经肝动脉化疗栓塞术联合局部热消融治疗大肝癌的效果及影响因素
2021-11-30 15:30祖亮杨栋云高杨应希慧赵中伟
中国现代医生 2021年18期
祖亮 杨栋云 高杨 应希慧 赵中伟


[關键词] 大肝癌;经肝动脉化疗栓塞术;局部热消融;疗效;危险因素
[中图分类号] R735.3 [文献标识码] B [文章编号] 1673-9701(2021)18-0100-04
Effect and influencing factors of transcatheter arterial chemoembolization combined with local thermal ablation in treatment of large hepatocellular carcinoma
ZU Liang1 YANG Dongyun2 GAO Yang1 YING Xihui1 ZHAO Zhongwei1
1.Department of Radiology,Lishui Municipal Central Hospital in Zhejiang Province, Lishui 323000, China; 2.Department of Ultrasonography, Lishui Municipal Central Hospital in Zhejiang Province, Lishui 323000, China
[Abstract] Objective To explore the efficacy of transcatheter arterial chemoembolization (TACE) combined with local thermal ablation in the treatment of large hepatocellular carcinoma (HCC), and to analyze the risk factors affecting the efficacy. Methods Ninety patients with large hepatocellular carcinoma treated in our hospital form January 2017 to December 2019 were selected as research subjects, and retrospective analysis was performed. Transcatheter arterial chemoembolization combined with local thermal ablation was given to all patients. The short-term efficacy was evaluated and the objective response rate was calculated. The patients were divided into the objective response group and the control group (not achieving the objective response) according to the short-term efficacy. The clinical data of the two groups were compared, and the risk factors affecting the efficacy of transhepatic arterial chemoembolization combined with local thermal ablation in patients with large hepatocellular carcinoma were analyzed by univariate analysis and multivariate Logistic regression analysis. Results After transhepatic arterial chemoembolization combined with local thermal ablation, among the 90 patients with large hepatocellular carcinoma, 47 patients achieved objective response, and 43 patients didn′t achieve objective response, with the objective response rate of 52.22%. In the univariate analysis, there were statistically significant differences in the tumor diameter, tumor number, tumor clinical stage, preoperative alpha-fetoprotein level, and portal vein tumor thrombus between the objective response group and the control group(P<0.05). There was no statistically significant difference in age, gender and body mass index between the objective response group and the control group(P>0.05). According