
Clinical observation on electroacupuncture plus long-snake moxibustion for rheumatoid arthritis due to kidney deficiency and cold coagulation
2020-12-24 02:35XieYuying谢玉英LiSisi李斯思BenYuehong贲跃宏
关键词:李斯
Xie Yu-ying (谢玉英),Li Si-si (李斯思),Ben Yue-hong (贲跃宏)
Rugao No.3 People’s Hospital,Nantong,Jiangsu Province,Nantong 226500,China
Abstract
Keywords:Acupuncture Therapy;Electroacupuncture;Acupuncture-moxibustion Therapy;Moxibustion Therapy;Indirect Moxibustion; Arthritis, Rheumatoid;Syndrome Differentiation Treatment
Rheumatoid arthritis(RA)is a chronic systemic autoimmune disease featuring synovitis[1]. Synovitis is among the main conditions that incapacitate human in labor ability because it can not only induce joint swelling,pain and morning stiffness,but also cause cartilage damage and bone erosion,thus leading to joint deformity and dysfunction[2].Western medicine mainly adopts the combined treatment of glucocorticoids,non-steroidal anti-inflammatory drugs(NSAIDs),conventional condition-relieving drugs and biological agents.However,adverse reactions such as liver and kidney function damage are common,and the medical costs are not affordable for most patients[3-4].In addition,the treatment compliance is also a big problem,especially in rural areas.In contrast,the traditional Chinese medicine(TCM)treatment of EA plus long-snake moxibustion has turned out to be an effective method with strength in less adverse reactions and low medical costs.In this regard,it is easy to be accepted by patients.In this study,we recruited the cases treated in our hospital in recent years to explore the efficacy of this treatment method,and the details are as follows.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Western medicine
The diagnostic criteria for RA referred the criteria formulated by the American College of Rheumatology (ACR)in 2010[5].The patient had at least one joint clinically defined as synovitis,and it could not be accounted for by other diseases.The diagnosis was based on the score of the affected joints,serum examination results,acute-phase reactants and symptom duration.The total score was 10 points,and the patient could be diagnosed with RA provided the score was≥6 points.In this study,the large joints included shoulder joints,elbow joints, hip joints,knee joints and ankle joints;the small joints included metacarpophalangeal joints,proximal interphalangeal joints,the second to fifth metatarsophalangeal joints,interphalangeal joints of the thumb and wrist joints.Low titer positive meant that the international unit value was higher than the upper limit of normal value,but lower than or equal to 3 times the upper limit of normal value,while high titer positive meant that the international unit value was 3 times higher than the upper limit of normalvalue.Check Table 1 for details.
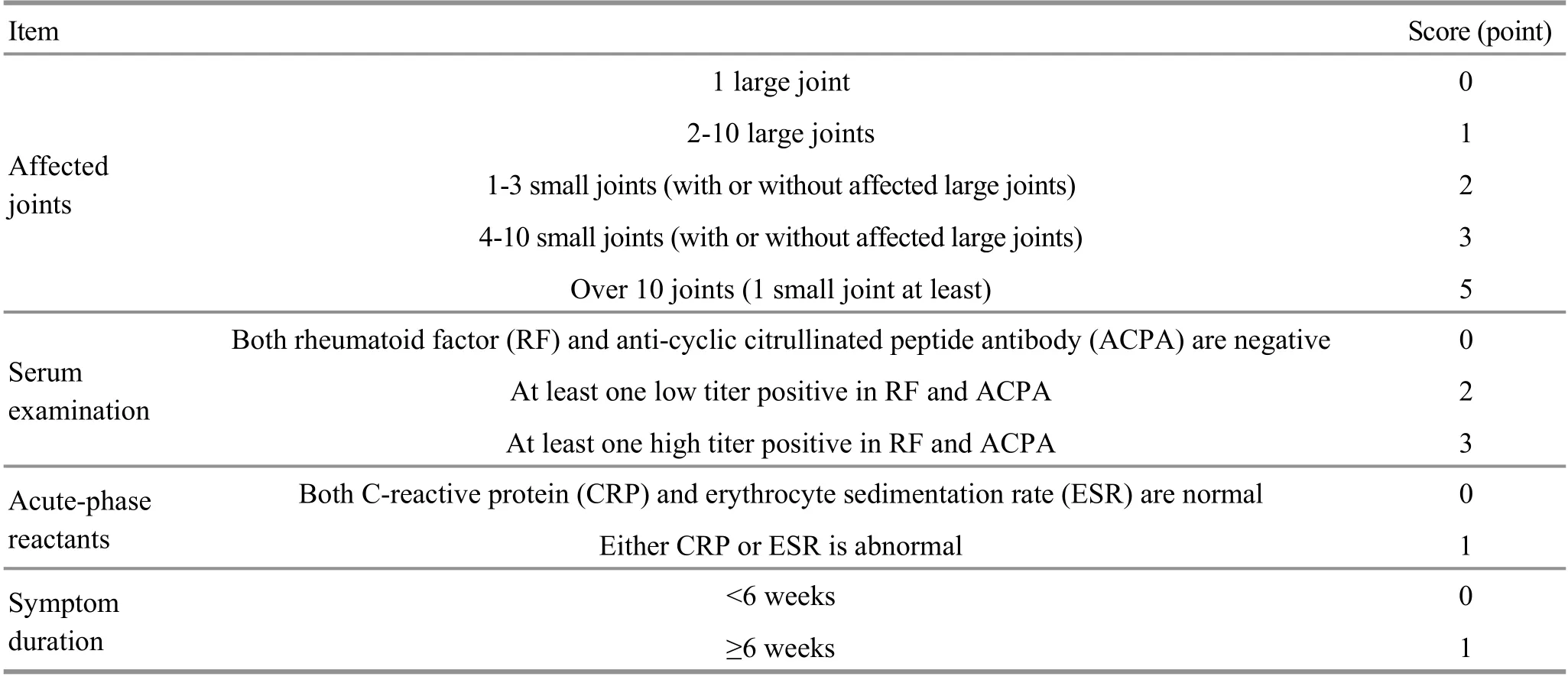
Table 1.RA classification criteria and scoring system in ACR 2010
