
Color change after tooth bleaching with ozone and 10% ozonized carbamide peroxide for in-office use
2022-11-05 11:05ThalytadosReisFurlaniZouainFerreiraNevesDiasFranciscoUbiratanFerreiradeCamposCeciliaPedrosoTurssiFlviaLucisanoBotelhodoAmaralFabianaMantovaniGomesFranRobertaTarkanyBasting
Medical Gas Research 2022年3期
Thalyta dos Reis Furlani Zouain Ferreira Neves Dias, Francisco Ubiratan Ferreira de Campos, Cecilia Pedroso Turssi,Flávia Lucisano Botelho do Amaral, Fabiana Mantovani Gomes França, Roberta Tarkany Basting
Faculdade São Leopoldo Mandic, Campinas, São Paulo, Brazil
Abstract There is a constant search for bleaching treatments that can offer greater safety with fewer adverse effects, especially in the techniques performed in the office, which usually employ hydrogen peroxide in high concentrations (35% to 40%) that are not recommended by some international control agencies.This in vitrostudy evaluated the color change after tooth bleaching with the use of ozone and a 10% ozonized carbamide peroxide bleaching treatment for in-office use.Thirty molars were allocated (n = 10):three applications of ozone (1 hour every 3 days); three applications of 10% ozonized carbamide peroxide (1 hour every 3 days); 10% carbamide peroxide agent (8 hours a day for 7 days).The teeth were mounted on a plaster model to simulate the dental arch, and trays made of silicone were used for the application of the bleaching agents and to allow ozone to enter through.The ozone concentration used was 60 μg/mL, with an oxygen flow of 0.25 L/min.The values of color change showed no significant differences among treatments.The variations in the parameters over time, as well as the values of ΔEab, ΔE00, and WID , showed that there was no significant difference among the three treatments.The use of ozone and 10% ozonized carbamide peroxide for in-office use was effective for tooth bleaching with clinically perceptible and acceptable color alterations.The study was approved on September 10, 2019 by the São Leopoldo Mandic Ethics Research Committee (CAAE No.17711719.4.0000.5374).
Key words:carbamide peroxide; color; color change; gas; hydrogen peroxide; ozone; ozone therapy; oxygen; tooth bleaching; whitening
INTRODUcTION
Tooth bleaching techniques use agents with different concentrations of hydrogen peroxide or carbamide for in-office or at-home treatments.1Higher concentrations of hydrogen peroxide (between 35% and 40%) are used for in-office techniques, whereas lower concentrations (up to 10% hydrogen peroxide and between 10% and 20% carbamide peroxide, which releases between 3% and 6% hydrogen peroxide), are used for techniques performed at-home by the use of trays.1
According to the American Dental Association,2products with hydrogen peroxide concentrations up to 3.5% are considered safe, whereas the Committee for Scientific Consumer Products3of the European Union approves products with up to 6.0% hydrogen peroxide.Thus, there is a need to develop safe bleaching treatments that can effectively deliver desired dental chromatic changes, especially for techniques that use concentrations higher than those recommended by control agencies.
In this respect, at-home bleaching technique using 10% carbamide peroxide can be considered a safe and effective procedure.1,4,5However, some patients do not adapt well to the use of trays, or they may still require an in-office procedure.4In case of the recommendation about using agents with low peroxide concentration, it may be useful to increase their oxidative capacity for possible use in-office for achieving effective results within a short duration after application.
Ozone is an agent that has been studied as a powerful oxidizer alone or in association with high concentrations of hydrogen peroxide in.6-10It has a short half-life and is unstable and dependent on system conditions such as temperature and pressure; therefore, it easily decomposes into pure oxygen.11In addition to its use as a medical antimicrobial and therapeutic agent,11its use in in-office bleaching techniques with agents with high concentrations of hydrogen peroxide, at 37.5%7and 38%,8-10has shown significant bleaching effects; additionally, it does not affect the mineral content of the enamel.12Furthermore, ozone bleaching has been shown to result in reduced dental sensitivity compared with the conventional in-office technique.10
By using ozone with low concentrations of bleaching agents, Manton et al.13found that applying ozone for 40 seconds did not potentiate the bleaching effect of an 8% carbamide peroxide aqueous solution, possibly because it was not used in gel form; the thickener leads to prolonged contact with the tooth surface, slowing the release of free radicals and reducing the duration of application.14,15
The concentration of hydrogen peroxide released by 10% carbamide peroxide is 10 times less than that of hydrogen peroxide used in in-office techniques.4Thus, because of the possible benefit of reduced sensitivity9,10and the potential for oxidation, the use of ozone with a bleaching gel containing 10% carbamide peroxide for in-office techniques should also be evaluated.
Therefore, the objective of this study was to assessin vitrothe effects of color change after ozone and a 10% ozonized carbamide peroxide bleaching treatments for in-office use.The null hypothesis for this study was that there are no differences between the changes in the color of teeth subjected to bleaching treatments using ozone and ozonized carbamide peroxide for in-office use compared to 10% carbamide peroxide for at-home use.
