
Fatal Legionella pneumophila serogroup 1 pleural empyema:A case report
2019-02-26 02:42
François Maillet,Nicolas Bonnet,Yacine Tandjaoui-Lambiotte,Intensive Care Unit,Avicenne Hospital,Assistance Publique – Hôpitaux de Paris,Bobigny 93000,France
Nicolas Bonnet,Paris XIII University,Bobigny 93000,France
Typhaine Billard-Pomares,Microbiology Department,Avicenne Hospital,Assistance Publique– Hôpitaux de Paris,Bobigny 93000,France
Fatma El Alaoui Magdoud,Microbiology Department,Jean Verdier Hospital,Assistance Publique–Hôpitaux de Paris,Bondy 93140,France
Abstract
Key words:Legionella pneumophila serogroup 1; Legionellosis; Legionnaire's disease;Pleural empyema; Case report
INTRODUCTION
Legionella pneumophila(L.pneumophila) is a Gram-negative,slow-growing intracellular bacillus,originally discovered in 1976 in Philadelphia among the delegates of the American Legion conference[1].Since then,sixteen different serogroups have been described,with a large predominance of serogroup 1,responsible for approximatively 85% of the cases[2].Risk factors for infection include male sex,aged more than 50 years,current or historical smoking,alcohol abuse,diabetes,cancer,chronic kidney failure,iron overload and immunocompromising diseases or treatments[3].Although it is mostly known to cause acute severe pneumonia,with frequent parapneumonic pleural effusion,L.pneumophilainfection may rarely cause pleural empyema.
We report here a case of pleural empyema caused byL.pneumophilaserogroup 1 in an immunocompromised patient,followed by a review of the literature.
CASE PRESENTATION
Chief complaints
In august 2018,an 81-year-old caucasian man presented to the emergency department with fever,progressive dyspnea,dry cough and left pleuritic chest pain.
History of present illness
Patients symptoms started 3 wk ago and worsened progressively.
History of past illness
His medical history was consistent with chronic lymphocytic leukemia,initially treated in 2007 with Fludarabine,Cyclophosphamide and Rituximab therapy with chronic lymphocytosis,type 2 diabetes mellitus,hypertension,hyperlipidemia and chronic kidney failure with an eGFR of 28 mL/min/1.73 m2.He reported no smoking or alcohol abuse and used to work as an upholsterer.
Personal and family history
None.
Physical examination upon admission
Physical examination revealed fever (38.1°C),tachycardia (105 bpm),peripheral percutaneous oxygen saturation was 100% with 2 liters of oxygen with tachypnea,normal blood pressure and almost abolished left vesicular murmur.Adenopathy,hepatomegaly or splenomegaly were not observed.Cardiovascular and neurologic examination were normal.
Laboratory examination
Biology tests revealed neutrophilia (18.7 g/L) and elevated CRP (297 mg/L)consistent with inflammatory response,along with stable lymphocytosis (242 g/L)and anemia (7.8 g/L).
Imaging examination
Chest X-ray at admission (Figure1) showed a large left pleural effusion with contralateral tracheal deviation.Complementary computed tomography (Figure2)confirmed a walled-off,loculated left pleural effusion,with right lung parenchyma considered normal.
Further diagnostic work-up
First bedside pleural puncture showed a citrine exudate (pleural protein 37 g/L,pleural fluid protein to serum ratio 0.61),unfortunately cytological examination was not performed.
Despite intravenous treatment with cefotaxime,the patient condition worsened with persistence of fever,neutrophilia,and severe hypoxemia appeared.Bacteriological standard culture of the pleural liquid sample was negative,as well as repeated blood cultures.In order to look for a tuberculosis etiology,auramine stained sputum smears and cultures were performed but remained negative.Spot-test for tuberculosis was not performed.Ten days after his admission,because of the uncontrolled large pleural effusion with acute hypoxemic respiratory failure,the patient underwent surgical thoracentesis with evacuation of 2 liters of purulent liquid.We chose surgery instead of repeated pleural drawings,because local sepsis was not controlled nor bacteriologically documented.Pleura was thick and nodular,with white pseudo-membranes.Treatment with metronidazole was added to cefotaxime after the surgery in order to cover anaerobic bacteria.Cytobacteriological examination and cultures of the liquid were negative.Lymphocyte phenotyping ruled out B-cell lymphoma as a complication of his chronic lymphocytic leukemia.Three days after,the patient progressively developed multiple organ failure requiring intensive care unit admission.As no massive transfusion was initiated during surgery and shock was the main matter,fluid overload could not explain the evolution in multiple organ failure.After a slow unfavorable evolution during the ten first days of hospitalization,the patient's condition worse brutaly three days after surgical thoracocentesis leading to septic shock complicated of multiple organ failure.Despite antibiotherapy with cefepime and amikacin,invasive mechanical ventilation,vasopressor infusion and renal replacement therapy,the patient died of uncontrolled septic shock few hours after ICU admission.