1.1.2 Traditional Chinese medicine (TCM)
The diagnostic criteria for RA due to kidney deficiency and cold coagulation referred the criteria described in thePractical Rheumatology of Traditional Chinese Medicine[6]. The main symptoms were joint pain and swelling,morning stiffness,inhibited movement and deformity. The secondary symptoms included fear of cold, fatigue and lassitude, soreness in the waist and back, and inhibited bending and stretching, worse in cold weather. The tongue was pale and enlarged with white glossy coating, and the pulse was deep and thin.One could be diagnosed with this disease if he met any 2 of the 4 main symptoms and any 2 of the 5 secondary symptoms,and in addition,his pulse and tongue coating should be completely consistent with the diagnostic criteria.
1.2 Inclusion criteria
Those who met the above diagnostic criteria and whose disease activity score with 28 joint counts(DAS28) was higher than 3.2; aged between 18 and 75 years old;did not receive standard anti-rheumatic treatment before; signed informed consent.
1.3 Exclusion criteria
Women during pregnancy or lactation; those who had serious cardiovascular or cerebrovascular diseases,or other serious diseases involving blood, liver, kidney and digestive tract;could not cooperate with the treatment;those with local skin damage at the to-be-treated acupoints; with joint X-ray examination in stage Ⅳ; used biological agents in the past 3 months or other conventional drugs to relieve symptoms.
1.4 Termination criteria
The study would be terminated in the situations where clinical adverse events,laboratory abnormalities or other medical conditions emerged,and we believed that terminating the study was in the best interests of patients after assessment;drug-induced liver damage occurred,and alanine transaminase or aspartate transaminase was 2 times higher than the upper limit of normal value;the number of leukocyte was lower than 3.0×109/L,and/or that of hemoglobin was lower than 90 g/L,and/or platelet lower than 80×109/L.
1.5 Statistical methods
The SPSS version 17.0 statistical software was adopted for data analysis.Measurement data which(almost)met normal distribution were expressed as mean ± standard deviation(±s).Paired samplet-test was used for intra-group comparisons,and independent samplet-test for inter-group comparisons.Measurement data which did not meet normal distribution were expressed as median(lower quartile,upper quartile)[M(QL,QU)].Chi-square test was adopted for counting data or one-way ordered data.P<0.05 indicated statisticalsignificance.
1.6 Generaldata
The 60 cases recruited in thisstudy were outpatients from the Acupuncture Department of Rugao No.3 People's Hospital,Nantong,Jiangsu Province,between June 2016 and September 2018.They were randomly divided into a control group and an observation group,with 30 cases in each group.There were no significant between-group differences in the general data.Check Table 2 for details.

