
Incidence of portal vein thrombosis after splenectomy and its influence on transjugular intrahepatic portosystemic shunt stent patency
2019-03-14 04:17FangDongShiHuaLuoLiJuanZhengJianGuoChuHeHuangXueQiangZhangKeChunYao
World Journal of Clinical Cases 2019年17期
Fang Dong,Shi-Hua Luo,Li-Juan Zheng,Jian-Guo Chu,He Huang,Xue-Qiang Zhang,Ke-Chun Yao
Abstract
Key words: Portal hypertension;Transjugular intrahepatic portosystemic shunt;Splenectomy;Portal vein thrombosis
INTRODUCTION
Portal hypertension secondary to liver cirrhosis is mainly due to chronic hepatitis and alcoholic liver disease[1].Esophagogastric varices and ascites secondary to portal hypertension are common major complications of liver cirrhosis[2].Esophagogastric varices are a serious,life-threatening complication and hypersplenism is often associated with portal hypertension in cirrhotic patients[3].
There are several approaches for treatment of portal hypertension related varices and variceal hemorrhage,including drugs,endoscopic variceal ligation,transjugular intrahepatic portosystemic shunt (TIPS),splenectomy with pericardial devascularization (SPD) and liver transplantation[4].SPD without liver transplantation has been widely accepted as a surgical treatment for cirrhosis in patients with variceal bleeding and secondary hypersplenism in China for many years[5].However,when compared with other treatments,simple splenectomy and SPD are associated with an increased incidence of postoperative complications,such as portal vein thrombosis(PVT)[6].
TIPS is widely accepted as an alternative to surgery for management of complications of portal hypertension such as variceal bleeding,refractory ascites,Budd-Chiari syndrome,hepatorenal syndrome,hepatic hydrothorax and even hepatopulmonary syndrome[7].TIPS has been used to effectively treat PVT in many centers since the 1990s[8].PVT is still considered a contraindication to the creation of a TIPS,however the advantages of TIPS for PVT in patients with cirrhosis are evident[9]as it addresses portal hypertension and reconstructs portal vein (PV) flow.
Despite its efficacy in treatment of complications of portal hypertension,TIPS is prone to shunt stenosis or occlusion leading to shunt failure,and approximately half of all patients with TIPS require shunt revision during follow-up[10],which makes close surveillance and frequent costly revisions mandatory[11]especially in patients with PVT despite the use of stent grafts covered with polytetrafluoroethylene.Even with these new stents,post-TIPS shunt obstruction and a high rate of clinical symptom recurrence remain problematic.
Although TIPS has good therapeutic effects on the formation of PVT,the effect of PVT on TIPS stenting has rarely been reported.The purpose of this study was to evaluate the incidence of PVT after splenectomy and its influence on the patency rate of TIPS in patients with cirrhosis of portal hypertension.
MATERIALS AND METHODS
Patients
A total of 486 patients who underwent a TIPS procedure between January 2010 and January 2016 were enrolled retrospectively.The study protocol was approved by the Institutional Review Board and Ethics Committee,and all the patients provided a written consent at the time of operation in the hospital.All procedures were conducted according to the guidelines approved by the ethics committee.We reviewed the patients’ medical records and medical images to gather information regarding the underlying etiologies,clinical presentations,age,sex and severity of cirrhosis.
Study design
This was a multi-center,retrospective study.Patients with cirrhosis without prior splenectomy served as group A (n= 289),and those with cirrhosis and prior splenectomy served as group B (n= 197).Three hundred and sixty-five patients with portal-hypertension-related complications of recurrent variceal bleeding after band ligation and/or glue injection,121 patients with refractory ascites and 86 with both who underwent TIPS were included.The incidence of PVT before TIPS was compared between the two groups.After TIPS placement,primary patency rate was compared at 3,6,9 and 12 mo,and 2 and 3 years.The clinical outcomes were analyzed.
Patients with acute PVT,variceal bleeding as an emergency indication,hepatic encephalopathy (HE),severe right-sided heart failure,severe liver failure,polycystic liver disease,dilated biliary ducts,age > 75 years,Child-Pugh score > 11,Model for End-stage Liver Disease score > 18,hepatic carcinoma,sepsis or spontaneous bacterial peritonitis and patients who underwent liver transplantation were excluded.
