Guilai (ST 29), Sanyinjiao (SP 6), and Xuehai(SP 10) were selected in the observation group. They were closely related to the female reproductive system.Acupuncture at these points could improve the blood supply to the ovary and uterus, promote the blood flow,and improve the growth and development of follicles.The mechanism might be the benign regulation on the secretion function of the hypothalamus-pituitaryovarian axis, which could normalize the secretion of gonadal hormones to improve ovulation function.Studies showed that acupuncture for ovulation induction also correlated with its inhibition of sympathetic center to change the brain neurotransmitters[18-22]. D'Anna R, et al[23]analyzed the neuro-endocrine mechanism produced by acupuncture and moxibustion, and pointed out that the realization of the effect was closely correlated with cell information transmission. Part of the acupuncture effect was generated from the acupuncture signal passing from the acupoint to the central nervous system through the peripheral nerve, triggering the activity of the body's neuroendocrine system, and resulting in the release of certain biologically active substances and the activation of the target cell's information conduction function.Under the effect of neuro-humoral factors, the corresponding information of the acupuncture signal was transmitted into the cells, resulting in a series of biological effects, and the function of the acupuncture in regulating functions of various body systems was finally realized. The study of Li N[24]indicated that acupuncture could significantly relieve pain, improve the rate of high-quality eggs, and prevent ovarian hyperstimulation.
Researchers of Cornell University searched the literature data and found that some effects of acupuncture on patients receiving IVF/ICSI were through the medium of endorphins of the central nervous system, especially β-endorphin[25]. These neuropeptides affected the secretion of gonadotropin by the effect on gonadotropin-releasing hormone(GnRH). As shown in Table 2, the blood flow RI and PI of the observation group were significantly lower than those of the control group, indicating that the ovarian blood supply and the egg quality of the observation group were better, resulting in the better pregnancy outcomes.
In this study, the placebo group was applied with the method of acupuncture at ineffective acupoint, that is,the selected acupoints were almost unrelated to the female reproduction. The pregnancy rate of the placebo group was higher than that of the control group, but the difference was not statistically significant, indicating that acupuncture may have a certain psychological effect. Therefore, further experimental researches with larger sample sizes were needed in this field in the future.
The results of this study indicated that acupuncture at follicular phase could improve the ovarian blood supply and the pregnancy rate in patients receiving IVF/ICSI-ET. It provided a basis for improving the method of in vitro fertilization. In the future,acupuncture and moxibustion may become an important adjuvant therapy in the treatment of fertility.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
Statement of Informed Consent
Ⅰnformed consent was obtained from all individual participants included in this study.
Received: 13 October 2017/Accepted: 19 November 2017
 Journal of Acupuncture and Tuina Science2018年4期
Journal of Acupuncture and Tuina Science2018年4期
- Journal of Acupuncture and Tuina Science的其它文章
- Therapeutic efficacy observation on acupuncture for persistent allergic rhinitis
- Observation of therapeutic effects of point application at Shenque (CV 8) plus moxa-salt hot compress for prevention of gastrointestinal adverse reactions after chemotherapy for non-Hodgkin lymphoma
- Effect of Governor Vessel-unblocking and mindrefreshing acupuncture plus functional training on neural development in infants with brain damage
- Correlation analysis on clinical effects of acupuncture for elderly patients with sensorineural deafness and ear distending sensation
- Clinical observation of abdominal acupuncture for subhealth insomnia
- Application and exploration of suspended magnetic moxibustion cup for obesity