
Knowledge, attitude, and practice towards coronavirus disease 2019 (COVID-19) among medical students: A cross-sectional study
2020-05-21 08:03SonamMaheshwariPuneetKumarGuptaRichaSinhaPraveshRawatDepartmentofCommunityMedicineGovernmentDoonMedicalCollegeDehradunIndia
Journal of Acute Disease 2020年3期
Sonam Maheshwari, Puneet Kumar Gupta, Richa Sinha, Pravesh RawatDepartment of Community Medicine, Government Doon Medical College, Dehradun, India
2ICFAI Business School, The ICFAI University, Dehradun, India
3Government Doon Medical College, Dehradun, India
ABSTRACT
KEYWORDS: COVID-19; Noval coronavirus; Knowledge; Attitude; Practice; Social distancing; Lockdown
1. Introduction
In December 2019, a pathogenic human coronavirus SARSCoV-2, coronavirus disease 2019 (COVID-19), was recognized and has caused serious illness and numerous deaths. The ultimate scope and effect of this outbreak are unclear at present as the situation is rapidly evolving[1]. The disease causes respiratory illness (like the flu) with main clinical symptoms such as a dry cough, fever, and in more severe cases, difficulty in breathing. COVID-19 is highly contagious with a certain mortality rate, and it was classified as a class B infectious disease and managed as a class A infectious disease in China in January 2020[2]. China has taken firm infection control measures, isolating the exposed and suspected cases according to international standards, constantly updating the diagnosis and treatment process, and carrying out public education[3].
The epidemics of COVID-19 have been recorded over 200 countries, territories, and areas with 2 878 196 confimed cased and 198 668 death cases[4]. On 11 March 2020, WHO changed the status of the COVID-19 emergency from public health international emergency (30th January 2020) to a pandemic. Nonetheless, the fatality rate of the current pandemic is on the rise (between 2%-4%), relatively lower than the previous SARS-CoV (2002/2003) and MERS-CoV (2012) outbreaks[5].
In India, a confirmed case of COVID-19 was reported on 30th January 2020, who was a student traveled from Wuhan, China, and has successfully recovered from the infection on 14th February 2020[6-8]. On 27th April 2020, the Ministry of Health and Family Welfare confirmed a total of 28 380 confirmed cases, 6 362 cured/discharge cases, and 886 death cases in the country from 32 states/ unioin terrrities[9]. The infection rate of COVID-19 in India is reported to be 1.7%, significantly lower than the worst affected countries, as the report on 29 March 2020[10]. After a 14-hour voluntary public curfew named as ‘Janta Curfew’, India immediately announced the implementation of a nation-wide complete lockdown for 21 d (i.e. up to 14th April 2020), which only allowed essential services to operate over the entire 130 million population of India[11]. The battle against COVID-19 is still unending in India.
People’s observance of the prevention measures is essential for controlling the spread of COVID-19, which is affected by their knowledge, attitudes, and practices (KAP) towards COVID-19. Therefore, we conducted a survey to investigate the KAP towards COVID-19 among the medical students of a government medical college during the rapid rise period of the COVID-19 outbreak.
2. Materials and methods
2.1. Participants and data collection
This cross-sectional survey was conducted among the medical students from a government medical college, in Uttarakhand, from 22th March to 25th March 2020, the week immediately before the lockdown of India.
As we all know, social-distancing is the best way of prevention from COVID-19, therefore, instead of conducting a community-based survey, this study collected the data using Google form platform as an online survey. The link of Google form was posted and circulated using various social media platforms like Whatsapp Group and e-mail address of the students. The study participants were informed about the details of the study objectives for filling the questionnaire and confidentiality at the beginning of the survey, and informed consent was obtained from each participant. It has been disclosed to all the participants that their identity will keep confidential and the results will be used only for research purposes. Among these 360 responses, 6 were incomplete, therefore, our final samples were 354.
2.2. Questionnaire
A self-designed questionnaire was prepared, which comprised two parts to collect demographic details of the participants along with KAP towards COVID-19. The questions were established on the basis of some published literature[12,13] and the authors’ experience of KAP. After the preparation of the questionnaire, it was sent to some experts to consult their opinions regarding the validity of the questionnaire followed by a small pilot study to test its simplicity and difficulty. However, the results of the pilot study were not included in the actual samples used for the study.
