
Factors associated with active aging in Chinese elderly in rural areas of Xiangtan County, China†
2021-12-29 11:16XueLinFuJinGungLiYinLiSuHongHongWngYngGuoLiQiongLiuChunYnZeng
Frontiers of Nursing 2021年4期
Xue-Lin Fu, Jin-Gung Li, Yin-Li Su, Hong-Hong Wng, Yng Guo, Li-Qiong Liu,Chun-Yn Zeng
aXiangtan Medicine and Health Vocational College, Xiangtan, Hunan 411104, China bSchool of Nursing, Central South University, Changsha, Hunan 410013, China
Abstract: Objectives: To explore the level of active aging and correlates among rural elderly in Xiangtan County, China.
Keywords: elderly • active aging • rural area
1. Introduction
Aging has become a global trend. By 2050, 22% of the world’s population will be over 60 years old, which is an increase from 11% in 2019. With the rapid increase of the aging population, a series of social problems brought about by the older population, such as health concerns and support and nursing for the aged, is already causing a wide social concern. Positive and effective measures to cope with these problems must be taken and prioritized worldwide.
If everyone can achieve a relatively close life expectancy and healthy lifespan and can spend their old age independently, then the problem of aging can be effectively solved. Under the guidance of this concept,the World Health Organization (WHO) introduced the concept of active aging, which is sometimes translated as “positive aging”. Active aging has been defined as “...the process of optimizing opportunities for health, participation, and security, in order to enhance quality of life and well being as people age”.1It is an umbrella concept embracing a semantic space in which healthy, successful, and productive aging are strongly related.2Unlike other theories of aging, active aging puts the elderly in an active position in the process of aging rather than in a passive one. It also includes old men suffering from any disability or disease. It encourages the elderly to participate in various social and family activities, which plays an important role in enhancing the self-worth of the elderly, maintaining individual physiological functions,and strengthening inter-generational friendship and solidarity. Importantly, the realization of active aging of the elderly can greatly reduce the expenditure of social care. Moreover, by making the best use of human capital and increasing community participation and mutual assistance, active aging also plays an important role in maintaining social stability and developing the economy.3The United Nations Madrid II International Plan of Action on Agingadopted active aging and inspired policies at national, regional, and international action.“Report on ageing and health” also emphasizes the important position of active aging policy in the process of coping with the aging society.4Active aging has even been converted into a mantra in aging societies.2
The mining and analysis of the influencing factors of active aging can provide a basis for the realization of active aging on a personal level. The WHO has initially formed a model of active aging determinants, including health and social services (health promotion and disease prevention, curative service, long-term care, mental health services), behavioral factors (tobacco use,physical activity, healthy eating, oral health), personal factors (biology and genetics, psychological factors),physical environment (physical environments, safe housing, falls, clean water, clean air, and safe food),social environment (social support, violence and abuse,education, literacy), and economic factors (income,social protection, work), which are embedded in cultural and gender contexts.1This model has aroused much attention and controversy among scholars.5Many of the determinants proved to be entwined, reflecting the transaction between individual and environmental factors in shaping adaptation to the aging process.6Some of these determinants are policy issues that need to be actively addressed by the government, such as the promotion and integration of health and social services and the construction of suitable aging environments. Some factors have been demonstrated by many studies as good, healthy behavior, and the construction of an aging environment will inevitably make active aging easier to achieve.
Gender and age differences affect the active aging situation.7The younger the elderly, the higher the level of active aging.8–10However, the effect of gender on active aging is controversial.2,11Regarding physical environment and economic factors, a high level of education,8,9,12,13good economic condition,8,14the absence of chronic disease,8,14,15,and abundant family support15are linked to high active aging levels. However, specific results vary across studies in different populations.
Good daily living ability and the absence of depressive symptoms have also been classified as indicators of active aging.11Pham et al. found that active aging is positively associated with perceived health, life satisfaction, and quality of life and negatively associated with falls, loneliness, and frailty.16A 6-factor model (i.e.,health, psychological component, cognitive performance, social relationships, bio-behavioral component,and personality) was formed through interviews with 1322 old people living in the community. Findings reinforced the importance of psychological functioning in active aging in the oldest old.6,17Active aging is strongly consistent with low depressive symptoms.18
However, due to transportation, language, funding, and other obstacles, the research and promotion of active aging are mostly concentrated in urban areas,involving very few in rural areas. Furthermore, inequalities in the development of health care and social services are apparent among Western countries,19African countries,20,and China.21The situation of the elderly in rural areas requires more attention.
Therefore, this study aimed to explore the level and factors associated with active aging in rural areas of Xiangtan County, China, and to provide health management suggestions to the health service sector for the rural elderly.
2. Methods
2.1. Design
This research involved a cross-sectional and descriptive study conducted in rural areas of Xiangtan County,China.
The research site of this study was located in rural areas of Xiangtan County, Hunan Province, Southeast China. According to the 2018 national economic and social development statistics bulletin, the total number of people in Xiangtan is 2.865 million, of which 0.61 million (21.3%) were aged 60 years and older.22The average life expectancy of the Xiangtan area is 78.63 years,which is higher than the national and provincial average levels. In summary, aging is a very important and burning social realistic issue in the region.