MATERIALs AND METHODs
Ethical aspects and tooth selection
Thirty healthy human third molars were selected from a dental research biorepository after the project was approved on September 10, 2019 by the São Leopoldo Mandic Ethics Research Committee (CAAE No.17711719.4.0000.5374) and stored in 0.1% thymol solution for a maximum of 6 months.12Written informed consent (Additional file 1) was obtained from the patients to provide the teeth for the experiment.
Bleaching protocols
Thirty molars were allocated by randomization into three groups (n= 10):CP group:bleaching with 10% carbamide peroxide agent (Opalescence PF 10%/Ultradent); O group:bleaching with three applications of ozone; OCP group:bleaching with three applications of 10% ozonized carbamide peroxide.The groups and bleaching protocols are presented in Table 1.The ozone concentration followed the protocol of Santana et al.7and Tessier et al.16adapted for use herein.The pH values of the 10% carbamide peroxide and the 10% ozonized carbamide peroxide bleaching agents were measured at different application times (15, 30, 45, and 60 minutes) using a pH meter (MS Tecnopon Equipamentos Especiais Ltda., Piracicaba, SP, Brazil).

Table 1:Groups, bleaching protocols, materials, and manufacturers
Tooth preparation for initial color evaluation and plaster model assembly
The allocation of the teeth to the respective groups was performed based on the initial color evaluation by the Vita Classical criterion using a spectrophotometer (VITA EasyShade Advance 4.0, Vita Zahnfabrik, BadSackingen, Germany) in order to distribute the tooth colors equally among the groups, and to avoid the risk of bias.For this, the teeth remained immersed in an artificial saliva solution (7 mL for each tooth) (1.5 mM Ca; 50 mM KCl; 0.9 mM PO4; 20 mM Tris buffer; pH = 7.0), as recommended by Featherstone et al.17and modified by Serra and Cury,18for 7 days at 37°C in a bacteriological oven.They were removed from the solution, dried with gauze, and evaluated using a closed white box to prevent the effects of external luminosity and standardization of light during the readings.The color measurements were obtained in duplicate to ensure accuracy.19The region for the assessment of color was the middle third of the buccal surface of the teeth.Based on the initial evaluations according to Vita Classical (the selected teeth had colors B3, A3.5, and A4), they were equally distributed among the three groups.Therefore, all the groups presented an equal amount of teeth with shades B3, A 3.5 and A4.At the same time, the color data forL*,a*, andb* were recorded by the CIELa*b* system for each tooth.
After the initial color analysis, the teeth were mounted on a plaster model to simulate the dental arch for the bleaching techniques.The lower arch of a dental mannequin (Prodens - Pronew, São Gonçalo, RJ, Brazil) without the artificial teeth was duplicated with special silicone (RTV-2 silicone rubber, HB FLEX 5528 - HBQUIMICA Representações, Comércio e Serviços Ltda., Custóias, Portugal).After duplication, the natural teeth were positioned in the empty alveoli.To correctly fit the teeth, the regularization of these alveoli was performed with a carbide drill 060 (Horico, Berlin, Germany).A new duplication with special silicone and casting with a special micro-granulated IV plaster (Durone, Dentsply Sirona, São Paulo, SP, Brazil) was carried out with a vacuum spatula to obtain the models.For this, each group of teeth (respective to each bleaching treatment to be evaluated) was mounted on each cast model, using 7 wax for fixing the entire root of each tooth after sealing along the dental arch of the model.This step was carried out to position and fit the teeth in the models to complete the subsequent steps.
Manufacturing the trays
Three trays made of silicone (Crystal PVC, Bioart, São Carlos, SP, Brazil) (thickness = 3 mm) were used for the application of the bleaching agents (one tray was used for each bleaching treatment).The trays were obtained after molding the plaster models in which the teeth were fixed with the use of alginate and a tray.The molds were cast with a special type IV dental plaster.For the group that would receive the 10% carbamide peroxide treatment (PC group), the tray was cut 2 mm above the gingival sulcus.For the experimental groups that were treated with ozone (O group) or 10% ozonized carbamide peroxide gel (PCO group), wearing was carried out with a number 6 spherical bur coupled to the micromotor in the end region of the vestibule, both on the outer face and the face inside the respective plaster models.A dense condensation silicone (Speedex - Coltene, Rio de Janeiro, RJ, Brazil) paste was used, and it was manipulated for the application using a thickness of 0.5 mm above the occlusal surface of the cast to make room for ozone circulation inside the tray.After the aforementioned processes, the trays were created in the vacuum plasticizer (P7, Bio-art, São Carlos, SP, Brazil) by cutting each tray at the location where wearing was previously carried out in the backend region of the vestibule.Later, four holes were drilled in the vestibular side and one hole was drilled in the lingual surface of the trays.These holes were made for installing the plastic cannulas (Macrobots Descarpack Luer Slip, San Paulo, SP, Brazil) to allow ozone to enter through the vestibular side of the trays and exit from the lingual face of the respective trays.