Table 2.Comparison of the general data between the two groups
2 Therapeutic Methods
2.1 Control group
Patients in the control group took methotrexate tablets and nimesulide dispersible tablets after meals.Methotrexate tablet[2.5 mg/tablet,State Food and Drug Administration(SFDA) Approval No.:H31020644,Shanghai Xinyi Co.,Ltd.,China]was taken orally at 10.0-12.5 mg/time,once a week.Nimesulide dispersible tablet (0.1 mg/tablet, SFDA Approval No.:H20010426,Lepu Pharmaceutical Co.,Ltd.,China)was taken orally at 0.1 mg/time,twice a day.Additional omeprazole enteric-coated capsules (10 mg/capsule,SFDA Approval No.:H20066393,Hainan Pharmaceutical Co.,Ltd.,China)could be taken according to his individual conditions if some patient had gastrointestinal discomfort.This capsule was taken orally before meals at 100 mg/time, twice a day.
2.2 Observation group
Patients in the observation group were given identical oral medications.2.2.1 EA treatment[7]
Major acupoints:Bilateral Quchi(LI 11),Hegu(LI 4),Waiguan(TE 5),Zusanli(ST 36),Yanglingquan(GB 34),Xuanzhong (GB 39),Ganshu(BL 18),Pishu(BL 20),Jinsuo(GV 8)and Shenshu(BL 23).
Adjunct acupoints:Those around joint lesions were selected.Jianliao (TE14),Jianyu (LI15) and Ashipoints were added for shoulder joints;Chize(LU 5)and Quze(PC 3)for elbow joints;Yangchi(TE4),Yanggu(SI5)and Yangxi(LI 5)for wrist joints;Baxie (EX-UE 9)for finger joints;Neixiyan(EX-LE 4),Ququan(LR 8)and Xiyangguan(GB 33)for knee joints; Taixi(KI 3),Jiexi(ST 41),Kunlun(BL 60)and Qiuxu(GB 40) for ankle joints;Bafeng (EX-LE10) for toe joints.
Methods:The patient took a supine position.After routine disinfection, we used filiform needles (Suzhou Medical Supplies Co.,Ltd.,China)of 0.25 mm in diameter and 40 mm in length to needle the acupoints perpendicularly.After needling qi was obtained,we connected the handles of the needles inserted at Hegu(LI4),Quchi (LI11),Yanglingquan(GB 34)and Zusanli(ST 36)to the KWD-808 Yingdi pulse acupuncture therapeutic apparatus(Shanghai Zhangdong Medical Technology Co., Ltd.,China).Continuous wave wasused with frequency of 50 Hz,and this treatment lasted for 20 min.Then we perpendicularly needled the adjunct acupoints and performed reducing manipulations.The needles were retained for 20 min.The patient turned into a prone position after the needleswere withdrawn.We sterilized his skin around the selected back acupoints,then inserted needles obliquely towards the spine,and twirled the needles with the even reinforcing-reducing manipulation.The needles were retained for 20 min,and manipulated once during this period.The treatment wasperformed once every other day.
2.2.2 Long-snake moxibustion treatment
Location:The rectangular area was from Dazhui(GV 14)to Mingmen(GV 4),taking 1.5 cun away from the spine midline as its two sides.
Methods:The patient took a prone position.After sterilization,we first wiped the moxibustion area with fresh ginger sap,then spread fresh ginger mash with a thickness of about 0.5 cm and a width of about 3 cm from top to bottom,and finally spread moxa evenly on the ginger mash with an appropriate thickness(If it was over thick,the heat was difficult to penetrate,and thus impaired the efficacy,or, conversely,it would be too hot to tolerate).Ignited all the flosses and replaced them with new onesfor 2 times after burning out,then removed the ashes and ginger mash to clean the back.The patient shall put on clothes in time to avoid catching a cold.This treatment was performed twice a week and has better performed in sunny weather and daytime.
Both groups were treated for 12 weeks.
3 Observation of Clinical Efficacy
3.1 Observed items
We observed the symptomatic grading and quantifying score,DAS28,ESRaswellas CRPbefore and after treatment.
