
Correlation analysis on clinical effects of acupuncture for elderly patients with sensorineural deafness and ear distending sensation
2018-09-12 02:45MoWenquan莫文权ChuWenhao褚文浩YangHui杨晖WangJie王洁PeiJian裴建
Mo Wen-quan (莫文权), Chu Wen-hao (褚文浩), Yang Hui (杨晖),Wang Jie (王洁), Pei Jian (裴建)
Abstract Objective: To investigate the relationship between clinical effects of acupuncture for elderly patients with sensorineural deafness and ear distending sensation.Methods: A total of 120 elderly patients with sensorineural deafness were randomly divided into a comprehensive treatment group, an acupuncture group and a Western medicine group, with 40 cases in each group. The acupuncture group received acupuncture treatment, the Western medicine group received oral mecobalamin tablets and the comprehensive treatment group received acupuncture plus acupoint injection and auricular acupoint sticking. The values of pure tone hearing threshold test of the three groups were observed before and after treatment, and the relationship between clinical effects and ear distending sensation was compared.Results: The total effective rate of the comprehensive treatment group was 82.5% versus 67.0% in the acupuncture group and 62.5% in the Western medicine group. The inter-group comparisons showed statistically significant differences in the comprehensive treatment group versus the Western medicine group (P<0.01) and the acupuncture group (P<0.05). In the comprehensive treatment group, there were 23 cases (57.5%) with ear distending sensation, the clinical total effective rate was 86.9%; there were 17 cases (42.5%) without the sensation, the clinical total effective rate was 76.5%. In the acupuncture group, there were 24 cases (60.0%) with ear distending sensation, the clinical total effective rate was 71.0%;there were 16 cases (40.0%) without the sensation, the clinical total effective rate was 63.0%. In the Western medicine group, there were 21 cases (52.5%) with ear distending sensation, the clinical total effective rate was 66.7%; there were 19 cases (47.5%) without the sensation, the clinical total effective rate was 57.9%. The total effective rate of patients with ear distending sensation were higher than the rates of those without ear distending sensation in the three groups, but the differences were insignificant (all P>0.05).Conclusion: The comprehensive therapy is one of the effective methods to treat elderly patients with sensorineural deafness. In the three groups of elderly patients with sensorineural deafness, the relief of ear distending sensation and the hearing loss were basically simultaneous, and the hearing recovery in the patients with ear distending sensation may be slightly better than that in those without ear distending sensation. Nevertheless, further research is needed.
Keywords: Acupuncture Therapy; Auricular Acupoint Sticking; Acupoint-injection; Deafness; Audiometry; Auditory Threshold; Aged; Randomized Controlled Trial
Sensorineural deafness is commonly seen in elderly patients treated in the Otorhinolaryngology Department and the Acupuncture-moxibustion Department. The impairment includes hair cells of cochlea spiral device, auditory nerves and cerebral cortex. Because of its complicated etiology and pathogenesis, it has become a major issue in the medical field[1]. Elderly sensorineural deafness is often accompanied by varying degrees of ear distending sensation. This sensation of the ear can be manifested as sensation of bulging, blockage and oppression. The outpatient morbidity rate is about 1% to 2%, of which the female is a high-risk group[2]. The sensation can produce negative emotions such as depression, anxiety and even detachment, which is especially evident in severe patients[3]. However, there are few reports to regard ear distending sensation as an observation item for clinical effect evaluation[4-5].
This study was to observe the clinical effect of acupuncture combined with acupoint injection and auricular acupoint sticking therapy on senile sensorineural deafness. The relationship between ear distending sensation and the clinical effect was analyzed.The report is as follows.
1 Clinical Materials
1.1 Diagnostic criteria
Diagnosis of sensorineural deafness was in accordance with the relevant standards in the Diagnostics of Otolaryngology[6].
Subjective symptoms: Hearing loss, deafness or having difficulty distinguishing words in either quiet or noisy environments; accompanied tinnitus or tinnitus alone without hearing loss, being either constantly or inconstantly, light or loud, with patients’ work, study and sleep being affected; possibilities of accompanied dizziness, sensation of blocked ears, and auditory hypersensitivity.