The day after,mycobacterial culture of surgical pleural samples yielded Gramnegative bacilli (Figure3).Rapid identification using matrix-assisted desorption ionization–time of flight mass spectrometry (MALDI-TOF MS; Microflex LT; Bruker Daltonics,Leipzig,Germany) was performed andL.pneumophilawas identified.The bacteria were addressed to the National Reference Center of Legionella and molecular typing analysis by sequence-based typing was performed and showed that the strain ofL.pneumophilaserogroup 1 belonged to Sequence Type 1.Urinary antigen research retrospectively performed on a urine sample of the patient confirmed the presence ofL.pneumophilaserogroup 1.
We believe that chances of super infection or co-infection with another bacterium are scarce.Patient indeed received broad spectrum antibiotics directed against common bacteria causing pleural empyema (including anaerobic bacteria,gramnegative bacillus,streptococci and staphylococci),and repeated standard bacteriological cultures remained negative.
Retrospectively,our patient presented the following risk factors:Male sex,aged more than 50 years,chronic lymphocytic leukemia with history of immunocompromising treatments,chronic kidney failure,diabetes mellitus and weaned smoking.

Figure1 Chest X-ray at admission:Large left pleural effusion with contralateral deviation of the mediastinum.
FINAL DIAGNOSIS
Fatal pleural empyema caused byL.pneumophilaserogroup 1.
TREATMENT
No specific treatment could have been introduced because of post-mortem diagnosis.Unfortunately,theL.pneumophilastain identified in our patient was naturally resistant to all the antibiotics received.
OUTCOME AND FOLLOW-UP
Patient died of uncontrolled sepsis caused byL.pneumophilaserogroup 1 pleural empyema.
DISCUSSION
Pleural effusion is a common manifestation of Legionnaire's disease.In a case series of 36 microbiologically proven legionellosis,Sakaiet al[4]reported in 2007 unilateral or bilateral scannographic pleural effusion in 60% of pneumonia caused byL.pneumophila,considered as a parapneumonic aseptic transudate.Similarly,Poirieret al[5]reported in 2017,in a 33 individuals canadian cohort,a scannographic frequency of 66% (22/33).In contrast,pleural empyema,defined as a septic exudate with presence ofL.pneumophila,seems exceptional.
Prevalence of pleural empyema in legionellosis is largely unknown.Since 1979,only 11 cases have been reported.These cases involved mostly men with an age ranging between 36 and 83[6-12].L.pneumophilaserogroup 1 seems to be involved in most cases,but one serogroup 5 nosocomialL.pneumophilahas been described in a patient following esophageal perforation after esophageal dilatation for carcinoma[6-8].All infected patients with detailed history presented classic risk factors:Tobacco use,relative immunosuppression caused by advanced age,high-dose steroids as a treatment for systemic lupus erythematosus[9],immunosuppressive drugs in a kidney transplant recipient[10].In 1981,Winn and Myerowitz reported two necropsias of fatal legionellosis with unilateral empyema with presence ofL.pneumophilain pleural fluid[11].Characteristics of pleural liquid,available for six cases,seem to be those of a classic empyema:Macroscopically purulent or serofibrinous,elevated LDH (5 out of 5,1 non tested,range 342-2371 UI/L) and proteins (6 out of 6,range 31-57 g/L),with a predominance of neutrophils (6 out of 6),with hypoglycopleuria and acid pH.
L.pneumophilainfection is associated with a poor outcome:In a retrospective study of 136 consecutive cases of communautaryL.pneumophilainfection in Spain between 2001 and 2015,85% of patients were hospitalized,including 11.7% in intensive care unit,and the mortality rate was 4.4%[13].Of the 11 patients described,2 died with unrecorded treatment,7 patients survived with adequate antibiotic course,and the outcome of the 2 last was unknown.Choice of antibiotic stewardship and duration of antibiotic course for pleural legionellosis is widely empirical:4 patients received a 4 wk course of IV erythromycin,2 received a combination of erythromycin and rifampicin during 8 wk,and the last one was treated with levofloxacin for an undetermined duration of time.

Figure2 Computed tomography of the chest at admission:Multiloculated left pleural effusion
Early identification of sepsis and early administration of adapted antibiotherapy is now recommended by international clinical practice guidelines[14].In our case report,identification of sepsis and its pleural origin was easy.Unfortunately,empirical antibiotherapy did not coverLegionellosis,and probably led to the patient's death.
Extrapulmonary legionellosis is a very challenging diagnosis and might involve many different organs[15-18].In patients with immunocompromising conditions,L.pneumophilacan cause septic arthritis,endocarditis,myocarditis,myositis or cutaneous involvement,including panniculitis,exanthema,subcutaneous nodules,pustules or even abscesses.OtherLegionellaspecies include,among others,L.bozemanii,andL.micdadei[2].These other species,much rarer thanL.pneumophila,can also exceptionally cause pneumonia with pleural empyema,which seems to be overrepresented compared toL.pneumophila[19,20].Mycoplasma pneumonia,another intracellular bacteria known to cause pneumonia,has also been reported a few times as the causative agent of pleural empyema[21].