3.1.1 Symptomatic grading and quantifying score
This score referred theGuiding Principles for Clinical Study of New Chinese Medicines[8].The main symptoms were joint pain and swelling,morning stiffness,limitation of motion and joint tenderness.According to these symptoms,RA patients were divided into four degrees:normal,mild,moderate and severe,with 0,2,4 and 6 points respectively.The secondary symptoms included fear of cold,fatigue and lassitude,soreness in the waist and back,limited bending and stretching,worse in cold weather.And according to the secondary symptoms,they were divided into the identical four degrees,with 0,1,2 and 3 points respectively.On the basis of this scoring standard,we observed and recorded the scoresbefore and after treatment.
3.1.2 DAS28
We calculated the DAS28 based on the number of swelling and tenderness in the 28 joints,ESR and the patient's health condition or the patient's overall evaluation of the disease.The score>5.1 points suggested high disease activity index (DAI); >3.2 points and≤5.1 points suggested moderate DAI;>2.6 points and≤3.2 points suggested low DAI;≤2.6 points suggested remission.We observed whether the patients were in low DAI(DAS28 between 2.6 and 3.2 points)or disease remission(DAS28≤2.6 points),and compared the number of patients in both stages between the two groups.
3.1.3 Inflammation indicators
We observed ESRand CRPpre-and post-treatment.
3.2 Efficacy evaluation criteria
The criteria referred theGuiding Principles for Clinical Study of New Chinese Medicines[8]and improvement rate of the symptomatic grading and quantifying score.
Improvement rate=(Pre-treatment score-Posttreatment score) ÷ Pre-treatment score×100%.
Markedly effective:The improvement rate was ≥75%,and all laboratory indicators were normal or close to normal.
Improvement:The improvement rate was ≥50%,but <75%,and all laboratory indicators were obviously improved.
Effective:The improvement rate was≥30%,but <50%,and the laboratory indicators were slightly improved or not improved.
Invalid:The improvement rate was less than 30%,and there was no improvement in laboratory indicators.
3.3 Results
All the patients completed the treatment with no dropout or termination.
3.3.1 Comparison of the symptomatic grading and quantifying score
Before treatment, there was no significant betweengroup difference in this score(P>0.05).After treatment,the scores in both groups were significantly improved(bothP<0.05),with the improvement in the observation group more obvious than that in the control group(P<0.05).Check Table 3 for details.
Table 3.Comparisons of the symptomatic grading and quantifying score( ±s, point)

Table 3.Comparisons of the symptomatic grading and quantifying score( ±s, point)
Group n Pre-treatment Post-treatment t-value P-value Observation 30 7.90±1.71 3.30±2.80 4.029 0.005 Control 30 7.82±2.11 4.83±1.82 4.221 0.001 t-value 1.363 3.169 P-value 0.200 0.010
3.3.2 Comparison of the DAS28
Before treatment, there was no significant betweengroup difference in the DAS28 score(P>0.05).After treatment, the scores in both groups were significantly improved (bothP<0.05), with the improvement in the observation group more significant than that in the control group (P<0.05). Besides, there were 11 cases in low DAI and remission in the observation group versus 5 cases in the control group,showing a statistically significant between-group difference (P<0.05).Check Table 4 and Table 5 for details.
3.3.3 Comparison of the inflammation indicators
Before treatment, there were no significant betweengroup differences in the ESR and CRP levels(bothP>0.05). After treatment,the two levels in both groups were significantly reduced(allP<0.05),also showing statistically significant between-group differences (bothP<0.05).Check Table 6 and Table 7 for details.