Ear examination: There were no obvious malformations or organic pathological changes seen in the external ear canal and tympanic otoscopy; ear auscultation revealed non-objective tinnitus; pure tone audiometry was consistent with sensorineural deafness.
Sensorineural hearing loss: Both air and bone conductance measurements decreased, and the conductance difference was <10 dB.
1.2 Inclusion criteria
Patients with non-hereditary sensorineural deafness who met the diagnostic criteria; hearing loss was still increasing or fluctuating; aged over 60 years old; with no gender limitation; no treatment used after the onset,or received treatments ineffective with discontinuation for more than one week; with no systemic comorbidities; with clear consciousness to cooperate with examination and adhere to treatment.
1.3 Exclusion criteria
Those did not meet the diagnostic criteria or inclusion criteria; those with foreign body inflammation or tumor in the ear; diagnosed as conductive deafness of mixed deafness through the ear examination; those with evident epidemic history of infectious disease such as ear herpes, epidemic cerebrospinal meningitis,mumps, measles lately or before the occurrence of deafness; those with central deafness caused by central brain lesions; those diagnosed as congenital deafness of acoustic nerve tumors by the auditory examination;those received other treatments simultaneously or within 2 weeks of the start of the observation; those unable to adhere to treatment or follow-up due to external causes or personal tolerance.
1.4 Statistical methods
The SPSS version 22.0 statistical software was used for data processing and statistical analysis. The measurement data were tested for normality and homogeneity of variance at the first place. Data meeting normal distribution and equal variance were expressed as mean ± standard deviation (±s). The paired sample t-test was used for intra-group comparison before and after the treatment. One-way analysis of variance was used for the comparison between groups. The difference was statistically significant at P<0.05.
1.5 General data
A total of 120 patients from in-patient and out-patient of Otorhinolaryngology and Acupuncture Departments in Huadong Hospital, Fudan University were enrolled between December 2014 and February 2017. All patients signed the informed consent after being informed of the contents of the study verbally and in writing. The approval of Ethics Committee of Huadong Hospital, Fudan University (approval number:20140132) and the clinical trial registration (registration number: ChiCTR-IOR-14005700) were completed before the 1st case included.
The patients were randomly divided into a comprehensive treatment group, an acupuncture group and a Western medicine group according to the visit order by random number table with 40 cases in each group. There was no significant differences in gender,age or duration among the three groups (all P>0.05),indicating that they were comparable (Table 1).

Table 1. Comparison of three sets of general information
2 Methods
Treatments were performed by doctors in our study group after finishing standard training. Members of the study group were at least attending physicians, having abundant experience in acupuncture clinical work.
2.1 Comprehensive treatment group
2.1.1 Acupuncture therapy
Main acupoints: Sishencong (EX-HN 1), Tinggong(SI 19), Tinghui (GB 2), Erming (Extra, 2 cun above the tip of the ear) on the affected side, and Jingqu [Extra,straight above Yifeng (TE 17) at the same level of the tip of the ear][7].
Adjunct acupoints: Hegu (LI 4), Quchi (LI 11) and Zhongzhu (TE 3).
Acupoints based on disease differentiation: Those with insufficient cerebral blood supply, Fengchi (GB 20)and cervical Jiaji (EX-B 2) were added; those with poor sleep, Neiguan (PC 6) and Shenmen (HT 7) were added.
Method: After routine disinfection by 75% alcohol cotton ball, filiform needles of 0.22 mm in diameter and 40 mm in length were used to puncture swiftly. After the arrival of needling sensation, the twirling manipulation was adopted to rotate the needles by a two-way 360° angle to promote the needle sensation to the ear. The needles were retained for 60 min, and manipulations were conducted every 30 min. The treatment was performed once every other day.
2.1.2 Acupoint injection therapy
Acupoints: Tinggong (SI 19) and Yifeng (TE 17) on the affected side (used alternately).