Considering previous data showing 36.67% satisfaction of rural elderly pension status23and according to the formula n = (Zα/2)2×P(1−p)/δ2, taking α = 0.05,Zα/2= 1.96, δ = 10% ×P, andP= 37%, the sample size was 654 cases. Considering the possible loss of samples, the sample size was increased by 20%. Hence, the sample size should be at least 785 cases.
Multistage sampling was adopted. First, according to the per capita annual income of farmers, 17 towns in Xiangtan County were divided into 3 levels: good,medium, and poor. In each level, a township was selected by the random number method. Three towns were selected: Shitan Town (2220 USD per year), Fenshui Town (1855 USD per year), and Zhonglupu Town(1609 USD per year). In each town, 3 villages were selected by random number simple sampling. Finally, 9 administrative villages were selected as the source of the survey objects.
Old adults were recruited in the study if they (1) were aged 60 years or over, (2) continuously lived in the local area for >1 year, and (3) were clear-minded and able to communicate effectively. Residents in hospitals or nursing homes were excluded from the survey.
2.2. Measurements
2.2.1. General information sheet
A general information sheet was used to collect demographic and general health data, including gender, age,education, marital status, living arrangement, number of children, subjective economic status, and number of chronic diseases.
2.2.2. Assessment of active aging
The positive aging questionnaire (PAEQ) compiled by Hu Min et al. in 2012 was used to evaluate the active aging level. The questionnaire was developed based on the concept of active aging and its three pillars, with the aim of developing an individual-level instrument for measuring active aging. The overall Cronbach’s α coefficient of the questionnaire was 0.914. The overall semi-reliability of the questionnaire was 0.801. The content validity of the questionnaire was analyzed by the expert judgment method, and the Content Validity Index (CVI) was 1. The correlation between each dimension and the total questionnaire ranged from 0.137 to 0.888, and the construct validity was good in Hu’s study.24The overall Cronbach’s α coefficient of the questionnaire in this study was 0.862. The assessment includes physical vitality (i.e., the physical activity of the elderly), life satisfaction (i.e., the spiritual and cultural aspects of the elderly and the status of their own life satisfaction), family support (i.e., family members, friends,or social groups to support and help the elderly), and active participation (i.e., the participation of the elderly in social activities and social services) in 4 dimensions.The assessment included 21 items that involved the use of a 5-point scoring method from “completely inconsistent” (1 point) to “fully qualified” (5 points); the median number is 3. Entries with scores of ≤1, ≥2 but <3, ≥3 but <4, and ≥4 indicate low, moderately low, moderately high, and high scores, respectively. The total score may range from 21 to 105 points, with scores of ≤42, >42 but≤63, >63 but ≤84, and >84 indicating low, medium–low,medium–high, and high levels of active aging, respectively. A high score indicates a high level of active aging.
2.2.3. Assessment of activities of daily living
Activities of daily living were measured using the activity of daily living scale (ADL) developed by Lawton and Brody in 1969.25It consists of the physical self-maintenance scale and the instrumental activities of daily living scale. The first part includes 6 items, namely, walking,eating, dressing, grooming, bathing, and toilet use. The second part is an instrumental daily living ability scale that consists of 8 items, namely, using transportation,cooking, doing housework, taking medicine, doing laundry, shopping, using of phone, and administration of their economy. Choices for each item were graded“1 = can do it myself,” “2 = have some difficulty doing,”“3 = need help to do it,” and “4 = cannot do it at all”. The total score of ADL represents the different dependence degrees of the elderly: ≤14 indicates the normal ability of daily living, whereas >14 indicates partial limitation of the ability of daily living. The Cronbach’s α of ADL was 0.918 in this study.
2.2.4. Assessment of depressive symptoms
The depression in old-age scale (DIA-S) was used to measure symptoms of depression. It was compiled by Heidenblut and Zank, designed specifically for the elderly,26and has been used in Germany and Iran.27,28The scale included 10 depression-related items that were to be answered with true or false with a yes/no answer format. The scale ranges from 0 (no depressive symptoms) to 10 (maximal number of depressive symptoms). The total maximum score is 10. A cut-off of ≥3 was considered an indication of depressive symptoms.High scores suggest high levels of severe depressive symptoms. Yang Bing et al.29produced a translated version of the DIA-S in Chinese. The Chinese DIA-S has a total Cronbach’s coefficient of 0.829, a split-half reliability of 0.831, a retest reliability of 0.907 and a content validity index (S-CVI/UA) of 0.9. The content validity index (I-CVI) of item level was 0.833–1. The average content validity index (S-CVI/Ave) was 0.983,and the Pearson correlation coefficient between each entry and the total score was 0.475–0.789. The coefficient of the internal consistency of the scale was 0.787 in this study.