The first part of the questionnaire covered demographic information of the participants and the second part contained questions for KAP assessment. Demographic variables included age, gender, and religion. The self-designed questionnaire comprised 11 questions regarding knowledge, 4 for attitude, and 8 for practice. Knowledge questions mainly dealed with the participants’ knowledge regarding clinical symptoms, transmission routes, prevention, and control of COVID-19. These questions were responded on a true/false basis with an additional “I don’t know” option. The true answer was assigned with 1 point and false/I don’t know answers were assigned with 0 point. Higher scores represented a better knowledge of COVID-19. Similar options were assigned for the questions related to attitude while only two options namely ‘Yes’ and ‘No’ were assigned for the questions related to practice towards COVID-19. Cronbach’s alpha coefficient of the knowledge statements was 0.71[14].
2.3. Statistical analysis
Statistical analyses were performed using SPSS, version 22. Knowledge, attitude, and practice scores were tested for normality of distribution using a one-sample Kolmogorov Smirnov test. Measurement data were expressed as mean±SD and categorical data were expressed as frequency and percentage. Parametric tests (t and ANOVA) were used for comparison between different subgroups of the participants pre-intervention. Comparisons of KAP scores among the students with respect to gender, religion, and age-category are done using independent samples t-test and one-way analysis of variance (ANOVA), as appropriate. The statistical significance level of the test was expressed as α=0.05.
3. Results
3.1. Demographic characteristics
Frequency and percentage of all the demographic characteristics like gender, age, and religion are represented in Table 1. Out of the 354 participants, 50.3% were males while the rest were female (49.7%); the majority of them were 21-23 years old while only 10% were ≥24 years old. Almost 88% of the participants belonged to the religion of ‘Hindu’ while only 3.4% belonged to the other religions.
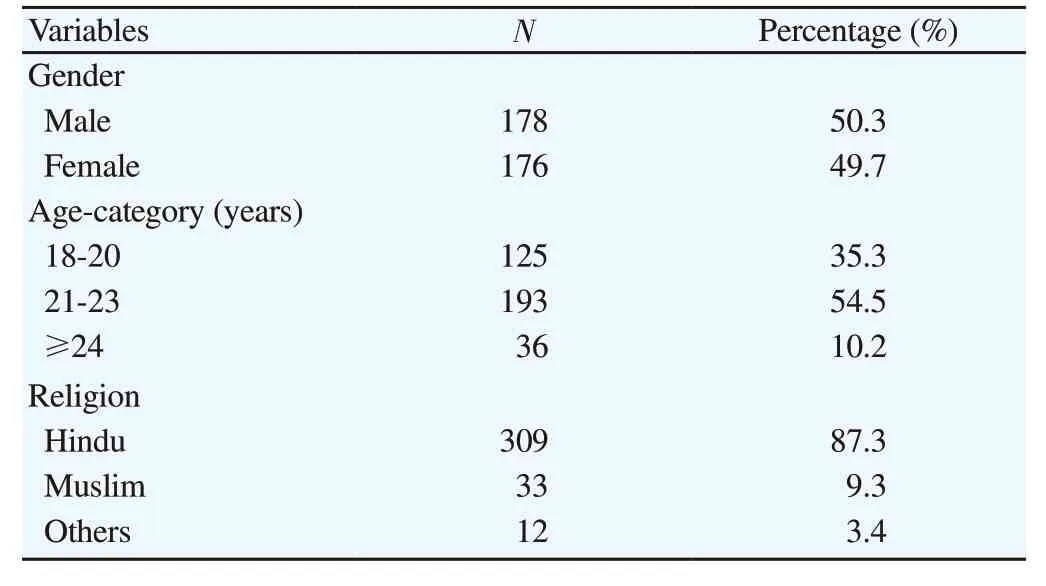
Table 1. Demographic information of the participants.
3.2. Knowledge
The results of the knowledge survey are presented in Table 2. The majority of the participants (86.7%) had correct knowledge about the main symptoms of COVID-19. Furthermost, 92.4% of the participants awared that early symptomatic and supportive treatment can help most patients recover from the infection.