Table 4.Comparison of the DAS28 score between the two groups( ±s, point)
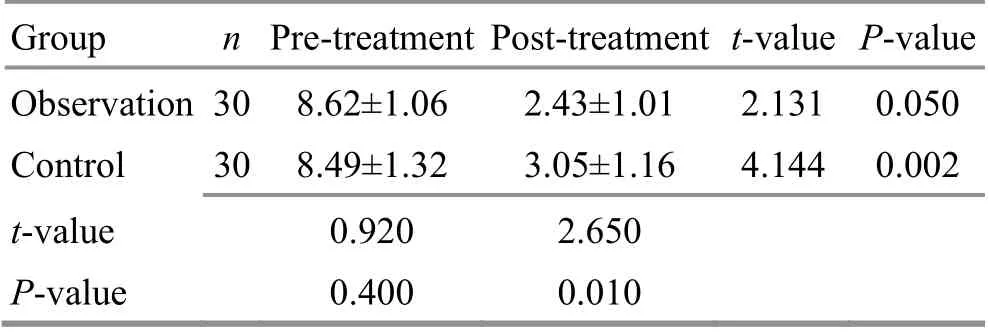
Table 4.Comparison of the DAS28 score between the two groups( ±s, point)
Group n Pre-treatment Post-treatment t-value P-value Observation 30 8.62±1.06 2.43±1.01 2.131 0.050 Control 30 8.49±1.32 3.05±1.16 4.144 0.002 t-value 0.920 2.650 P-value 0.400 0.010
Table 6.Comparisons of the ESR level between the two groups( ±s,mm/h)
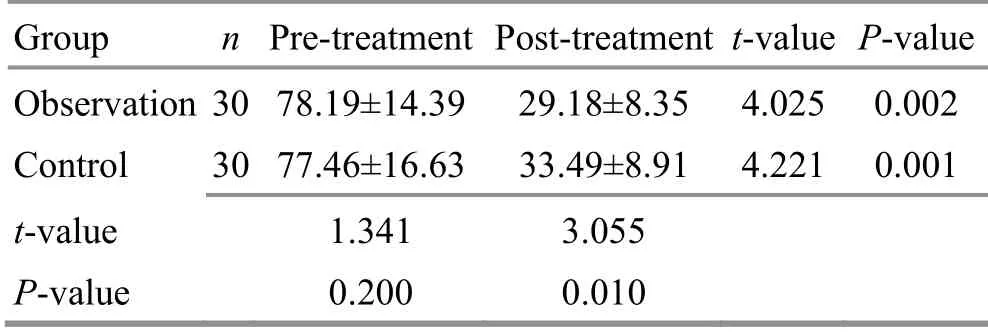
Table 6.Comparisons of the ESR level between the two groups( ±s,mm/h)
Group n Pre-treatment Post-treatment t-value P-value Observation 30 78.19±14.39 29.18±8.35 4.025 0.002 Control 30 77.46±16.63 33.49±8.91 4.221 0.001 t-value 1.341 3.055 P-value 0.200 0.010

Table 5.Comparison of the DAI between the two groups(case)
Table 7.Comparisons of the CRP levels between the two groups( ±s,mg/L)

Table 7.Comparisons of the CRP levels between the two groups( ±s,mg/L)
Group n Pre-treatment Post-treatment t-value P-value Observation 30 45.07±11.06 14.71±4.59 3.747 0.020 Control 30 41.23±9.95 20.92±7.83 4.029 0.025 t-value 0.868 2.583 P-value 0.400 0.020
3.3.4 Comparison of the clinical efficacy
The total effective rate was 89.9% in the observation group versus 76.6%in the control group, showing a significant difference (P<0.05). Check Table 8 for details.

Table 8.Comparison of the clinical efficacy between the two groups (case)
3.3.5 Safety observation
During the study,4 patients presented mild liver dysfunction,including 1 case in the observation group and 3 cases in the control group.Their conditions improved after taking silymarin tabletsand thus did not quit the study.Besides,3 patients showed leukopenia with the leukocyte count between 3.4×109/L and 4.0×109/L,including 1 case in the observation group and 2 cases in the control group.After taking Leucogen tablets, their leukocyte count returned to normal and they continued treatment.No other adverse reactions were found in the two groups.
4 Discussion
RA falls under the category of Bi-Impediment syndrome in TCM.It ismainly attributed to deficiency of both healthy qiand kidney.Professor Jiao Shu-de holds that RA is caused by constitutional kidney deficiency and cold pathogen invading bones,which illustrates why the pattern of kidney deficiency and excessive cold is more common in clinical practice[9].Professor Wu SY[10]thinks that various etiologies and complicated pathogenesis can induce RA,among which kidney deficiency and cold coagulation isthe crucial one.In the opinions of Professor Kuang Hui-tao,this disease is a result of phlegm blood stasis caused by healthy qi deficiency and pathogen invasion[11].Therefore,this study took patients with RA due to kidney deficiency and cold coagulation as the research subjects.
RA is a refractory autoimmune disease and a challenge for modern medicine. Clinical treatment will take such measures to protect joint function asrelieving joint inflammation, slowing disease development and inhibiting bone destruction function,and consequently achieve complete remission or low DAI.As for the oral medications,methotrexate has a positive effect in controlling patients’conditions.As an anchor drug for this disease,it is often used in combination with other anti-rheumatic drugs. However,it may increase the risk of infection and tumor,and the patients often show poor compliance.