2.3. Procedure of data collection
After unified training and assessment, 3 investigators entered the home of the elderly in the countryside and conducted face-to-face investigations with the assistance of the staff in each village. Given the common characteristics of poor eyesight and low education of the elderly in rural areas, the survey was conducted in the form of face-to-face interviews, and all data were recorded by investigators. Approximately 20–30 min were taken to complete a questionnaire.After the investigations were concluded, respondents were thanked for their participation and given some incentives, such as a pack of food. The data collectors performed the necessary checking and verification procedures in time after the participants had completed the questionnaire.
2.4. Data analysis
Information from the questionnaires was typed into a computer by 2 researchers according to the serial numbers. SPSS 19.0 was used for data analysis. Categorical variables (gender, age, education, marital status, number of children, subjective economic status, and number of chronic diseases) were presented as frequencies and percentages, whereas continuous variables (positive aging level, activities of daily living, and depression symptoms) were expressed as mean ± standard deviation (SD). Self-care dependence and depressive symptoms in the elderly were also measured as percentages.A single samplet-test was used to compare the mean scores of PAEQ between the study and that of Cao’s.12Independent samplet-test and ANOVA were applied to examine the difference in active aging level among sociodemographic variables.
Correlations between PAEQ score, ADL, and depressive symptoms were analyzed using Pearson’s correlation analysis. Multiple linear regression was used to explore the influential factors affecting the level of active aging of rural elderly. In the study,P-values <0.05 were considered significant.
3. Results
3.1. General characteristics of the participants
A total of 945 rural elderly were investigated, 10 of which stopped answering due to time shortages during the investigation. Finally, 935 valid questionnaires (98.9%)were collected. Among the participants, 477 (51.0%)were males, and 437 (46.8%) participants were aged 60–69 years. Most of the participants had primary education or below (76.8%, n= 718), married and with a living spouse (70.8%, n= 662) and had 2–3 children (68.8%,n= 643). With regard to financial status, 477 (51%) respondents reported that they were in a fair financial status. In terms of health, 511 (54.6%) participants suffered from 2 or more types of chronic diseases, as shown in Table 1.
评价课堂效率是否高,看一种教学改革是否成功,重要的不是看学生在课堂干什么,而是看学生在课外干什么。如果学生在课外不是预习就是做作业,整天忙于文化课学习,其课堂效率一定不高。提高课堂效率的目的,是让学生在课外有更多的时间从事社团活动和社会实践活动,发展爱好、特长,提高核心素养。
3.2. Descriptive analysis of activities of daily living
The results showed that 44.7% (n= 418) of the elderly suffered from impaired activity of daily living. A higher number of older adults were impaired in instrumental daily living (n= 412, 44.1%) than in self-maintenance ability (n= 177, 18.9%), as shown in Table 2.
3.3. Symptoms of depression in the elderly in rural areas
Of those surveyed, 19.7% (n= 184) reported symptoms of depression. Furthermore, 29.5% (n= 276) of older people found difficulty in relaxing, whereas 23.2% (n= 217)recently (nearly 2 weeks) felt spiritless (Table 3).
3.4. Levels of active aging and its associations with demographic characteristics
A descriptive analysis of active aging is presented in Table 4. The average score of active aging among the rural elderly was 72.81, which belongs to the medium upper level.
The mean scores of the 4 dimensions (physical vitality, life satisfaction, family support, and active participation) of PAEQ were 3.28 (SD = 0.98, scale range 1–5),3.70 (SD = 0.78, scale range 1–5), 4.40 (SD = 0.94,scale range 1–5), and 2.81 (SD = 0.95, scale range 1–5), respectively. The total score and dimensions of life satisfaction and physical vitality were significantly lower than those in Cao’s findings12(P< 0.001).
The results of the correlation analysis among the independent variables and active aging are summarized in Table 5. Significant differences in active agingwere found for gender (t= 2.404,P= 0.016), education (F= 15.348,P< 0.001), marital status (F= 13.687,P< 0.001), number of children (F= 11.484,P< 0.001),subjective economic status (F= 73.227,P= 0.001), and number of chronic diseases (F= 61.257,P< 0.001).Furthermore, the elderly who were male, married and with living spouses, accepted higher education, had two to three children, had good subjective economic status,and had no chronic disease were more likely to be in a higher level of active aging. However, we did not find asignificant difference in active aging scores among different age groups in this study (F= 1.175,P= 0.309).