The majority of the students had correct knowledge about the transmission routes of the virus, however, only half of the total participants agreed that ordinary residents can wear general medical masks to prevent the infection by the COVID-19 virus.
Consciousness about the prevention and treatment was high among the participants, such as nearly everyone (96.9%) knew that COVID-19 can be prevented by avoiding crowded places such as train stations and avoiding public transportation. Furthermore, 97.2% of participants realized that people who have contacted with someone infected with the COVID-19 virus should be immediately isolated in a proper place. In general, the observation period is 14 day.
3.3. Attitude
Table 3 shows that the high percentage of the students (76.6%) agreed that media coverage (e.g. newspaper, television, online) give much exposure to news about COVID-19 virus. In addition, the majority of the participants (94.1%) supported the lockdown of the major cities, and more than 75% were in favor of “Janta Curfew” as well.
3.4. Practice
Table 4 presents the health-seeking behavioral intentions and prevention practices of the participants. A high percentage of the participants (98.6%) avoided unnecessary travel or outing during the outbreak. Maintaining social distance during the outbreak was the second most prevalent behavior reported by the participants. Also, a high percentage of participants used hand sanitizer, washed their hands, used a mask, covered a cough and sneeze with a tissue, which represented a good practice of the participants towards COVID-19. However, it is recommended to store helpline number so that they can find help in case of any emergency.

Table 2. Results of the knowledge survey (n=354).

Table 3. Results of the attitude survey (n=354).

Table 4. Results of the practice survey (n=354).
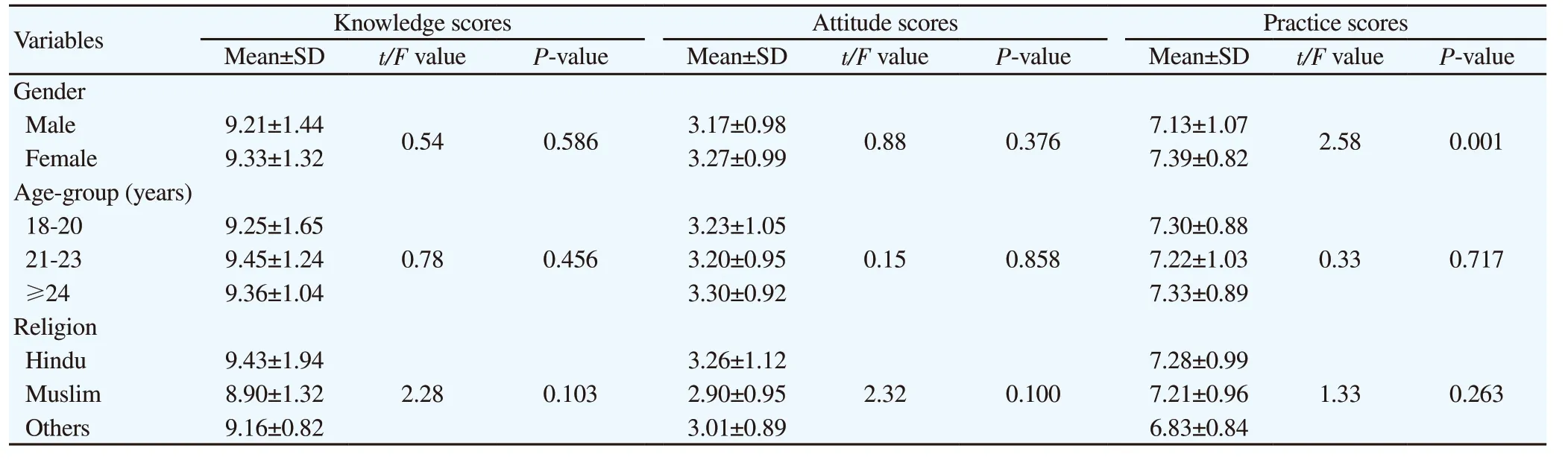
Table 5. Comparison of knowledge, attitude, and practice scores among different demographic variables.
3.5. Analysis of KAP scores with respect to demographic characteristics
Table 5 describes the scores of knowledge, attitude, and practices towards COVID-19 with respect to demographic variables such as gender, age, and religion. The knowledge scores of the female were slightly higher than that of males, although the difference was not significant (P>0.05). Higher scores of females were observed in the attitude and practice as compared with that of males. In addition, the difference in practice score was significant between different genders (P<0.05), therefore, it is recommended that males should pay more attention to practice towards COVID-19.