to the multivariate Logistic regression analysis, tumor diameter ≥7 cm, tumor number ≥2, tumor clinical stage Ⅲ-IV, preoperative alpha-fetoprotein level ≥200 μg/L, and portal vein tumor thrombus were risk factors affecting the efficacy of transcatheter arterial chemoembolization combined with local thermal ablation in patients with large hepatocellular carcinoma. Conclusion Transcatheter arterial chemoembolization combined with local thermal ablation has a certain efficacy in patients with large hepatocellular carcinoma,but the efficacy is affected by tumor diameter, tumor number, tumor clinical stage,preoperative alpha fetoprotein level, portal vein tumor thrombus and other factors,so it is necessary to implement corresponding intervention according to the above risk factors.
[Key words] Large hepatocellular carcinoma; Transcatheter arterial chemoembolization; Local thermal ablation; Efficacy; Risk factors
肝癌作为一种常见的恶性肿瘤,发病率极高,其发病率在我国恶性肿瘤中居于第4位,且具有较高的死亡风险,患者的生命健康受到严重威胁[1-3]。经肝动脉化疗栓塞术、局部热消融是临床治疗肝癌的主要方法,均属于介入治疗[4],但由于大肝癌作为肿瘤直径达到5 cm的肝癌,其治疗难度大[5],采用肝动脉化疗栓塞术、局部热消融治疗后部分患者的近期疗效欠佳,还需对其疗效影响因素进行明确,以进一步提高大肝癌患者的近期疗效。本研究针对90例经肝动脉化疗栓塞术联合局部热消融治疗的大肝癌患者进行回顾性研究,以探讨经肝动脉化疗栓塞术联合局部热消融治疗大肝癌的疗效,明确影响其疗效的危险因素,现报道如下。
1 资料与方法
1.1 一般资料
选择2017年1月至2019年12月我院收诊的90例大肝癌患者作为研究对象,患者年龄30~79岁,年龄≥60岁者39例,年龄<60岁者51例;男49例,女41例;身体质量指数(BMI)≥25 kg/m2 23例,<25 kg/m2 67例;23例患者伴门静脉癌栓。
纳入标准[6]:①经影像学检查、临床症状观察、手术病理诊断,肿瘤直径≥5 cm,确诊为大肝癌者;②具备经肝动脉化疗栓塞术、局部热消融指征者;③术前对手术方案知情同意,签署知情同意协议;④临床资料保存完整,无缺失者。
排除標准[7]:①合并全身严重感染者;②合并其他恶性肿瘤者;③既往有肝切除术、肝移植术、肝动脉化疗栓塞术、消融治疗等治疗史者;④存在精神障碍者;⑤临床资料欠缺完整性者。
1.2 方法
所有患者均接受经肝动脉化疗栓塞术联合局部热消融治疗,患者采取仰卧位,经右侧股动脉穿刺置管,将导管置入肝脏肿瘤供血靶动脉,注入造影剂,明确肝脏肿瘤位置,再经导管将明胶海绵颗粒栓塞剂、碘化油乳剂注入至肝动脉,对肝动脉进行栓塞;经肝动脉化疗栓塞术后1周实施局部热消融治疗,患者采取仰卧位,局部浸润麻醉,在超声或CT引导下穿刺,置入消融针至肝癌病灶中央区,设定好消融电压和时间,再开始局部消融。
1.3 观察指标及评价标准
治疗后,评价近期疗效,统计客观缓解率,客观缓解率=(完全缓解例数+部分缓解例数)/总例数×100%,具体评价标准为:完全缓解(CR):肝脏肿瘤病灶消失,无新病灶出现;部分缓解(PR):肝脏肿瘤病灶面积减小幅度≥30%,无新病灶出现;稳定(SD):肝脏肿瘤病灶面积减小幅度<30%或增大幅度<20%;进展(PD):肝脏肿瘤病灶面积增大幅度≥20%,出现新病灶[8]。
根据患者近期疗效将其分为客观缓解组、对照组(SD+PD),比较两组的临床资料,对影响大肝癌患者经肝动脉化疗栓塞术联合局部热消融疗效的危险因素进行单因素分析、多因素Logistic回归分析,分析指标包括年龄(≥60岁或<60岁)、性别(男或女)、BMI(≥25 kg/m2或<25 kg/m2)、肿瘤直径(≥7 cm或<7 cm)、肿瘤数目(≥2个或<2个)、肿瘤临床分期(Ⅰ~Ⅱ期或Ⅲ~Ⅳ期)、术前甲胎蛋白水平(≥200 μg/L或<200 μg/L)、门静脉癌栓(有或无)。
1.4 统计学方法
应用SPSS 26.0统计学软件处理数据,计量资料用(x±s)表示,采用t检验,计数资料用[n(%)]表示,采用χ2检验,P<0.05为差异有统计学意义;将单因素分析中数据资料整理成计数资料形式,实施χ2检验,P<0.05时为差异有统计学意义,将单因素分析中统计学结果为P<0.05的变量纳入多因素Logistic回归模型中,赋值,分析,以α=0.05为检验水准。
2 结果
2.1 大肝癌患者经肝动脉化疗栓塞术联合局部热消融治疗的疗效