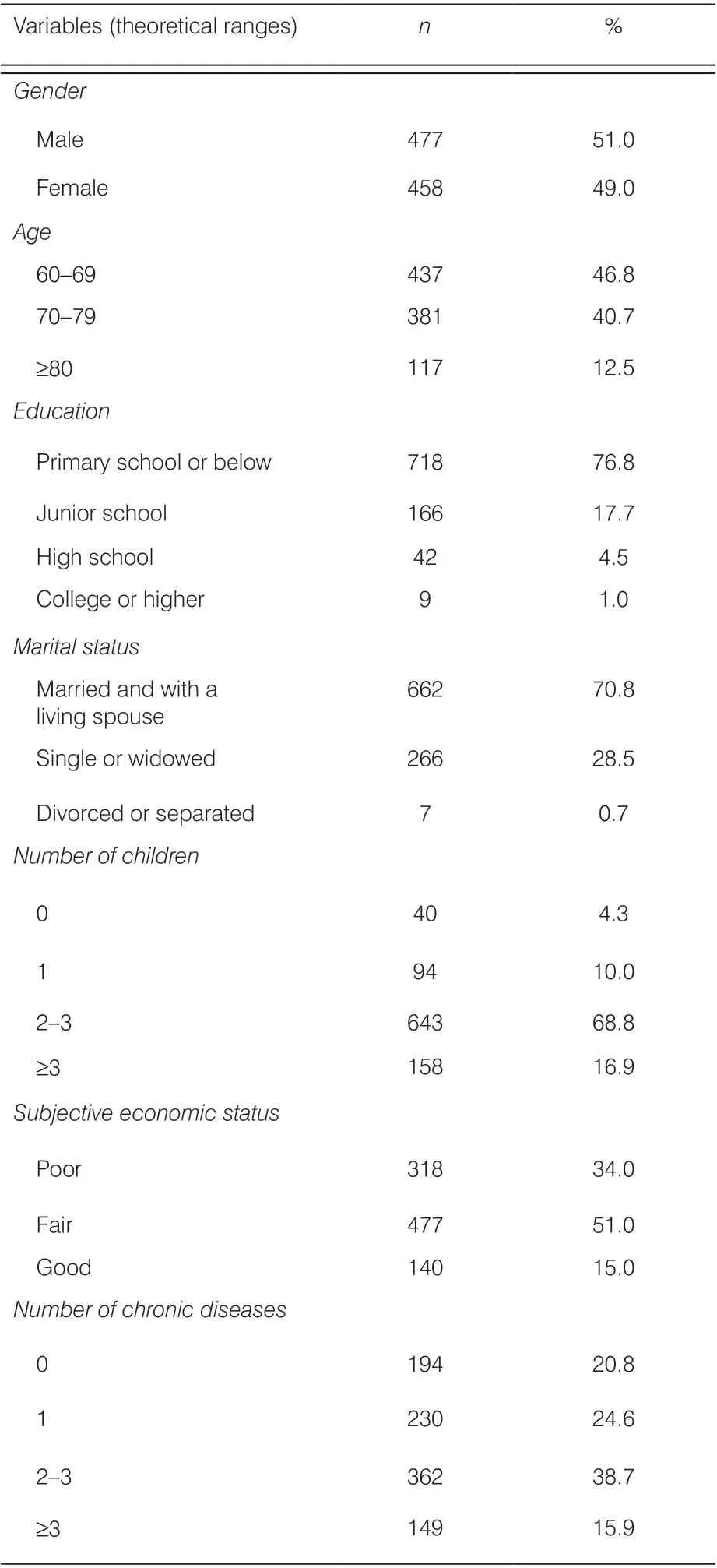
Table 1. Characteristics of participants (N = 935).

Table 2. ADL of participants (N = 935).
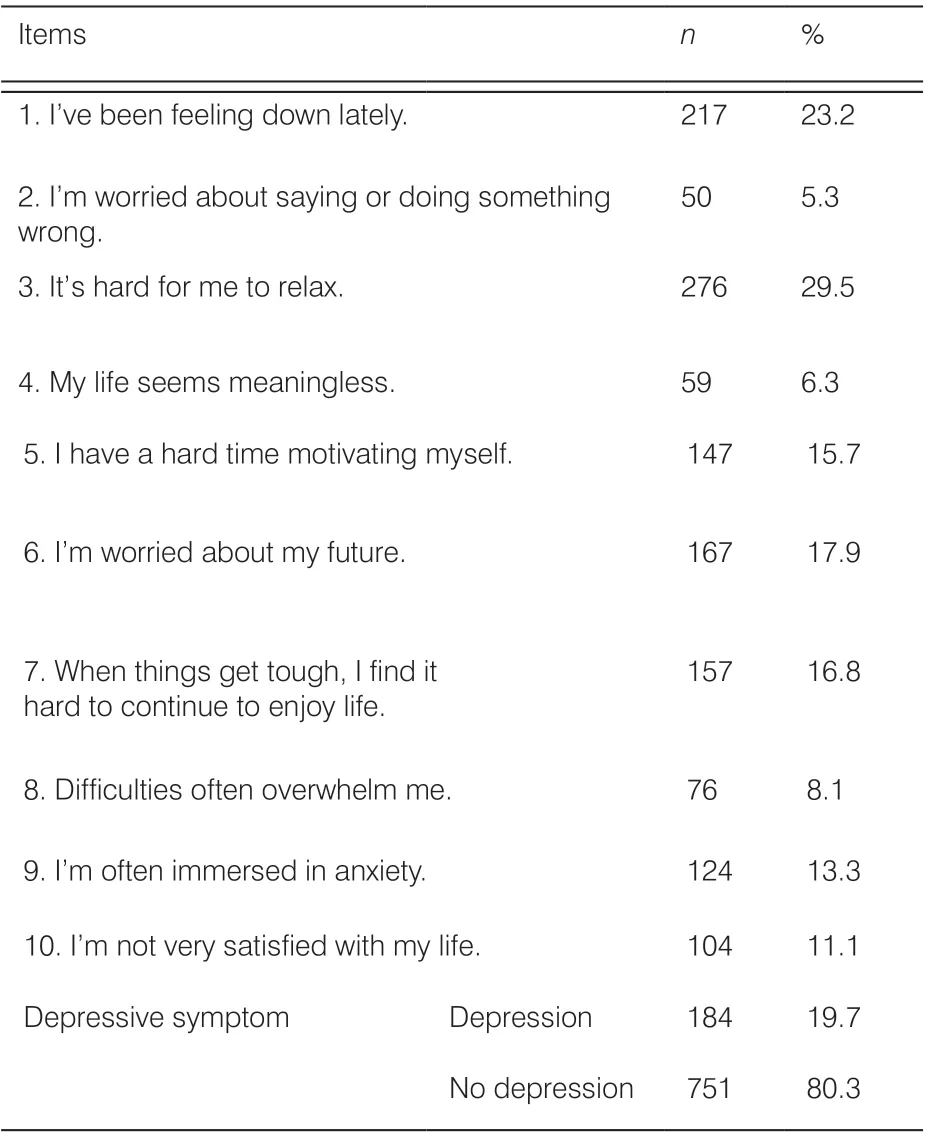
Table 3. Selection of items for symptoms of depression (N = 935).