Method: One milliliter of mecobalamin injection(national drug approval number: H20130076, Shanghai Suzuken Huzhong Pharmaceutical Co., Ltd., China) was drawn by a syringe for acupoint injection. The treatment was performed once every other day.
2.1.3 Auricular acupoint sticking
Ear acupoints: Shenmen (TF4), Kidney (CO10), Liver(CO12), Spleen (CO13), Adrenal Gland (TG2p), Inner Ear(LO6), Outer Ear (TG1m), Sympathetic (AH6m) and Subcortical (AT4).
Manipulation: Applied the seed of Wang Bu Liu Xing(Semen Vaccariae) to the auricular acupoints of the affected side. The treatment was performed once every other day.
2.2 Acupuncture group
The same acupoint selection and treatment manipulation of the acupuncture therapy as those adopted in the comprehensive treatment group.
2.3 Western medicine group
Oral administration mecobalamin tablets (national drug approval number: H20143107, 0.5 mg/tablet,Shanghai Suzuken Huzhong Pharmaceutical Co., Ltd.,China), 0.5 mg, tid.
2.4 Treatment course
Ten-day treatment constituted a course. A one-week rest was taken after the first course. The treatment continued for another course after the rest. A total of 2 courses were performed.
3 Therapeutic Effect Observation
3.1 Observation items
According to the method specified in the Acoustics-Audiometric Test Methods: Basic Pure Tone Air and Bone Conduction Threshold Audiometry[8], a Clinical Audiometer AC40 pure tone audiometry instrument was used to perform pure tone auditory threshold test at frequencies of 0.5 kHz, 1 kHz, 2 kHz, and 4 kHz,respectively, in a soundproof room to observe the hearing loss level. The results of average hearing threshold were recorded and calculated.
3.2 Efficacy criteria
In accordance with the Clinical Diagnostic Basis and Criteria for Cure and Improvement of Disease[9].
Cure: The average hearing threshold at the 4 frequencies returned to normal, or reached the level before the onset of the illness, or reached the level of the healthy ear; symptoms such as tinnitus and dizziness disappeared; no relapse at the 1-month follow-up.
Markedly effective: The average hearing threshold at the 4 frequencies was improved by 30 dB or more, or the value of single hearing frequency test was restored to 15 dB or above; accompanied tinnitus symptoms became intermittent from continuous, the appearance and aggravation in noisy environment improved to occurrence in quiet environment only, and the affected work, sleep and mood turned back to normal.
Effective: The average hearing threshold at the 4 frequencies was increased by 15 dB or above;symptoms such as tinnitus were improved to sporadic and low volume from continuous and high volume; or tinnitus only appeared in quiet environment or at night,so that daily activities were not affected.
Invalid: The average hearing threshold at 4 frequencies was improved by no more than 15 dB;symptoms such as tinnitus and vertigo were not improved.
3.3 Treatment results
3.3.1 Comparison of clinical efficacy of hearing
The total effective rate in the comprehensive treatment group was 82.5%, versus 67.0% in the acupuncture group and 62.5% in the Western medicine group, expressing a better clinical effect in improving the pure tone auditory threshold in the comprehensive treatment group versus the acupuncture group and the Western medicine group (P<0.05, P<0.01). There was no significant difference in clinical efficacy between the acupuncture group and the Western medicine group(P>0.05), (Table 2).
3.3.2 Relationship between ear distending sensation and hearing improvement
The total effective rate of hearing loss accompanied by distending sensation was 86.9% in the comprehensive treatment group, 71.0% in the acupuncture group and 66.7% in the Western medicine group, slightly higher than the effective rate of those without ear distending sensation [76.5% in the comprehensive treatment group (χ2=0.321, P=0.571),63.0% in the comprehensive treatment group (χ2=0.029,P=0.866) and 57.9% in the Western medicine group,(χ2=0.321, P=0.571)], but the differences were statistically insignificant. The results suggested that there was certain correlation between the efficacy of hearing loss and ear distension. The clinical efficacy of hearing loss in patients with ear distending sensation may be higher than that in patients without ear distending sensation (Table 3).

