
Computer navigation-assisted minimally invasive percutaneous screw placement for pelvic fractures
2020-09-15 08:58
World Journal of Clinical Cases 2020年12期
Tong Yu,Xue-Liang Cheng,Yang Qu,Rong-Peng Dong,Ming-Yang Kang,Jian-Wu Zhao,Department of Orthopedics,the Second Hospital of Jilin University,Changchun 130014,Jilin Province,China
Abstract
Key words:Computer navigation;Percutaneous puncture;Screw;Pelvic fracture;Sacral fracture;Acetabular fracture;Iliac fracture;Pubic fracture
INTRODUCTION
There has been a rapid development of minimally invasive technology in orthopedics in recent years,and the advantages of this technology,including less trauma and rapid recovery,have been recognized by both doctors and patients.However,the procedure’s application is limited due to disadvantages such as the need for repeated fluroscopies,extensive clinician training,and high technical requirements.Computerassisted navigation is a technology that offers a secure method for successfully undertaking minimally invasive techniques.The dislocation rate of screw placement under navigational guidance is 0.1%,which is lower than the traditional screw implantation error rate of 2.6% to 29.5%[1].In addition,the use of navigational guidance can reduce the amount of radiation exposure experienced by surgeons[2].Moreover,patient radiation exposure does not increase either,and may even decrease[3].Although 3-dimensional (3D) scanning of navigation-guided percutaneous punctures may increase scan time,it can reduce unnecessary and repetitive radiation exposure during conventional minimally invasive surgery.
The radiation that a patient receives is affected by the patient’s body mass index,as patients who are overweight may require more energy to be used before a clear image is achieved.Currently,the primary types of computer navigation used in orthopedics are computed tomography (CT)-based navigation,2-dimensional (2D) fluoroscopybased navigation,3D fluoroscopy-based navigation,and electromagnetic navigation(Table1).
The application of navigation techniques in orthopedics is common and used for conditions including spinal deformities,spinal degenerative diseases,bone tumors,joint replacements,etc[4,5].Complex anatomical structures of the pelvis such as narrow corridors,rich muscle-ligament tissue,and neurovascular overlapping intestinal shadows may lead to the insufficient reduction of a fracture or poor screw position.Hence,the therapeutic advantages of navigation for pelvic fractures are evident[6-10].Therefore,this article reviews the indications,contraindications,surgical procedures,and related complications of navigation-guided percutaneous puncture-screw implantation for the treatment of sacral fractures,sacroiliac joint injuries,pelvic ring injuries,and acetabular fractures.We also analyze the causes of inaccurate screw placement.
APPLICATION OF NAVIGATION IN TREATMENT OF PELVIC FRACTURES
Navigation-assisted percutaneous screw placement for treatment of sacroiliac joints and sacral fractures
Sacroiliac joint injury is often accompanied by a pelvic fracture,and these patients often exhibit unstable hemodynamics as well.Sacroiliac joint screws can be used in narrow channels,however,angle deviation may lead to injury of the sacral foramen or penetration of the bone cortex.Anatomical variants of the sacrum and sacroiliac joint,obesity,excessive bowel gas,and osteoporosis may affect the accuracy of screw placement[2,11].Traditional minimally invasive screw placement is prone to damaging blood vessels and nerves,the sacral canal,the gastrointestinal tract,and the urogenital system[2].Although some studies have reported that the sacroiliac joint can be safely repaired without the use of an intraoperative computer-navigation system[12],there are high requirements for both surgeons and surgical positioning accuracy.Therefore,navigation-guided screw placement is conducive to the accurate positioning of the screw and to the safety of the surgery.
Indications and contraindications
Biomechanical technology has shown that navigation-guided percutaneous puncturescrew implantation can provide sufficient stability for pelvic fractures[13].It is indicated for sacroiliac joint dislocations and Dennis type I and type II sacrum fractures with no displacements or slight displacements.Contraindications include sacral fractures with obvious displacement or high instability,and sacral fractures with obvious neurological dysfunctions.When a fracture deformity score is more than 70,navigation cannot improve the accuracy of screw placement[14,15].In general,if a fracture displacement is greater than 10 mm,the cross-sectional contact area is reduced by more than 50%,and the safety of a screw placement is significantly reduced[16].However,when the displacement is more than 10 mm and there is a device that can maintain the reduction,such as a traction bed,a percutaneous screw fixation using navigation for the sacral fracture is feasible[17].