CONCLUSION
Although uncommon,pleural empyema caused byL.pneumophilais associated with a poor outcome,and is therefore a very challenging diagnosis.We suggest that Legionnaire's disease should be considered in patients with multiple risk factors and pleural empyema with negative bacteriological standard culture and unresponsive to conventional antibiotherapy.
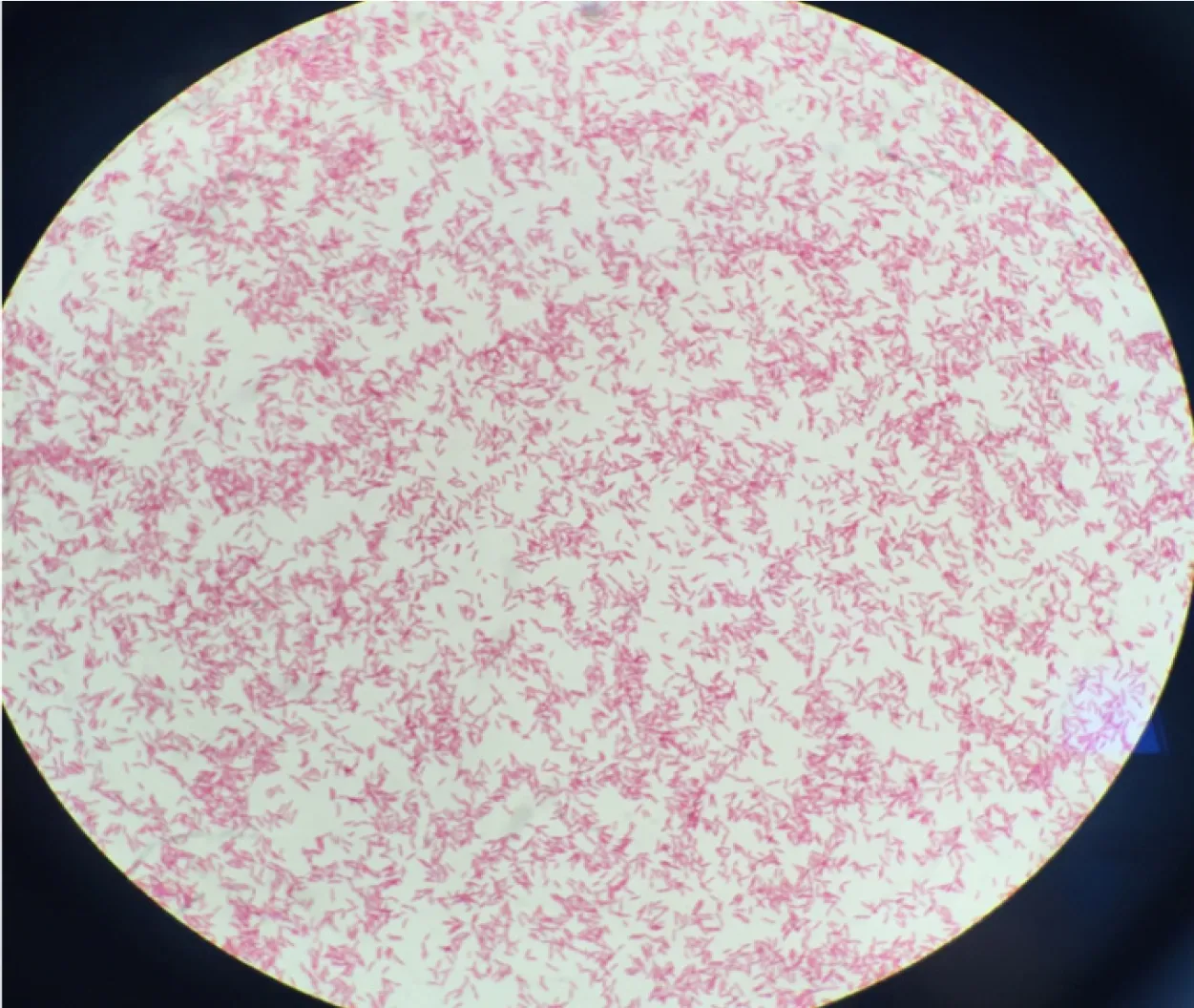
Figure3 Gram staining of pleural culture confirmed gram-negative bacillus,consistent with Legionella pneumophila.
ACKNOWLEDGEMENTS
The authors would like to thank Laetita Beraud,from the French National Reference Center for Legionella,for her work in the identification of serogroup 1Legionella pneumophila.
 World Journal of Critical Care Medicine2019年6期
World Journal of Critical Care Medicine2019年6期
- World Journal of Critical Care Medicine的其它文章
- Anticoagulation with direct thrombin inhibitors during extracorporeal membrane oxygenation