Table 2. Clinical effects of hearing in the three groups (case)
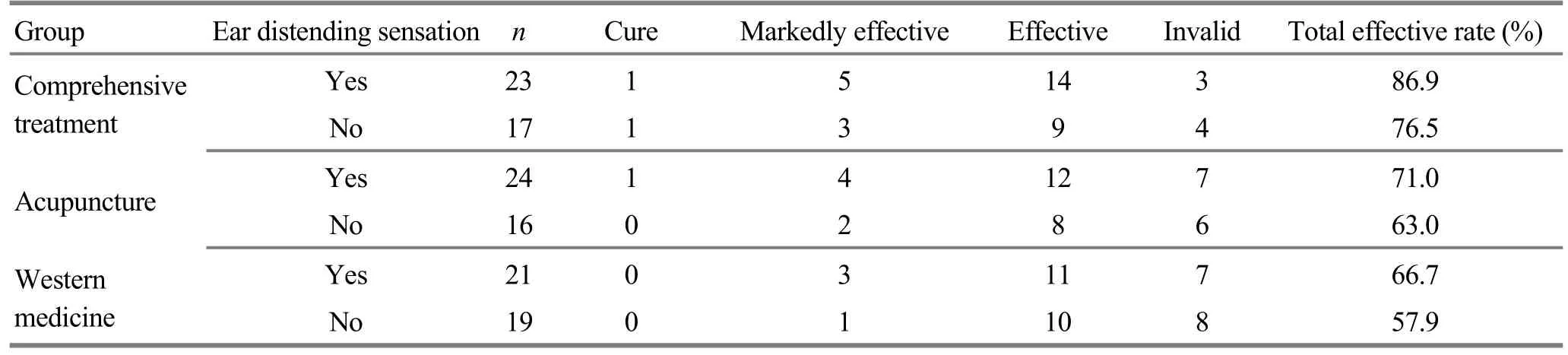
Table 3. Relationship between ear distending sensation and clinical efficacy in each group (case)
4 Discussion
In recent years, with the population aging, the incidence of sensorineural deafness in the elderly has also increased[10]. Modern medicine believes that sensorineural deafness is caused by damage to spiral hair cells, auditory nerves, auditory conduction pathways, and neurons at all levels due to drugs, noise,trauma, and viruses[11-12]. Western medicine treatment of sensorineural deafness includes vasodilators,vitamins, mecobalamin, and neurotrophic factors[10].Due to its varying causes and complicated pathological mechanisms, though Western medicine has certain effects for senile deafness, there is lack of specific drugs and therapies[13]. Chinese medicine has a long history and rich experience in the understanding and treatment of deafness. Acupuncture treatment plays an important role in various therapies of traditional Chinese medicine.In recent years, acupuncture has achieved positive clinical efficacy in the treatment of sensorineural deafness[14-18]. Studies have shown that acupuncture can improve the inner ear nerve function by regulating the inner ear and brain stem microcirculation, and promote the recovery of inner ear hair cells[19]. Based on the meridian theory of traditional Chinese medicine:meridians function along where they pass through,acupoints around the ears and along the meridians are often selected to achieve good clinical results in improving hearing loss[20-21]. The results of this study indicated that the clinical efficacy of the comprehensive treatment group was superior to that of the acupuncture group (P<0.05) and the Western medicine group (P<0.01). Erming (Extra, 2 cun above the tip of the ear) and Jingqu [Extra, straight above Yifeng (TE 17)at the same level of the tip of the ear] used in the comprehensive treatment are experienced points[7]summed up through long-term clinical practice.Combining the two points with acupoint injection and auricular acupoint sticking therapy can exert the joint action of acupoints and drugs to further strengthen qi and blood circulation to improve the local hemorheological indexes. Traditional Chinese medicine believes that deafness is generally caused by pathogenesis of localized blood stasis and meridian blocking, which especially occur in elderly patients with a long course of illness. Therefore, the comprehensive treatment can improve the symptoms of the disease by unblocking the meridians, promoting qi circulation and removing blood stasis to increase the hearing threshold.