Secondly, the KAP score for the age-category of 21-23 was higher than the other categories, with no significant difference among groups (P>0.05).
With respect to the religions, participants belonging to the Hindu religion had more knowledge in comparison with the Muslim and others, although the difference was not significant (P>0.05). Also, the same trend was observed in the attitude and practice scores, but again this difference was not significant (P>0.05).
4. Discussion
In the present study, the knowledge, attitude, and practice of the medical students of the Government Doon Medical College towards COVID-19 were assessed. We found that, during the COVID-19 pandemic, 92.7% of the participants had extensive knowledge of COVID-19. In addition, more than 80% of the participants had a positive attitude towards COVID-19.
However, no significant difference was found in mean knowledge or attitude scores with respect to all demographic variables, but gender played a significant role in mean practice scores, and this result is similar to the studies conducted in China, which also reported that practice scores were affected by gender[12,17]. It is worth mentioning that sufficient COVID-19 knowledge scores, positive attitude, and adequate practice were found among the students. Considering that the present study assessed only three demographic variables, so it is recommended that more demographic factors should be included in further studies.
Demographic factors, especially the association between gender and KAP towards COVID-19 are generally consistent with previous studies on COVID-19 and SARS in 2003[12,15,16]. Although the results are very positive towards KAP, we still have some suggestions for both the government and residents of India as well: (1) Few participants stored the helpline number issued by the government, therefore, it is recommended that Indian authorities should raise the awareness about helpline number among the residents; (2) 9% of the participants still not used protective items (like masks, etc.) even the medical students, therefore, the importance of these items should be emphasized more; (3) The results of this study can help to make public-health policies targeting the specific groups with low KAP and increase their KAP through well-planned, appropriate and tailored strategies. Consequently, health promotion activities are vital in improving KAP towards COVID-19, and it is recommended to conduct interventional studies using the results of this study. Positively, In the near future, India will be able to tackle COVID-19 through joint efforts of the Indian governments and all Indian residents.
The major limitation of the present study is that the sample sizes are limited to the students of a government medical college, and hence the results based on the used sample sizes could not be generalized to all the populations of Uttarakhand and India as well, although it can certainly help the state and the country to enhance the awareness regarding KAP in the general population. Due to the questionnaire being self-answered by the participants, there is also a high chance of errors or misrepresentation of information. Less demographic variables is also a limitations. In view of these, more studies should be conducted in the near future to investigate the KAP for COVID-19 at various states and countries.
Conflict of interest statement
The authors report no conflict of interest.
Acknowledgments
The authors thankfully acknowledge the critical suggestions and comments from the learned referees and editorial board which greatly helped us in the improvement of the paper. The first author sincerely acknowledges the colleagues at Department of Community Medicine, Govt. Doon Medical College for their suggestions and comments.
Authors’ contribution
S.M.: Concepts, definition of intellectual content, manuscript preparation, manuscript editing, manuscript review, and guarantor; P.K.G.: Concepts, design, literature search, data acquisition, data analysis, statistical analysis, manuscript review, and guarantor; R.S.: Design, literature, search, data analysis, statistical analysis, manuscript preparation, manuscript editing, manuscript review, guarantor; P.R.: Definition of intellectual content, data acquisition, manuscript preparation, manuscript editing, manuscript review, guarantor.
 Journal of Acute Disease2020年3期
Journal of Acute Disease2020年3期
- Journal of Acute Disease的其它文章
- Factors affecting outcomes of surgically treated patients with cranial extradural hematoma: A cross-sectional study
- Clinical characteristics and treatment of acute epiglottitis: A retrospective study of 28 cases
- Aberration detection of pertussis from the Mazandaran province, Iran, from 2012 to 2018: Application of discrete wavelet transform
- Identification of Panton-Valentine leukocidin virulence gene in methicillinresistant Staphylococcus aureus isolated from clinical specimens of burn patients in Zare Hospitals of Sari, Iran
- Successful treatment of hepatic hydrothorax: A case report
- Suicide attempt of an overt hypothyroid patient with levothyroxine: A case report