Surgical technique
Patients are anesthetized using general anesthesia and placed in a supine or prone position according to the surgeon’s preference.A reference tracker is fixed to the contralateral iliac wing (with attention given to the position of the tracker to avoid an overabundance of metal artifacts).A 3D scan is then performed,using the fracture site as the center.The acquired images are then matched with the preoperative CT data.The puncture point should be located at the one third position starting from the posterior superior iliac spine to the anterior superior iliac spine of the patient’s posterior pelvic ring.A small skin incision is made under the guidance of navigation.It is important that the incision location is not chosen based on experiences[18,19],as the lateral tension of the patient’s muscle can create pressure on the guide wire cannula,which may lead to incorrect screw placement.After the guide wire sleeve is calibrated,a guide wire (diameter,3.2 mm) is inserted,and the sleeve is then moved while the needle enters it until the guide wire breaks through the sacroiliac joint.At this point a 6.5 mm-8.0 mm diameter screw is inserted through the guide wire.The process can refer to Figure1[19].
The relative spatial position of the reference tracker and pelvis should not be changed during the operation,which is key to ensuring accurate navigation.If the sacroiliac joint is significantly displaced by more than 10 mm,it can be further fixed according to the method of Takao[6]to ensure that there is no change in relative positioning.When the angle between the screw and the vertical line of the bone surface is too large,the risk of positional error during screw insertion increases[20].Therefore,pre-drilling with the navigational drilling tool is recommended if the angle of the screw to be inserted is>35° in the axial position.
Complications
The accuracy of navigation-guided placements is significantly higher than that of conventional percutaneous placements[2].Ghislaet al[21]followed 21 patients with posterior pelvic rings that had been fixed with sacroiliac screws under the guidance of 3D navigation.They found only one case with cortical destruction;there were no other obvious complications in any of the other patients.Improper placement of S1 and S2 screws can be a devastating complication in sacral-fracture surgery or sacroiliac-joint injury[22].If the sacral injury is serious,the S2 nerve is more likely to be injured due to a narrow channel.Moreover,rectal injury may also occur during the surgery.

Figure1 Procedure of sacral screw implantation.A:Navigation planning to design the length,diameter,and the best trajectory of screws;B:The user interface of the screw view mode of navigation,guiding the screw implantation.When the right lower corner of the image shows green (yellow arrow),it would be the best time to implant a guide wire.
Navigation-assisted percutaneous screw placement in the treatment of pubicbranch fractures
Treating the anterior ring of the pelvis was once controversial.It was thought that surgery is necessary only when the pubic symphysis separated more than 25 mm,thus few pubic-branch fractures would need fixation.In recent years however,biomechanical data has confirmed that the anterior ring of the pelvis bears 30% of the tension from the entire pelvis.Therefore,it is necessary to fix the anterior ring and reconstruct the stability of the pelvis.Traditional treatment methods have included open reduction and internal fixation or limited incision and implantation of a titanium plate by minimally invasive plate osteosynthesis technology.However,patient injury can be substantial,and the economic cost of a titanium plate is higher than a screw,so percutaneous puncture technology is now universally preferred.
Indications and contraindications
Treatment of pubic-branch fractures by percutaneous screw fixation under navigation is indicated when there is no displacement,or slight displacement,of a pubic-branch fracture,and the closed reduction of the pubic branch fracture can reach a functional reduction standard[23].Treatment using navigation is contraindicated when there is a fracture at the site of needle insertion,an open pelvic fracture,or a comminuted pubic-branch fracture.