Diagnosis and definitions
Color Doppler ultrasound was performed initially for the diagnosis of PVT.It revealed that the main PV was obstructed along with a reduction or absence of portal flow or disappearance of the native PV and formation of extensive collaterals.Contrast-enhanced computed tomography and/or magnetic resonance imaging showed stenosis,filling defects or complete occlusion of the PV with or without collaterals.
Acute PVT was defined by the absence of collateral vessels and any one of the following:(1) Aapid onset of abdominal pain due to PVT within 14 d and intestinal ischemia or infarction without chronic thrombosis;or (2) A high intraluminal density within the PV on non-contrast-enhanced computed tomography.Chronic PVT was defined by at least one of the following:(1) A low intraluminal density on contrastenhanced computed tomography;(2) Replacement of the original main PV (MPV)with a fibrotic cord or no identifiable MPV;or (3) Presence of portal cavernoma.Thrombosis in the MPV was further classified as partial occlusion,complete occlusion and fibrotic cord in place of the original MPV.
TIPS procedure
Direct portography was then performed to confirm if the PV system was entirely patent.After the TIPS procedure,patients were treated with intravenous heparin(4000 U/d;Chase Sun Pharma Co.Ltd,Tianjing,China) and oral warfarin (2.5 mg/d;Orion Pharma Co.Ltd,Orionintie,Finland).
Follow-up
Patients underwent baseline duplex sonography on the day after TIPS.The results were compared with subsequent shunt velocities.After TIPS,patients were followed up using the same protocol for each groupviaoutpatient visit 1 mo after the procedure and then every 3 mo or whenever needed.Clinical examination,blood chemistry test and assessment of HE were carried out during the follow-up period.Ultrasonography was also performed after TIPS or in case of recurrent bleeding or ascites.
Shunt dysfunction or significant recurrent symptoms were used as endpoints for the loss of primary unassisted patency.TIPS angiography was performed in these patients and TIPS revision was made when hemodynamically significant shunt stenosis was > 50% with recurrent variceal bleeding and ascites,and portosystemic pressure gradient was ≥ 15 mmHg without grade III/IV HE (West Haven Criteria)
Statistical analysis
Results are expressed as mean ± SD.Patency time was calculated by the Kaplan-Meier method,and the median time was compared by the log-rank test.Variables were subjected to logistic regression analysis.Differences between the groups were compared using one-way analysis of variance and least significant differencettest.P< 0.05 was considered statistically significant.SPSS version 20.0(SPSS,Chicago,IL,United States) was used for the statistical analysis.
RESULTS
Between January 2010 and January 2016,there were 289 patients with cirrhosis with no prior splenectomy in group A,and 197 patients with cirrhosis who underwent splenectomy in group B.The etiology,clinical presentations,age,sex and severity of cirrhosis did not differ significantly (Table 1).In group A,the incidence of PVT was 11.0% (65/289).In group B,the incidence of PVT was 44.2% (87/197).The distribution of patients is shown in Figure 1.The incidence of PVT in group B was higher than in group A,and the difference was significant between the two groups (P= 0.003).
Of the 289 patients in group A,255 (88.2%) cases had technically successful TIPS compared with 144 (73.1%) cases in group B.TIPS technical success rate in group A was higher than in group B (P= 0.016).No patient died of severe procedure-related complications within 30 d after TIPS (Figure 2).After TIPS,the mean portosystemic pressure gradient decreased from 32.43 ± 6.64 to 11.15 ± 1.20 mmHg in group A (P=0.027),and 31.90 ± 4.63 to 10.79 ± 1.18 mmHg in group B (P= 0.025).There were significant differences before and after TIPS (P< 0.05),but there was no difference before and after TIPS between the two groups (P= 0.447,P= 0.605,respectively)(Table 2).
The primary patency rate for group A was 97.6% at 3 mo,88.6% at 6 mo,84.3% at 9 mo,69.4% at 12 mo,51.0% at 2 years and 30.6% at 3 years.In group B,the patency rate was 88.1% at 3 mo,78.7% at 6 mo,68.1% at 9 mo,45.1% at 12 mo,26.4% at 2 years and 12.5% at 3 years.Compared with the two groups,there were significant statistical differences at the time 3 mo,6 mo,9 mo,12 mo,2 year and 3 year (P= 0.006,P= 0.011,P= 0.023,P= 0.032,P= 0.037,P= 0.028,respectively).The median patency time of the total 3 years was 12 mo in group A (95% confidence interval (CI):10-14) and 4 mo in group B (95%CI:3-6),and a significant difference was observed in stent dysfunction times between groups A and B (P= 0.009,log-rank test) (Table 3).