3.5. Relationship among activities of daily living, symptoms of depression and active aging
In addition, we analyzed the correlation between active aging and activities of daily living and found a moderate negative correlation (r= −0.361). Active aging and symptoms of depression also had a moderate negative correlation (r= −0.495), as show in Table 6.

Table 4 Mean scores of dimensions of PAEQ and comparison (N = 935).
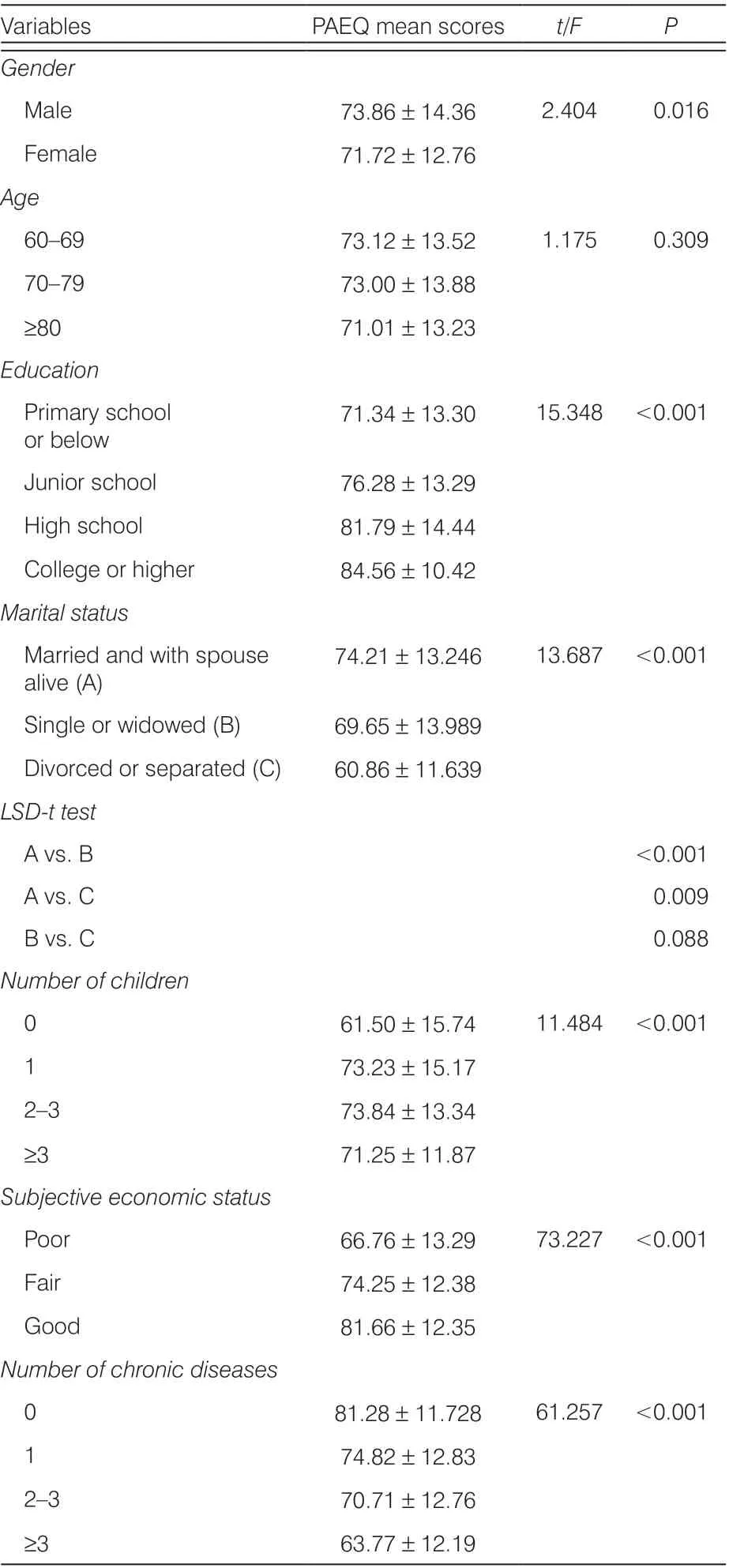
Table 5. Factors associated with active aging.