经肝动脉化疗栓塞术联合局部热消融治疗后,90例大肝癌患者中有47例患者客观缓解(19例完全缓解、28例部分缓解),其余43例未达到客观缓解(30例稳定、13例进展),客观缓解率为52.22%。
2.2 大肝癌患者经肝动脉化疗栓塞术联合局部热消融治疗疗效的危险因素分析
2.2.1 单因素分析 在单因素分析中,客观缓解组与对照组的肿瘤直径、肿瘤数目、肿瘤临床分期、术前甲胎蛋白水平、门静脉癌栓比较,差异均有统计学意义(P<0.05),而两组的年龄、性别、体质量指数比较,差异均无统计学意义(P>0.05)。见表1。
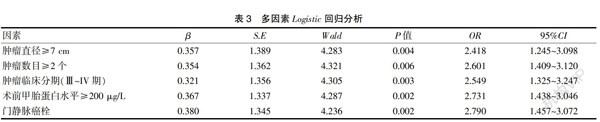
2.2.2 多因素Logistic回顾分析 将单因素分析中P<0.05的变量录入至多因素Logistic回归模型中进行赋值,赋值结果见表2;经多因素Logistic回归分析发现,肿瘤直径≥7 cm、肿瘤数目≥2个、肿瘤临床分期Ⅲ~IV期、术前甲胎蛋白≥200 μg/L、伴有门静脉癌栓是影响大肝癌患者经肝动脉化疗栓塞术联合局部热消融治疗效果的危险因素。见表3。
3 讨论
原发性肝癌是我国最为常见的恶性肿瘤之一,具有高发病率和高死亡率,患者发病后存在肝区疼痛等症状[9]。原发性肝癌患者早期阶段的肿瘤恶性程度低,随着病情进展,其肿瘤体积逐渐增大,逐渐侵袭周围组织,严重危害患者的生命安全[10]。大肝癌是指肿瘤直径≥5 cm的肝癌类型,其肿瘤体积较大,预后较差[11-12],需实施积极治疗。
近年来,肝动脉化疗栓塞术、局部热消融在原发性肝癌治疗中取得一定的效果。肝动脉化疗栓塞术属于介入治疗,主要是通过穿刺置管,经导管将明胶海绵颗粒、碘化油注入至肝动脉,对肝动脉进行栓塞,可阻断肝动脉对肝脏肿瘤的血供,促使肝脏肿瘤逐渐萎缩,发挥缩小肿瘤体积、延缓肿瘤进展的作用[13-15]。局部热消融也属于介入治疗手段,主要是利用微波或射频电流对肝脏肿瘤进行振荡,利用振荡作用摩擦生热,而肿瘤组织对热的耐受性不及正常组织,当温度达到一定程度时,肿瘤组织可逐渐消融,癌细胞内部线粒体和溶酶体遭到破坏,癌细胞逐渐凋亡,从而发挥抗癌作用[16-18]。本研究中,经肝动脉化疗栓塞术联合局部热消融治疗后,90例大肝癌患者中有47例患者客观缓解,客观缓解率为52.22%,说明肝动脉化疗栓塞术+局部热消融可在大肝癌患者中发挥良好抗癌作用,延缓肿瘤进展,但部分患者近期疗效不够理想,有待提高。
明确影响疗效的危险因素是提高疗效的关键,本研究针对经肝动脉化疗栓塞术联合局部热消融治疗后不同疗效的大肝癌患者进行回顾性研究,经单因素分析、多因素Logistic回归分析后发现,肿瘤直径≥7 cm、肿瘤数目≥2个、肿瘤临床分期Ⅲ~IV期、术前甲胎蛋白≥200 μg/L、伴有门静脉癌栓是影响大肝癌患者经肝动脉化疗栓塞術联合局部热消融治疗效果的危险因素,作用机制如下:①肿瘤直径、肿瘤数目、肿瘤临床分期、甲胎蛋白水平均反映了肝癌患者肿瘤进展情况,而肿瘤直径≥7 cm、肿瘤数目≥2个、肿瘤临床分期Ⅲ~IV期、术前甲胎蛋白≥200 μg/L的大肝癌患者其病情更加严重,采用肝动脉化疗栓塞术+局部热消融治疗易存在肿瘤残留、不完全消融等情况,影响其疗效;②门静脉癌栓是原发性肝癌患者的常见并发症,原发性肝癌患者并发门静脉癌栓后其病情加重,其肿瘤进展加快,生存期限缩短,这类患者经介入治疗后的预后相对较差[19-22]。
综上所述,经肝动脉化疗栓塞术联合局部热消融在大肝癌中具有一定的治疗效果,但患者疗效受到肿瘤直径、肿瘤数目、肿瘤临床分期、术前甲胎蛋白水平、门静脉癌栓等因素的影响,临床上需根据上述危险因素实施相应干预。
[参考文献]
[1] Joskin Julien,de Baere,Thierry Auperin,et al.Predisposing factors of liver necrosis after transcatheter arterial chemoembolization in liver metastases from neuroendocrine tumor[J].Cardiovascular and Interventional Radiology,2015,38(2):372-380.
[2] 刘凌晓,王建华,王小林,等.经皮热消融同步肝动脉化疗栓塞(TACE)治疗肝癌的临床价值[J].复旦学报(医学版),2015,42(1):1-6.
[3] Chao Yee,Chung Younghwa,Han Guohong,et al.The combination of transcatheter arterial chemoembolization and sorafenib is well tolerated and effective in Asian patients with hepatocellular carcinoma:Final results of the START trial[J].International Journal of Cancer,2015, 136(6):1458-1467.
[4] Hiraoka Atsushi,Ishimaru Yoshihiro,Kawasaki Hideki,et al.Tumor markers AFP, AFP-L3,and DCP in hepatocellular carcinoma refractory to transcatheter arterial chemoembolization[J].Oncology,2015,89(3):167-174.
[5] 袁宏军,刘凤永,李鑫,等.肝动脉化疗栓塞联合局部消融治疗大肝癌的现状和趋势[J].中华肝胆外科杂志,2017, 23(10):712-716.