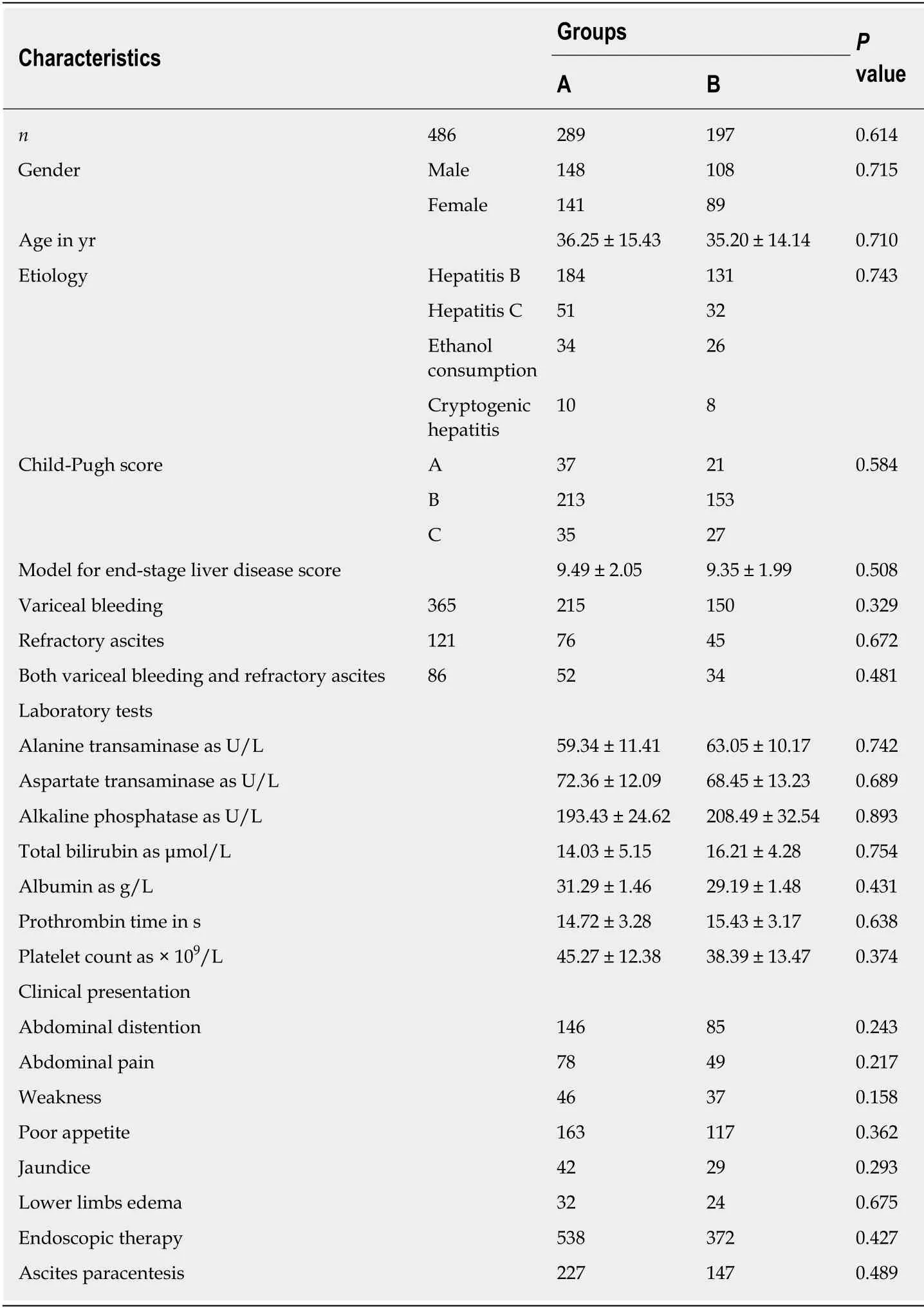
Table1 Demographic characteristics of the patients
Total shunt malfunction occurred 378 times of 289 patients in group A and 419 times of 197 patients in group B.There was a significant difference in stent dysfunction times between groups A and B (P= 0.006,log-rank test).The patients with stent dysfunction underwent balloon dilation.After stent revision,their symptoms disappeared.