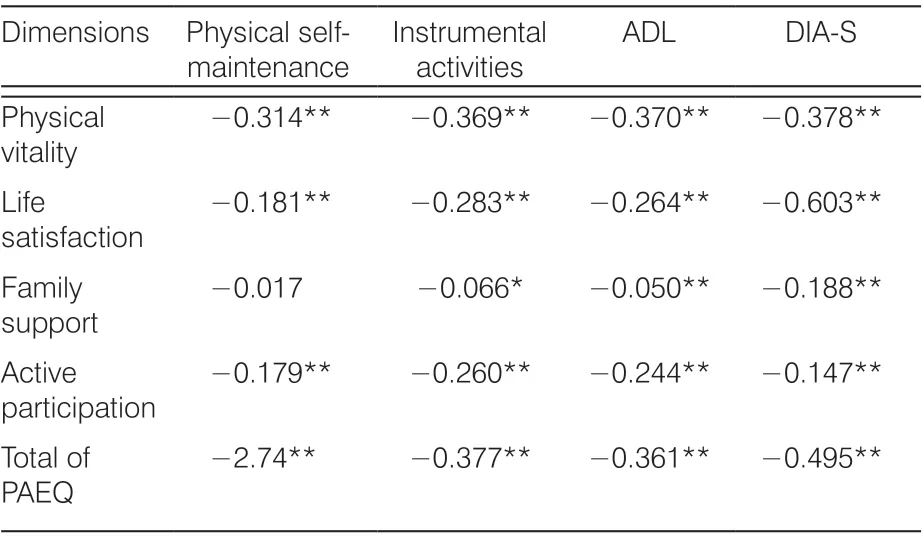
Note: ADL, activity of daily living; DIA-S, depression in old-age scale;PAEQ, positive aging evaluation questionnaire.*P < 0.05; **P < 0.01.
3.6. Multiple linear regression for active aging
Multiple linear regression models were constructed to evaluate the factors which affect active aging. In the model, total PAEQ score was the dependent variable,whereas gender, education, marital status, number of children, total score of ADL, subjective economic status, depression, and number of chronic diseases were the independent variables. The results showed that depressive symptoms (β = −0.321,P< 0.001), number of chronic diseases (β = −0.281,P< 0.001), subjective economic status (β = 0.239,P< 0.001), ability of daily living (β = −0.196,P< 0.001), education (β = 0.126,P< 0.001), number of children (β = 0.097,P< 0.001),and marital status were the influencing factors of active aging in rural elderly. The elderly with no chronic disease, low depression score, good subjective economic status, good ability of daily living, high education level,more children, married and living with spouses had a high level of active aging (P< 0.05). These results are presented in Table 7.
4. Discussion
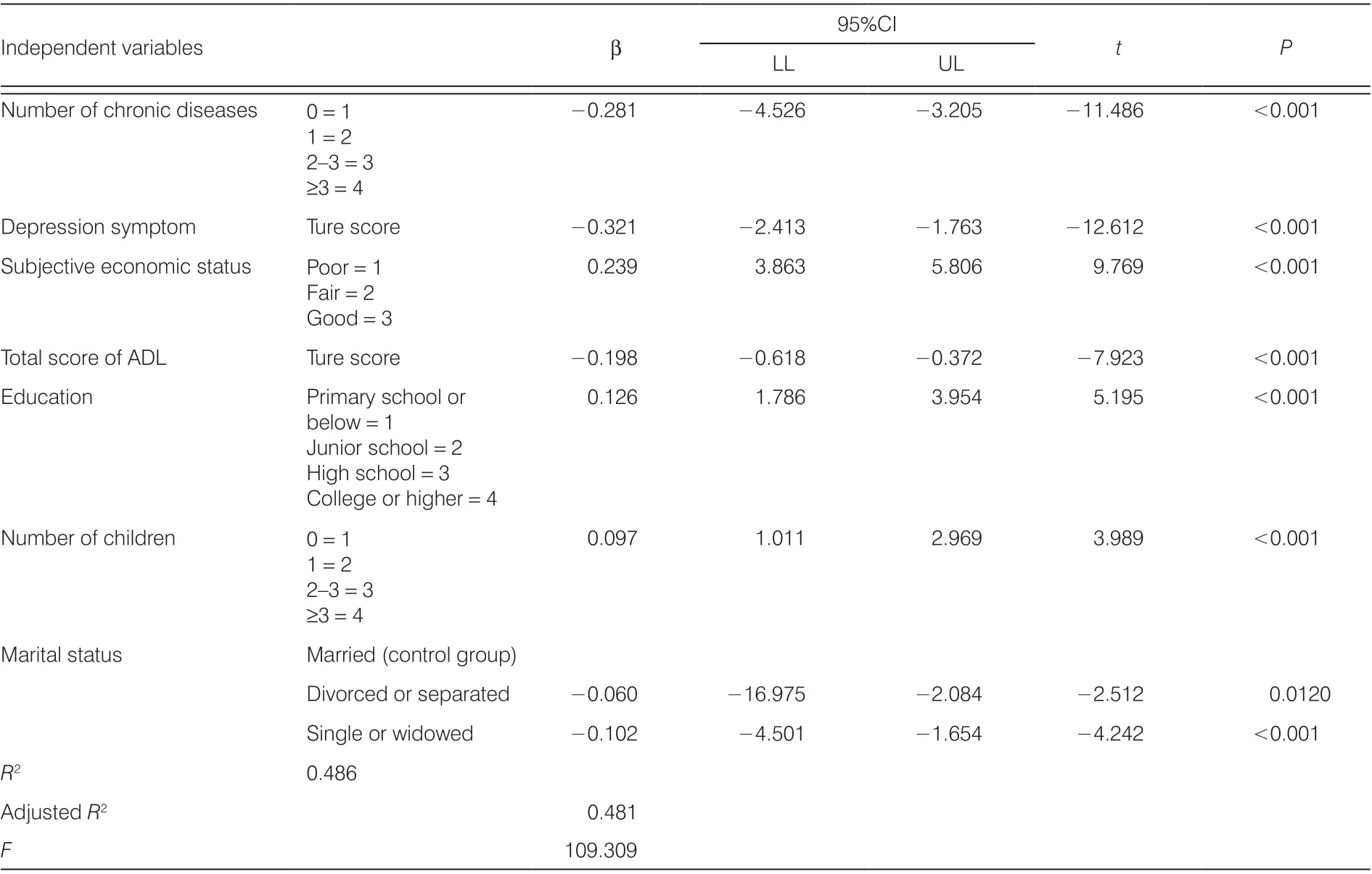
Table 7. Regression analysis of active ageing (N = 935).
Symptoms of depression showed great relevance to active aging in the present study, which is consistent with previous findings.17A good mental state may contribute to more positive attitudes toward health, facilitate functionality and enable the elderly to better integrate themselves.6The prevalence rate of depression among those aged >60 years is in the range of 11–57%.37Moreover, the proportion of untreated depressed patients in rural areas is very high – double that in cities.38According to the biological– psychological–social medical model,39health personnel should pay attention not only to the physical diseases of the elderly but also to their psychological problems. In the government’s free medical examination program for the elderly, the focus is on the assessment and examination of physiological disease. Psychological problems are ignored.As a result, mental disorders are likely under-recognized and under-treated. This situation suggests that psychological problems should be taken into account when providing health services for the elderly in rural areas.
The number of chronic diseases and ADL are also predictors of active aging. In our study, 79.3% of the elderly had one or more chronic diseases. This result may be related to the low awareness of disease prevention among the elderly in rural areas. At the same time,it is related to the narrow scope of rural primary health services. Rural primary medical care mostly focuses on the treatment of diseases. However, the publicity of