Surgical technique
Fractures of the pubic branch are classified into three types according to Nakatani fracture system[24].The surgical scheme for types I and II is retrograde pubic cannulated screw implantation[25,26],and for type III,it is antegrade implantation of screws.The surgical position of the patient should be supine and general anesthesia is used.After routine disinfection,a reference tracker is fixed on the iliac crest of the healthy side.After activating the tracker on the C-arm,patient,and sleeve,3D scanning is carried out.The position of the guide-wire sleeve is then monitored in real time using the screw-viewing angle mode (Figure2[25]).In general,when the pubic branch is fractured at a low position,the needle entry point should be close to the pubic symphysis.When the pubic branch fracture is in a high position,the needle point should be close to the pubic tubercle.If the fracture is a Nakatani III type,the point of insertion should be the midpoint of the line between the vertex of the greater trochanter and the protrusion of the iliac node.After selecting the appropriate puncture point,a 20 mm skin incision should be made.A guide wire is then inserted after determining the accurate insertion point and direction,and a hollow screw is inserted[12].For men,6.5 mm screws are safe to use;however,these may penetrate the cortex in women[27].
Complications

Figure2 Procedure of transpubic screw implantation.A:Navigation planning;B:The user interface of the screw view mode of navigation.
The accuracy of placement of hollow screws using navigation guidance is significantly higher than that of traditional methods[28,29].If the reduction of a pubic fracture is poor,the possibility of screw perforation will be greater.Injuries of the spermatic cord,uterine ligament,or neurovascular injury are complications associated with pubicbranch fractures[29,30].Therefore,care must be taken when making surgical incisions,subcutaneous tissue should be bluntly separated,and soft-tissue protective sleeves should be added when placing screws.In addition,special care needs to be taken to avoid injury to the corona mortis when treating pubic fractures[31].These can be dangerous vascular injuries that are associated with high mortality[32,33].
Navigation-assisted percutaneous screw placement for acetabular fractures
The treatment of acetabular fractures has always been difficult due to bleeding,the high incidence of postoperative traumatic arthritis[34],heterotopic ossification[35],and other issues.The treatment goal for these fractures is to restore the flatness of the joint surface and stability[36].If the joint surface can be restored through closed reduction,then a traditional operation is unnecessary.Percutaneous screw fixation under navigational guidance can,however,improve the safety of the surgery and reduce trauma and risk of pressure ulcers[37].
Indications and contraindications
The indications of navigation treatment for acetabular fractures are mainly nondisplaced fractures or displaced fractures which can be anatomically reduced by closed reduction[38-42].Contraindications include comminuted fracture,soft tissue incarceration,and other fractures that cannot be anatomically reduced.In general,open reduction and internal fixation is the standard treatment for acetabular fracture displacement.It is difficult to restore the articular surfaceviaclosed reduction if the fracture block is substantially displaced.Articular-surface irregularity is the main factor in the later stage of arthritis,and it has been reported that the risk of arthritis is more than 10%[17],even when satisfactory reduction (displacement < 2 mm[43,44]) has been obtained.Therefore,navigation-guided percutaneous puncture for acetabular fractures should only be applied to non-displaced acetabular fractures or acetabular fractures that can be restored to anatomic reduction following closed reduction[17,45].
Surgical technique
In the treatment of acetabular fractures,the appropriate position (upward,prone,or lateral) is selected according to the surgeon’s preference and general anesthesia is used.A reference tracker is fixed to the anterior,superior iliac spine,or the ischial tuberosity,following routine disinfection,and should then be calibrated and 3D scanned.The data are then matched with the preoperative scanned data.A skin incision is first made using the navigation guide,then a drill-guided pin as long as the screw is inserted.The depth of the screw is then monitored through real-time 3D navigation (Figure3[46]).After inserting all of the guide pins,several 6.5 mm screws should be implanted,and the safety of the screws be confirmed through standard position fluoroscopy.The retrograde anterior column screw technique is used to treat the low anterior column fracture of the acetabulum.In retrograde pubic screw fixation,a guide wire is used to make a channel,and a probe is used to detect whether there is a perforation of the cortical bone.Only then are a guide wire and a screw inserted[47].