政府购买服务模式适用于内河码头。这些区域船舶规模小、船员环保意识差,在现阶段需要由政府提供船舶污染物接收处置的公共服务,而政府出资签约民营单位提供公共服务的做法符合我国政府改革的方向。通常政府购买服务模式的地区实行船舶污染物免费接收的政策。
Incidence of recurrent bleeding (Table 4) and ascites (Table 5) in group B was higher than in group A at 3 mo (14.6%vs5.1%,P≤ 0.001;16.7%vs5.9%,P= 0.001),6 mo (25.7%vs9.8%,P= 0.003;24.3%vs10.2%,P= 0.005),9 mo (29.8%vs15.3%,P=0.005;35.4%vs20.0%,P= 0.012),12 mo (39.6%vs20.0%,P= 0.008;43.8%vs34.1%,P=0.024),2 years (45.1%vs29.0%,P= 0.011;39.6%vs27.8%,P= 0.018) and 3 years (59.7%vs40.0%,P= 0.016;56.3%vs40.8%,P= 0.017).
The median time to recurrent bleeding was 10 mo in group A (95%CI:8-12) and 5 mo in group B (95%CI:4-7).The median time to recurrence of ascites was 11 mo in group A (95%CI:6-16) and 16 mo in group B (95%CI:12-19).There were significant differences in median time to recurrent bleeding and ascites between the two groups(P= 0.009,P≤ 0.001,log-rank test).
During the 3-year follow-up,the 1-year survival rate was 92.9%versus85.4%,2-year survival rate was 83.9%versus68.1%,and 3-year survival rate was 69.4%versus56.3%in group A and group B.Compared with group B,the 1-,2-,and 3-year survival rates in group A were longer (P= 0.008,P= 0.021 andP= 0.011,respectively) (Table 6)(Figure 3).
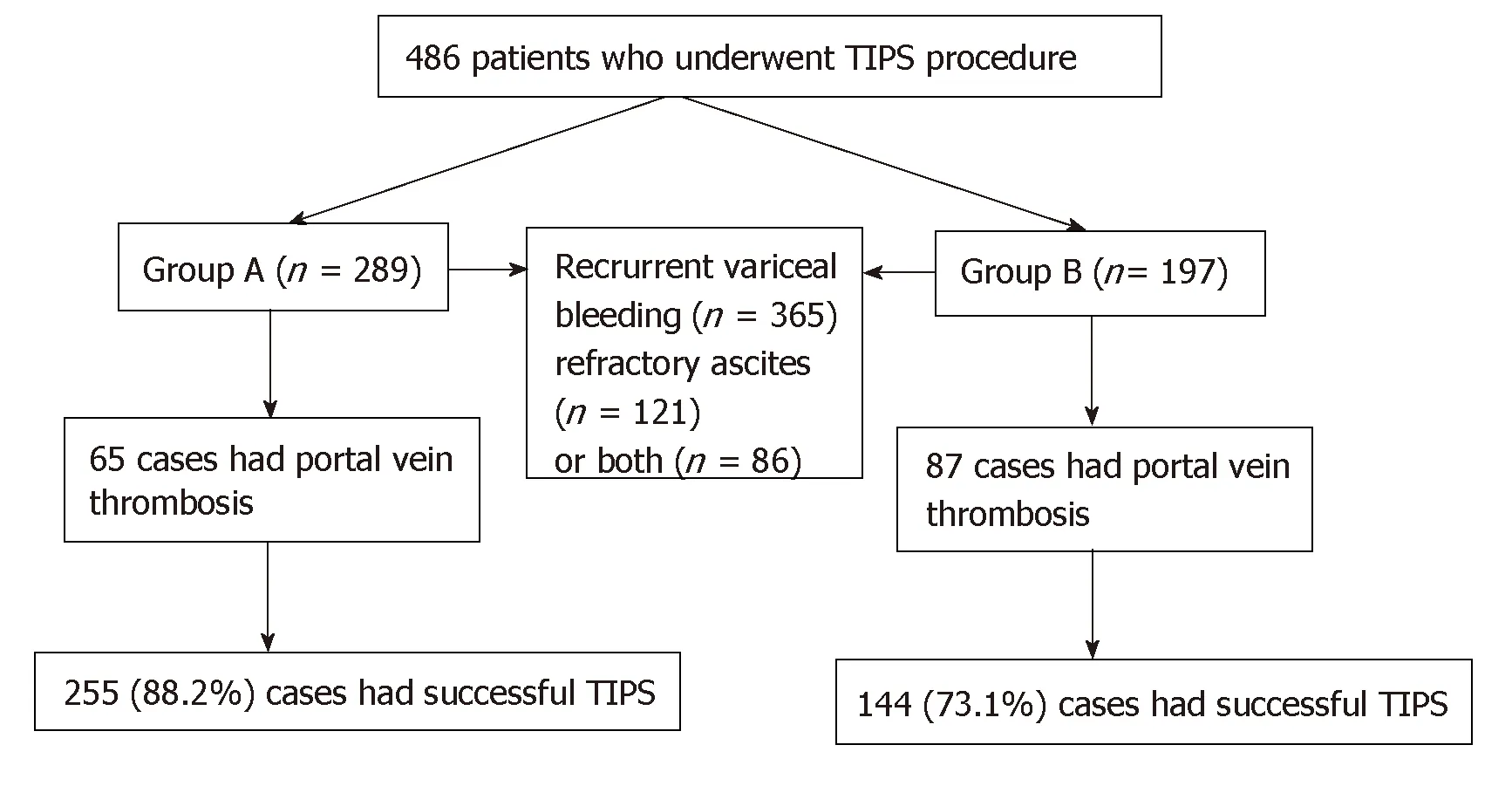
Figure1 Distribution of patients.