knowledge on disease prevention is relatively little.Furthermore, guidance on the rehabilitation of chronic diseases is minimal. Chronic diseases seriously affect people’s quality of life due to high morbidity, disability,mortality, and high medical expenses.40–42. As chronic diseases cannot be prevented and controlled, the ability of daily life is impaired. In the study, the incidence of elderly people with impaired instrumental daily life ability is relatively high, especially in the use of public vehicles and mobile phones, which may be related to inconvenient rural transportation and underdeveloped information technology. Health is an important pillar of the concept of active aging.1The unhealthy state of the body caused by chronic diseases and the inability to participate in society caused by impaired daily life ability have greatly reduced the active aging level of the elderly in rural areas.
Subjective economic status, education level, marital status, and number of children have certain effects on active aging. This result is consistent with that of a South Korean study.16The self-perception of good economic conditions not only brings self-esteem to the elderly but also makes the elderly more likely to spend money on high-quality food, medical care, and social activities.43Thus, older people can better protect their health, maintain self-esteem at a higher level, and adopt a more positive attitude toward life. A prior study also found that active aging is higher in elderly people with a higher education level.44Elderly people with high education levels in rural areas usually have fixed jobs, retirement pension, wide social contact, and more opportunities to participate in social activities. In addition, their information literacy is also high, and they can effectively access a variety of health resources to ensure their own health.45The arrival of information society makes the realization of active aging inseparable from network technology. The establishment and implementation of information and communication technology training for the elderly can improve the satisfaction and quality of life of participants.46
Respondents who have no children, no spouse,and are living with collateral relatives are also the key objects to which medical workers should pay attention.Socio-emotional selectivity theory maintains the focus of older people’s social interactions on family relationships to enhance their positive experiences.47Influenced by traditional Chinese concepts, the rural elderly put most of their energy into the care of their families, and their emotional support mainly comes from their families. Due to their relatively closed social contacts, rural elderly have higher family needs than urban elderly.48Spouses,children, and other immediate family members are an important source of affection.