[6] 王斌,付守忠,戴锋,等.TACE联合热消融治疗中小肝癌24例[J].实用临床医药杂志,2015,19(21):94-95.
[7] Lee SS,Kim KA,Park MS,et al. MRI findings and prediction of time to progression of patients with hepatocellular carcinoma treated with drug-eluting bead transcatheter arterial chemoembolization[J].Journal of Korean medical science,2015,30(7):965-973.
[8] Takeda Akihiro,Koike Wataru,Hayashi Shotaro,et al.Magnetic resonance imaging and 3-dimensional computed tomographic angiography for conservative management of proximal interstitial pregnancy by hysteroscopic resection after transcatheter arterial chemoembolization[J].Journal of Minimally Invasive Gynecology,2015,22(4):658-662.
[9] 霍祥辉.经导管肝动脉化疗栓塞联合微波消融治疗大肝癌的临床研究[D].青岛:青岛大学,2017.
[10] Farinati Fabio,Vanin Veronica,Giacomin Anna,et al.BCLC stage B hepatocellular carcinoma and transcatheter arterial chemoembolization:A 20-year survey by the italian liver cancer group[J].Liver international,2015, 35(1):223-231.
[11] Murotani Kazuhiro,Nakai Motoki,Sato Morio,et al.Change in portal vein hemodynamics after chemoembolization for hepatocellular carcinoma: Evaluation through multileveld dynamic multidetector computed tomography during arterial portography[J].Journal of Computer Assisted Tomography,2015,39(3):396-400.
[12] 王忠,李伟,刘丹丹,等.肝动脉栓塞化疗术联合射频消融治疗初发性及复发性肝癌的疗效及影响因素分析[J].实用老年医学,2018,32(9):821-824.
[13] Hirooka M,Hiraoka A,Ochi H,et al. Transcatheter arterial chemoembolization with or without radiofrequency ablation: Outcomes in patients with barcelona clinic liver cancer stage B hepatocellular carcinoma[J].The American Surgeon,2018,210(4):1-8.
[14] Tang Bixia,Sheng Xinan,Chi Zhihong,et al. Efficacy and safety of transcatheter arterial chemoembolization combined with systemic chemotherapy in urothelial carcinoma patients with liver metastasis[J]. Tumor,2018,38(2):120-125.
[15] Erica SA,Rosemarie Mick,Gregory J,et al. Combined chemoembolization and thermal ablation for the treatment of metastases to the liver[J]. Abdominal Radiology, 2018, 22(4):1-9.
[16] Takeshi Hatanaka,Hirotaka Arai,Satoru Kakizaki.Balloon-occluded transcatheter arterial chemoembolization for hepatocellular carcinoma[J]. World Journal of Hepatology,2018,10(7):485-495.
[17] Houbin Sun,Minghui Zhang,Ruibao Liu,et al. Endovascular implantation of 125 I seed combined with transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma[J]. Future Oncology,2018,14(12):12-15.
[18] Jianying Zeng,Xianghao Piao,Zhongyuan Zou,et al. Cryoablation with drug-loaded bead embolization in the treatment of unresectable hepatocellular carcinoma: Safety and efficacy analysis[J].Oncotarget,2018,9(7):7557-7566.
[19] 许贇,王能,沈强,等.经皮热消融治疗极早期肝癌的疗效及预后因素分析[J].中国普通外科杂志,2015,24(7):945-951.
[20] 宗迎迎,徐浩,许伟,等.经肝动脉化疗栓塞联合经皮微波消融序贯治疗早期肝癌的疗效及预后影响因素[J].介入放射學杂志,2015,24(3):210-214.
[21] 邢爱丽,郑加生.经肝动脉化疗栓塞术联合局部热消融治疗大肝癌的效果及影响因素[J].临床肝胆病杂志,2019,35(1):98-103.
[22] 帕哈尔丁·白克热,阿不拉江·阿不都克力木,王海林,等. 超声引导下射频消融术治疗原发性肝癌的疗效及对患者免疫功能与预后的影响[J].疑难病杂志,2019, 18(6):577-581.
(收稿日期:2020-08-13)
猜你喜欢
中华养生保健(2020年1期)2020-11-16
中国中医急症(2019年10期)2019-05-21
中国医药指南(2017年3期)2017-11-13
科技资讯(2016年19期)2016-11-15
中国实用医药(2016年24期)2016-10-17
中国康复理论与实践(2015年10期)2015-12-24
中国医学科学院学报(2014年6期)2014-03-11
军事体育学报(2014年3期)2014-02-27