HE occurred in 70 patients in group A and in 35 patients in group B during followup with an incidence of 27.5% and 24.3%,respectively.There were no significant differences between the groups (P= 0.527).After drug treatment,the symptoms disappeared in patients with grade overt and grade II of HE.In patients with grade III and grade IV of HE,the symptoms disappeared after 18 stents were implanted for shunt reduction.
DISCUSSION
Portal hypertension is a consequence of liver cirrhosis;the mechanisms by which it develops are complicated and associated with changes in the vascular architecture of the liver due to fibrosis and regenerative nodules[14].Surgical treatments have been designed to prevent many complications.Currently,SPD is the most commonly used method in China[15].SPD is one of the common treatment methods for patients with cirrhosis with portal-hypertension-related complications and hypersplenism[16]and can correct hypersplenism and reduce PV blood flow and pressure within a short period of time[17].
However,the availability of many treatment methods suggests that no one in particular yields entirely satisfactory outcomes for all patients or in all clinical situations[18].Splenectomy in patients with portal hypertension does not resolve the risk of PVT,and it can further aggravate portal hypertension,cause PVT,increase the probability of rebleeding and ultimately affects quality of life[19,20].In the study of resection of spleen,reduction of portal venous pressure depends on the splenic venous blood reflux and portal venous shunt.Resection of the communicating branches from the splenic hilus will cause increased portal venous pressure and portal venous thrombosis.
The incidence of PVT is mostly 12%-72% after splenectomy or SPD,and the risk factors for PVT after splenectomy have been studied[21,22].Patients with portal hypertension were seeking TIPS treatment in our center.However,it has been found that the probability of PVT is significantly increased after splenectomy.This highlights the difficulties in the TIPS procedure,and it also affects the patient prognosis and the effect of liver transplantation.We found that the total incidence of PVT after splenectomy was 44.2%,which was higher in the splenectomy group than that in the group without splenectomy.
TIPS creation has been widely used in the treatment of patients with esophageal and gastric variceal bleeding secondary to portal hypertension and has achieved good results[23,24].With the improvement of procedure methods and instruments,the incidence of complications after TIPS has greatly decreased.Although being effective in preventing such syndromes,TIPS may cause shunt stenosis or occlusion leading to shunt failure.Stent stenosis and occlusion are the main complications of TIPS placement and cause recurrent bleeding and ascites[25].
There are multiple causes of thrombosis after splenectomy.It is believed that splenectomy reduces synthesis of coagulation factors in patients with liver cirrhosis,and the scavenging activity of tissue plasminogen activator is decreased resulting in a high blood coagulation state[26].In addition,the risk of PVT after splenectomy can be caused by lack of microcirculation,increased blood viscosity,blood stasis induced by splenic vein stump,decreased blind pouch postoperative PV pressure,slower blood flow and platelet count[27,28].The presence of these factors can lead to the formation of PVT and have a continuous impact on the PV system despite treatment with TIPS.It is also easy to cause thrombosis in the TIPS shunt and PV system and to cause stenosis or occlusion of the TIPS shunt,and these factors promote each other.

Table2 Clinical characteristics of the patients
PVT can develop in the trunk of the PV,including its right and left intrahepatic branches,or it can originate everywhere in the portal system and may even extend to the splenic or superior mesenteric veins or towards the liver involving the intrahepatic PV branches[29].PVT leads to portal hypertension and cavernous transformation of the PV,which causes difficulty with TIPS creation[30].Although TIPS has good therapeutic effects on the formation of PVT,the effect of PVT on TIPS stenting is rarely reported.