Notably, gender and age are not included in the model of influencing factor analysis. No statistical difference was found in the level of active aging between the elderly and the young (Table 5), which is inconsistent with our conventional view. The possible explanations are as follows: (1) since the concept of equality between men and women is deeply rooted in the hearts of the people, elderly women’s awareness of participation and health care has gradually improved; and (2)some elderly people were not included in our survey because they could not communicate well for various reasons. This requires further research and exploration.
The influencing factors of active aging were discussed to realize the active aging of the rural elderly at the personal level, and the direction of further efforts was defined to meet the following objectives: (1) increase the construction of the rural environment suitable for the elderly so that the rural elderly have more places for sports and fitness and to provide basic facilities for their physical health; (2) strengthen the mental and physical disease prevention propaganda of prevention and disease screening; (3) provide different security conditions according to different physical conditions of rural elderly in different areas; for example; for the elderly with poor physical condition, the government needs to adopt different forms of old-age support to ensure their dignified life; (4) create opportunities to solve the employment problem of young rural people, help rural entrepreneurs,and encourage more young people be with their parents,which can greatly reduce the labor burden of the rural elderly, enhance emotional exchange between generations, and reduce the occurrence of depression; and (5)facilitate the elderly to engage in literacy activities, not only in writing but also in the application of electronic products.If possible, skills or knowledge training can be carried out for the elderly according to their own conditions.
Active aging is rooted in healthy life and behavior in the pre-old-age period. Attention to active and healthy aging needs to be focused on middle- and young-aged populations.49Chronic diseases, depression, economic status, and education level are not just immediately acquired by the elderly but are accumulated in the young. Therefore, from another aspect, attention should also be paid to the physical health status of the young and middle-aged populations in rural areas to promote the active aging of the elderly in rural areas in the future.
5. Conclusions
The study provides a profile of active aging among Chinese rural elders in Xiangtan County. The active aging of the elderly in China’s rural areas in Xiangtan County is at a medium–upper level but lower than that of the urban elderly. The regression model indicates that depressive symptoms, ADL, number of chronic diseases, subjective economic status, and education are the most important predictors of active aging. The focus group of active aging in rural areas should be elderly people suffering from chronic diseases, physical decline, poor education and economic conditions, childlessness, and who have no partner. These results suggest some tentative recommendations for the elders,primary health personnel, and departments. A more rigorous longitudinal design is necessary to investigate the causality of the related factors and active aging.
Strengths and limitationsIn this study, the active aging questionnaire was used to investigate the active aging status of the elderly in rural areas at the personal level, and relevant information on the status quo and influencing factors of the elderly in rural areas was provided. The results provided not only suggestions for the elderly in rural areas to achieve active aging and improve the quality of life but also direction on the elderly work of primary health workers. The research also provides a certain reference value for the implementation of an active aging policy for the rural elderly.
We affirm that the study has certain limitations. First,the research object only consisted of 9 villages and towns in Xiangtan County, and the results can only have a certain reference value. Second, because it is only a cross-sectional survey, the causal relationship between various influencing factors and active aging is difficult to explain.
Acknowledgments
This study received strong support from Xiangtan County Civil Affairs Bureau, Shitan Township Civil Affairs Office,Fenshui Township Civil Affairs Office, and Zhonglupu Township Civil Affairs Office. We thank all the research participants for their kind participation.
Ethical approval
This study was approved by the Ethics Review Committee of Behavioral Medicine and Nursing Research of Xiang-ya Nursing School, South-Central University China (No. 2019013). All the participants and their families gave their informed consent before the survey. The researcher also emphasized to potential participants that they had the right to refuse to participate or to stop participating at any time. The questionnaires were recorded anonymously, and no information regarding identity was collected.
Conflicts of interest
All contributing authors declare no conflicts of interest.
猜你喜欢
故事作文·低年级(2021年11期)2021-11-28
作文通讯·初中版(2020年8期)2020-09-27
作文周刊·小学一年级版(2020年36期)2020-09-17
21世纪商业评论(2019年9期)2019-10-12
快乐语文(2018年10期)2018-06-05
中国学校体育(2018年8期)2018-05-14
高中生学习·高三版(2017年3期)2017-03-23
湖北教育·综合资讯(2017年2期)2017-03-17
东方女性(2016年4期)2016-04-28
人生十六七(2014年35期)2014-02-28
- Frontiers of Nursing的其它文章
- Predictors of nurse’s happiness:a systematic review
- Redefining the concept of professionalism in nursing: an integrative review
- Clinical nursing competency assessment:a scoping review
- Moderating effect of psychological resilience on the perceived social support and loneliness in the left-behind elderly in rural areas†
- Effects of progressive muscular relaxation and stretching exercises combination on blood pressure among farmers in rural areas of Indonesia: a randomized study†
- Visualization analysis of research“hot spots”: self-management in breast cancer patients†