Professor Wu ZC[12]notes that the method of warming meridian is the fundamental treatment principle for Bi-Impediment syndrome,and acupuncture and moxibustion have therapeutic advantages for RA.Based on Western medicine treatment,we employed EA plus long-snake moxibustion to treat this disease,which can elevate yang qi,tonify the kidney and dispel cold,warm yang and unblock collaterals.This therapy can effectively relieve the pain and reduce DAI,thus improving the patients’quality of life.By needling relevant points,local qiand blood can be dredged,which facilitates the harmony of Ying-Nutrient and Wei-Defensive aspects,and therefore the manifestation can be treated.Long-snake moxibustion demonstrates such strengths as relatively large moxibustion area and moxa cone,long treatment time,and strong warming and dredging power[13].The Governor Vessel runs along the posterior midline of the human body, and plays a leading role among yang meridiansbecause it intersectswith the six yang meridians and Yang Link Vessel.In this regard,it can regulate qi and blood of yang meridians,and dominatesboth the activity and function of yang qi.The function of moxibustion on the Governor Vessel lies in warming kidney and strengthening bones,as well as supplementing essence and nourishing marrow[14].The prominent TCM master Zhu Liang-chun once observed that treatment of Bi-Impediment syndrome shall emphasize ‘tonifying kidney and strengthening the Governor Vessel’to address the root cause[15]. EA plus long-snake moxibustion can treat both manifestation and root cause of this disease,through which Bi-Impediment syndrome will be improved or even corrected.
In recent years,studies have shown that the pathogenesis of RA is closely related to the dysfunction of hypothalamic-pituitary-adrenal axis(HPAA),and acupuncture can regulate the secretion of relevant hormonesof HPAA[16].Modern studies have proved that acupuncture can achieve analgesic and antiinflammatory effects by increasing the antiinflammatory cytokine contents,reducing the proinflammatory cytokine contents and thus adjusting the balance of T helper cells(Th)1/Th2[17].Wu HG,et al[18]have found that moxibustion can regulate the synthesis of inflammatory cytokines by increasing the level of adrenocorticoid through HPAA.Various moxibustion therapies for experimental RA have all shown obvious anti-inflammatory effects[19].Ai Ye(Folium Artemisiae Argyi)polysaccharide can regulate the immune function of mice and has consequent enhancing effects on humoral immunity,cellular immunity and non-specific immunity[20].Ren JG,et al[21]have found that moxibustion can not only reduce the hyperplasia of joint fibrous tissues and synovial tissues,but also the synovial tissue mPD-1 expression and inflammatory cell infiltration.Chang XR,et al[22]confirmed that the mechanism of moxibustion’s warming and tonifying effect is that it activates acupoints,promotes qi and blood circulation,and thus regulates nerve-endocrineimmune network and functionsof Zang-fu organs.
The results of this study showed that EA plus longsnake moxibustion can significantly improve the symptoms in RA patients and enhance the clinical efficacy. Therefore,it isworthy of further study.
Conflict of Interest
The authorsdeclarethat thereisno conflict of interest.
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received:8 October 2019/Accepted:24 February 2020
猜你喜欢
小小说月刊(2019年3期)2019-03-25
爱你(2018年25期)2018-09-12
爱你·心灵读本(2018年9期)2018-09-10
新作文·初中版(2016年4期)2016-05-05
儿童故事画报(2016年2期)2016-04-18
共产党员(辽宁)(2015年18期)2015-12-06
微型小说选刊(2014年18期)2014-11-15
意林·少年版(2014年18期)2014-10-21
花样盛年(2014年3期)2014-03-19
辽河(2009年9期)2009-11-09
 Journal of Acupuncture and Tuina Science2020年6期
Journal of Acupuncture and Tuina Science2020年6期
- Journal of Acupuncture and Tuina Science的其它文章
- The role of microglia in thalamic reticular nucleus in acupuncture regulating cognitive deficits in insomnia rats
- Study on the acupoints belonging to the three yin meridians of foot reflecting the variation pattern of uterine qi and blood in women with moderate constitution
- Effects of electroacupuncture on uterine prostaglandin F2α, cyclooxygenase 2 and nuclear factor κB in rats with primary dysmenorrhea
- Effect of moxibustion at sensitized-acupoints on quality of life in patients with chronic superficial gastritis
- Research advances in the brain mechanisms of acupuncture effects based on the BOLD-fMRI technology
- Effects of intradermal needle therapy plus pinaverium bromide on gastrointestinal hormone levels in irritable bowel syndrome-diarrhea patients