In our study,the incidence of PVT in group A was lower than in group B,and the success rate of TIPS placement was also higher in group A.Our results indicated that PVT easily forms after splenectomy as described previously,and it creates difficulty for treatment with TIPS and other methods.The patency rate after TIPS in group A was higher than in group B,the median unassisted patency time in group A was longer than in group B,and recurrent bleeding and ascites in group A were less than in group B.Our results confirmed that prior splenectomy is an important determinant of shunt patency.
It is reported[31]that after TIPS treatment,hypersplenism is relieved due to decreased PV pressure and splenic blood flow,which can improve quality of life.However,there are still some patients with hypersplenism with no satisfactory outcome of treatments,including partial splenic arterial embolization,which can improve the symptoms of hypersplenism[32,33].In patients with cirrhosis who are prone to PVT,which can lead to difficulty with TIPS creation and stent stenosis or occlusion,we suggest that splenectomy should be considered carefully.
The present study has some limitations.TIPS was established by the left branch of the intrahepatic PV,which may affect the results of patency rate.This is only a retrospective study.Randomized controlled trials are needed to verify our results.
In conclusion,patients with portal hypertension with prior splenectomy had a high incidence of PVT,which is an important determinant of TIPS stent patency and potentially increases the risk of recurrent symptoms associated with shunt stenosis or occlusion.Patients with portal hypertension have the opportunity to avoid splenectomy if they are undergoing TIPS treatment.

Table3 Clinical characteristics of the patients in stent primary patency rate

Table4 Clinical characteristics of the patients in recurrent bleeding rate
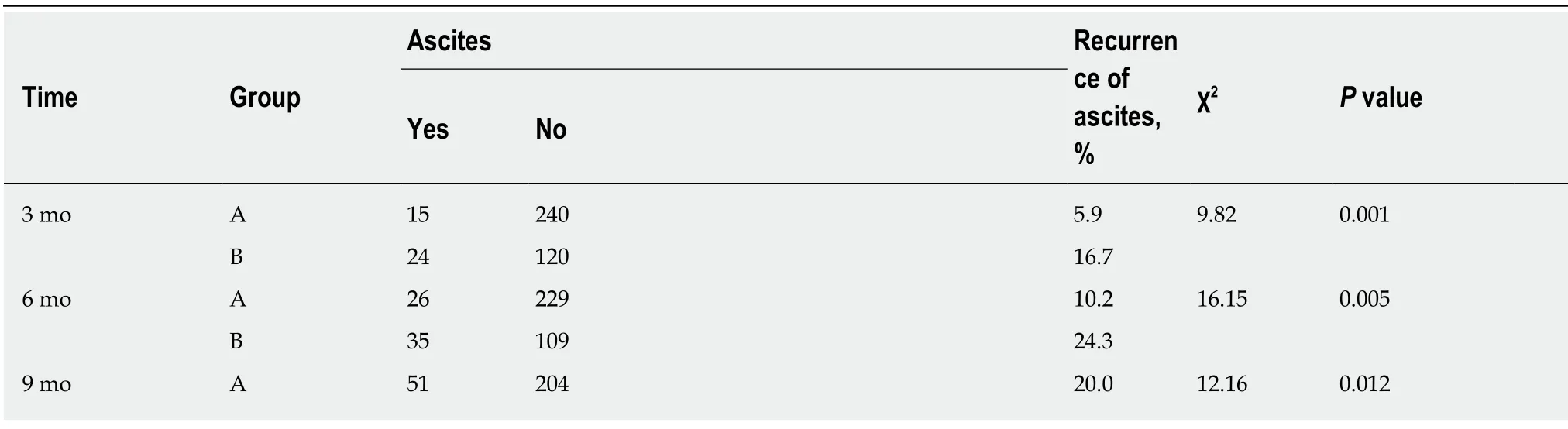
Table5 Clinical characteristics of the patients in recurrence of ascites

51 93 35.4 12 mo A 87 168 34.1 4.50 0.024 B 63 81 43.8 2 yr A 71 184 27.8 6.56 0.018 B 57 87 39.6 3 yr A 104 151 40.8 10.02 0.017 B 81 63 56.3 Median recurrent of ascites in mo Four quantile spacing in mo Total 3 yr A 11 (6,16) 0.009 B 16 (12,19)B

Table6 Clinical characteristics of the patients in survival rate and incidence of hepatic encephalopathy

Figure2 Decompensative liver cirrhosis and portal vein thrombosis treated with transjugular intrahepatic portosystemic shunt.