Through this study, we found that for elderly patients with sensorineural deafness, there was certain correlation between clinical efficacy and ear distending sensation, but there was no inevitable connection. The majority of patients with sensorineural hearing loss have hearing impairment as the first symptom, and some having ear distending sensation as the first symptom or major accompanied symptom are often misdiagnosed or missed or treated as eustachian tube obstruction, secretory otitis media or Meniere's syndrome[22]. Studies have shown that there is a certain relationship between ear stuffiness and low-frequency sensorineural hearing loss[23]. We believe that elderly patients with sensorineural deafness usually suffer from hearing loss and tinnitus resulting from long-term inner ear ischemia, hypoxia, and microcirculatory disturbances, which are also the main causes of ear stuffiness or distension in elderly patients[24]. Studies have shown that acupuncture, auricular acupoint sticking and acupoint injection can improve inner ear ischemia, hypoxia and microcirculation to improve hearing loss and tinnitus[25-26], and thus symptom of ear distending sensation can be improved. In clinical treatment certain medication is used to improve the inner ear microcirculation, besides treatment methods such as hormonal drugs, neurotrophic drugs and hyperbaric oxygen therapy must also be considered.Clinical study by Sakata T, et al[27]found that though there was little correlation between ear distending sensation and auditory function, the improvement of symptom of ear distension could indicate a good prognosis. Questions such as the relationship between ear distending sensation and the mechanism of hearing loss in sensorineural deafness need to be further studied[28].
In summary, the randomized controlled trial approved that the relief of ear distending sensation often occur with hearing recovery. The clinical efficacy of hearing loss in those who had ear distending sensation was higher than that of those without ear distending sensation. Its significance for clinical works requires further research and discussion.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
Acknowledgments
This work was supported by Project of Shanghai Municipal Commission of Health and Family Planning (上海市卫生和计划生育委员会课题, No. ZYJX-2017023);Guidance Project of Traditional Chinese Medicine of Shanghai Science and Technology Committee (上海市科学技术委员会中医引导项目, No. 14401932900); Key Project of Shanghai Science and Technology Committee(上海市科学技术委员会科研重点项目,No.16401970300); Lu’s Acupuncture Ⅰnheritance Study of Shanghai Schools of Traditional Chinese Medicine,Shanghai Municipal Commission of Health and Family Planning (上海市卫生和计划生育委员会海派中医流派“陆氏针灸”传承研究项目, No. ZY3-CCCX-1-1007).
Statement of Informed Consent
Ⅰnformed consent was obtained from the patients in this study.
Received: 25 September 2017/Accepted: 29 October 2017
猜你喜欢
浙江中医杂志(2022年7期)2022-12-12
戏曲研究(2022年1期)2022-08-26
中小学校长(2021年7期)2021-08-21
环球中医药(2021年4期)2021-04-26
学生导报·初中版(2020年1期)2020-05-03
戏曲研究(2019年3期)2019-05-21
非遗传承研究(2018年2期)2018-10-14
江西中医药大学学报(2018年2期)2018-02-11
车迷(2017年12期)2018-01-18
上海戏剧(2017年11期)2017-11-16
 Journal of Acupuncture and Tuina Science2018年4期
Journal of Acupuncture and Tuina Science2018年4期
- Journal of Acupuncture and Tuina Science的其它文章
- Therapeutic efficacy observation on acupuncture for persistent allergic rhinitis
- Observation of therapeutic effects of point application at Shenque (CV 8) plus moxa-salt hot compress for prevention of gastrointestinal adverse reactions after chemotherapy for non-Hodgkin lymphoma
- Effects of acupuncture on ovarian blood supply and pregnancy outcomes in patients receiving assisted reproduction
- Effect of Governor Vessel-unblocking and mindrefreshing acupuncture plus functional training on neural development in infants with brain damage
- Clinical observation of abdominal acupuncture for subhealth insomnia
- Application and exploration of suspended magnetic moxibustion cup for obesity