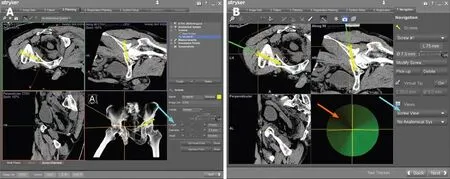
Figure3 Procedure of periacetabular screw implantation.A:Navigation planning;B:The user interface of the screw view mode of navigation.
In the process of screw placement,a safety channel is affected by the thickness of the screw and the angle of insertion.With the increase in screw length,the safety channel becomes narrow.It has been reported that the diameter of the anterior column screw is 6.5 mm,which is safe[29,45,48-50].Morandiet al[47]consider the insertion of screws above 90 mm in the acetabulum to be unsafe because of the need for a larger anterior oblique angle,which can increase the brittleness of the screws.However,short screws can achieve a mechanical strength similar to long screws[45].
Complications
The perforation rate of screw placement under navigational guidance is significantly lower than that under conventional fluoroscopy,and the volume of bleeding is also significantly reduced[42,46,48,51,52].The decrease in bleeding volume may be related to the decrease in puncture times,surgery choice,and surgical time[17].In addition,the incidence of heterotopic ossification also decreases,which may be related to surgical choice[53]and time[54].Under the guidance of 3D navigation,3D fluoroscopy can be used to observe the reduction during surgery,so as to reduce traumatic arthritis caused by the reduction quality.
CAUSES OF INACCURATE PLACEMENT OF SCREWS IN NAVIGATION-GUIDED PERCUTANEOUS SCREW INSERTION
The main role of navigation is to accurately guide the operator in the placement of screws.However,if it is used or operated incorrectly,the accuracy of the navigation becomes questionable.This is primarily due to:(1) The camera and tracker fixed on the patient do not keep stationary and exhibit relative displacement[19,46].This scenario may be caused by the tracker not being firmly fixed,or the fracture being displaced after the reduction;(2) Navigation-guided devices are sleeves,not guide wires or screws;(3) The flexibility of the guide wire causes a deviation during insertion[46];(4)The notch is too small,which causes the guide wire to deviate during insertion,and it cannot be correctly positioned along the expected image-guided track[45,55];and (5)Soft-tissue wrapping.Without the use of a soft-tissue protective sleeve,the guide wire,drill bit,screw,etc.will be twisted by soft tissue during insertion,which affects the accuracy of the navigation.
Although navigation can provide accurate virtual navigation routes and real-time imaging prompts,even when 3D navigation is used,perforation caused by the guide wire or screw cannot be completely avoided due to the possibility of technical problems,the technical expertise of the operator,or the complexity of the anatomy[55].Therefore,the operator must combine both tactile feedback and the visual feedback displayed on a computer screen to determine the accuracy of screw placement.The combination of 3D fluoroscope navigation and CT-based preoperative planning enables the operator to successfully insert a guide wire in a short amount of time[17].
CONCLUSION
Percutaneous screw placement under navigational guidance has the advantages of high accuracy,low incidences of complications and small soft-tissue damage,minimal blood loss,short hospital stays,and quick recovery.Under the premise of mastering navigation skills,there is no difference in the incidence of complications between surgeries performed by new doctors and experienced ones in terms of navigationassisted minimally invasive treatments of pelvic fractures.The use of screws requires that the degree of fracture displacement is not large,and that the screws are able to bear enough shear force.However,computer navigation technology requires extensive training,and attention should be given to avoid complications such as screw misplacement and serious vascular and nerve injuries caused by navigational drift.
 World Journal of Clinical Cases2020年12期
World Journal of Clinical Cases2020年12期
- World Journal of Clinical Cases的其它文章
- Assessment of diaphragmatic function by ultrasonography:Current approach and perspectives
- Research on diagnosis-related group grouping of inpatient medical expenditure in colorectal cancer patients based on a decision tree model
- Evaluation of internal and shell stiffness in the differential diagnosis of breast non-mass lesions by shear wave elastography
- Real-time three-dimensional echocardiography predicts cardiotoxicity induced by postoperative chemotherapy in breast cancer patients
- Lenvatinib for large hepatocellular carcinomas with portal trunk invasion:Two case reports
- Biopsy-proven acute phosphate nephropathy:A case report