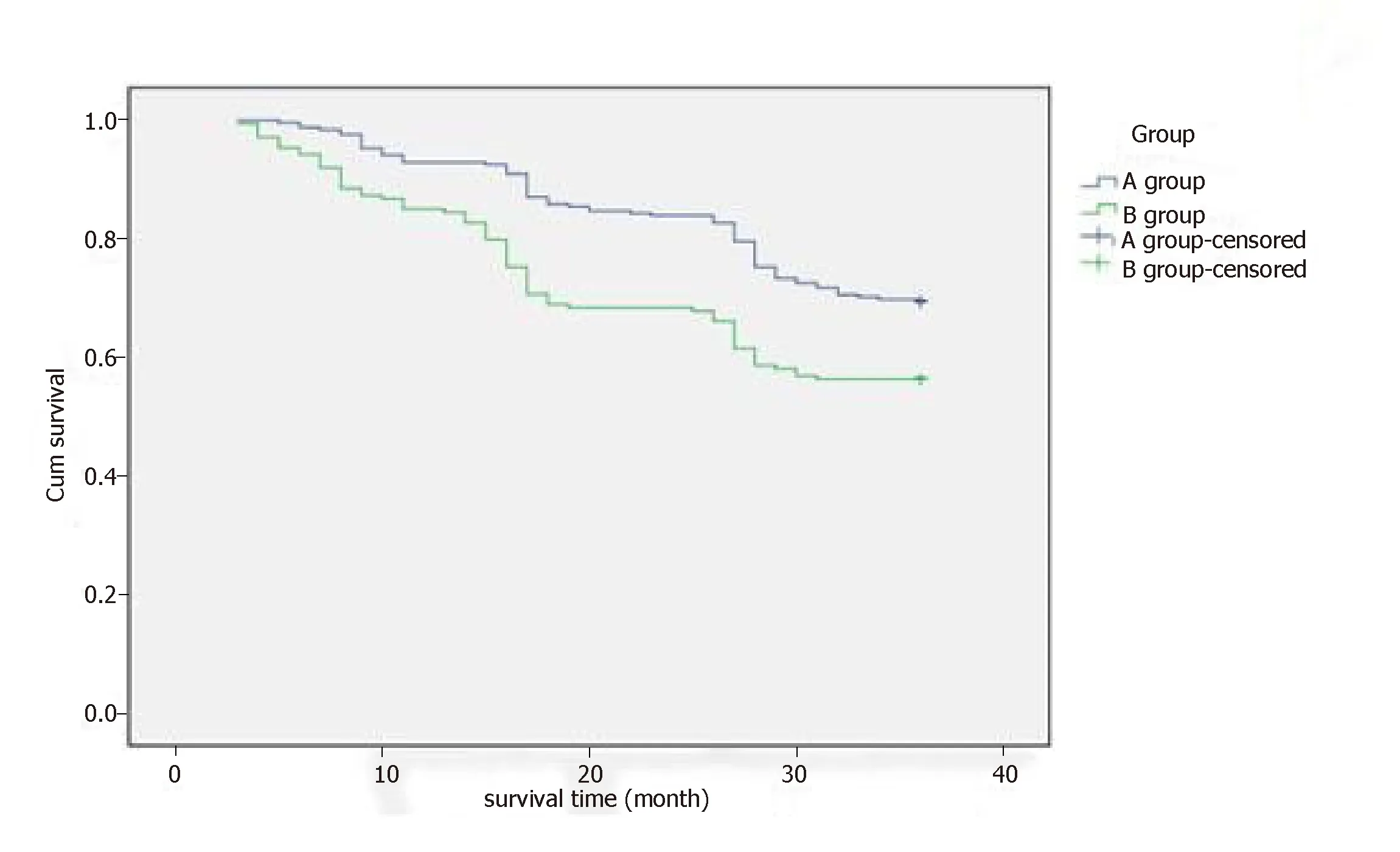
Figure3 Survival time.
ARTICLE HIGHLIGHTS
Research background
Splenectomy with pericardial devascularization (SPD) without liver transplantation has been widely accepted for the treatment of cirrhosis in patients with variceal bleeding and secondary hypersplenism in China.However,when compared with other treatments,simple splenectomy and SPD are associated with an increased incidence of postoperative complications,such as portal vein thrombosis (PVT).Transjugular intrahepatic portosystemic shunt (TIPS),as an alternative to surgery,is now commonly used for management of complications of portal hypertension.Patients with SPD had a high incidence of PVT,which can markedly affect TIPS stent patency and increase the risk of recurrent symptoms associated with shunt stenosis or occlusion.
Research motivation
SPD is one of the common treatment methods used in China for patients with cirrhosis and portal-hypertension-related complications and hypersplenism.It can correct hypersplenism and reduce PV blood flow and pressure within a short period of time.However,it may aggravate the portal hypertension,cause PVT,increase the probability of rebleeding and ultimately affects quality of life.In this study,we evaluated the incidence of PVT after splenectomy and its influence on the patency rate of TIPS in patients with cirrhosis and portal hypertension.
Research objectives
The main objective of this study was to investigate the effects of high incidence of PVT in patients with portal hypertension and prior SPD on the TIPS stent patency and the risk of recurrent symptoms associated with shunt stenosis or occlusion.
Research methods
We conducted a retrospective study to compare the incidence of PVT before TIPS for patients without prior SPD (group A) and those with prior SPD (group B).After TIPS placement,primary patency rate was compared using Kaplan-Meier analysis at 3,6,9 and 12 mo,and 2 and 3 years.The clinical outcomes were analyzed.Results are expressed as mean ± SD.Patency time was calculated using the Kaplan-Meier method,and the median time was compared by means of the log-rank test.Logistic regression analysis was performed on the variables.The differences between the groups were compared using one-way analysis of variance followed by least significant differencettests.Differences were considered significant atP< 0.05.The statistical analysis was performed with SPSS version 20.0 (SPSS,Chicago,IL,United States).
Research results
The incidence of PVT in group B was higher than in group A,and the difference was significant between the two groups (P= 0.003).The success rate of TIPS in group A was higher than in group B,and the primary patency rate in group A tended to be higher than in group B at 3,6,9 and 12 mo,2 years and 3 years.Recurrence of bleeding and ascites rate in group A were lower than in group B at 3 mo,6 mo,9 mo,12 mo,2 years and 3 years.During the 3-year follow-up,the 1-,2- and 3-year survival rates in group A were higher than in group B,but there was no difference of the incidence of hepatic encephalopathy.
Research conclusions
Patients with a SPD have a high incidence of PVT,which potentially increases the risk of recurrent symptoms associated with TIPS stenosis or occlusion.
Research perspectives
This study showed that patients with portal hypertension with prior splenectomy had a high incidence of PVT,which is an important determinant of TIPS stent patency and potentially increases the risk of recurrent symptoms associated with shunt stenosis or occlusion.Patients with portal hypertension may avoid splenectomy when they are undergoing TIPS treatment.However,this is only a retrospective study,and randomized controlled trials are needed to verify our results.
ACKNOWLEDGEMENTS
We are grateful to all the patients who were involved in this study and our colleagues in the Department of Radiology of Air Force General Hospital of PLA for their contributions to the data collection.
猜你喜欢
水上消防(2021年4期)2021-11-24
消费导刊(2020年35期)2021-01-28
西部交通科技(2021年9期)2021-01-11
中国外汇(2019年19期)2019-11-26
水上消防(2019年3期)2019-08-20
名作欣赏(2017年11期)2017-01-28
航运交易公报(2016年40期)2016-11-22
科学中国人(2016年27期)2016-03-11
商界评论(2015年8期)2015-10-15
环球时报(2013-02-22)2013-02-22
 World Journal of Clinical Cases2019年17期
World Journal of Clinical Cases2019年17期
- World Journal of Clinical Cases的其它文章
- Multifocal G1-G2 gastric neuroendocrine tumors:Differentiating between Type I,II and III,a clinicopathologic review
- Attention deficit hyperactivity disorder and comorbidity:A review of literature
- Dietary manipulation and testosterone replacement therapy may explain changes in body composition after spinal cord injury:A retrospective case report
- Risk factors,clinical features,and short-term prognosis of spontaneous fungal peritonitis in cirrhosis:A matched case-control study
- Multiplex gene expression profile in inflamed mucosa of patients with Crohn’s disease ileal localization:A pilot study
- Analysis of the postoperative hemostatic profile of colorectal cancer patients subjected to liver metastasis resection surgery