Bleaching treatment with 10% carbamide peroxide – cP group
A disposable syringe (Biotecmed, São Paulo, SP, Brazil) was used to apply 0.02 mL of the bleaching gel on the vestibular surface of the enamel using trays with 10% carbamide peroxide.The bleaching agent was kept on the enamel surface for 8 hours a day in an artificial saliva solution and a bacteriological oven at 37°C, according to the manufacturer’s recommendations.Subsequently, the gel was removed from the enamel surface with deionized water for 10 seconds, and the tooth was dried with gauze.Next, the model was immersed in an artificial saliva solution and kept in a bacteriological oven at 37°C.This cycle was repeated for 7 days.After the end of the applications, the enamel surface was washed with distilled water and stored again in the artificial saliva solution for 12 hours in a bacteriological greenhouse at 37°C until the final color assessments are made.
Ozone gas treatment – O group
An ozone gas generator (Medplus MX Philozon, Camboriú, SC, Brazil) was connected to an oxygen cylinder by a flowmeter standard20to the experiment.The dose adjustment was applied according to the ozone concentration and the acting time.The ozone concentration used was 60 μg/mL, with an oxygen flow of 0.25 L/min, as per the manufacturer’s specifications.The application time was 1 hour every 3 days for a total of three applications.For the ozone application, one of the ends of the cannulas was adapted to the four holes in the vestibular region of the tray, whereas the other end of the cannula was adapted to the ozone generator equipment.For the ozone output of the tray, one of the ends of the cannulas was adapted to the tray in the hole in the lingual region, whereas the other end was adapted to the ozone generator vacuum suction system (Figure 1).Between the bleaching sessions, the specimens were kept in a humid environment in a bacteriological oven at 37°C.

Figure 1:Application of ozone treatment with cannulas adapted in the tray.
10% ozonized carbamide peroxide treatment – OcP group
A disposable syringe (Biotecmed, São Paulo, SP, Brazil) was used to apply 0.02 mL of the 10% carbamide peroxide bleaching agent over the surface of the vestibular enamel of the teeth, and the tray was positioned with the previously prepared cannulas.The tray with plastic cannulas was connected to the ozone generator, as previously presented.The 10% carbamide peroxide, together with the ozone to be applied, remained on the specimens for 1 hour.This application was repeated every 3 days three times.Between the bleaching sessions, the specimens were kept in a humid environment in a bacteriological oven at 37°C.
final color analysis
The final color evaluations were performed 24 hours after completion of treatments using the Vita Classical scale and CIEL*a*b* system, as described for the initial color evaluation.
The tooth color obtained using the Vital Classical scale was converted to numerical values (1 to 16) as previously reported.4,19Lower numerical values represented brighter teeth.The color change (ΔEab) obtained by the CIELabsystem was calculated using the following formula21:ΔEab* = [(ΔL*)2+ (Δa*)2+ (Δb*)2]1/2, where ΔL=Lfinal–Linitial; Δa=afinal–ainitial; Δb=bfinal–binitial.The color change was also assessed by CIEDE2000 (ΔE00), which is based on hue and chroma values,22and the Whiteness Index for Dentistry (WID), in which the parametersL*,a*, andb* are used in transmittance analysis according to the following equation:WID= 0.511L* – 2.324a* – 1.100b*.23
statistical analysis
Since the data did not meet the assumptions of the one-way analysis of variance, they were analyzed by generalized linear models, considering the design of repeated measures forL*,a*,b*, and the color values using the Vita Classical scale.The data fromWIDwere not adjusted to a known distribution.The non-parametric Kruskal-Wallis tests were used to compare the groups, and the Wilcoxon test was used for time comparison (WID).The data for ΔL, Δa, and Δbwere not adjusted to a known distribution, and they were analyzed using the non-parametric Kruskal-Wallis test.Generalized linear models were also used, considering the treatment factor, to analyze ΔEab, ΔE00, and ΔWID.R (R Core Development Team 2020, Vienna, Austria) and SAS (SAS Institute Inc., Cary, NC, USA) were used for the analyses, assuming the level of significance of 5%.
The values for ΔEababove 2.7 were considered clinically acceptable.24,25The values for ΔE00of 0.8 and 1.8 were adopted as thresholds for the perceptibility and acceptability criteria.24The thresholds for ΔWIDwere 0.72 for perceptibility and 2.60 for acceptability.26
REsULTs
pH values
The pHs of the bleaching agents evaluated at different times (Table 2) were similar and close to neutrality within 60 minutes.There was a slight decrease in pH values for the 10% ozonized carbamide peroxide throughout the period evaluation (from 7.43 to 7.21) while the 10% carbamide peroxide remained at 7.43 during this time.
cIEL*a*b*, Vita classical and WID results
For the color variable (Table 3), there was no significant association between the groups and the times (P> 0.05); there were also no significant differences among the three groups (P> 0.05).For all treatments, there was a significant increase in the parametersL* (teeth became lighter) andWID(teeth became whiter) and a significant decrease in a* (teeth became less red),b* (teeth became less yellow), and in the Vita Classical scale (an average change of 10 shade colors).
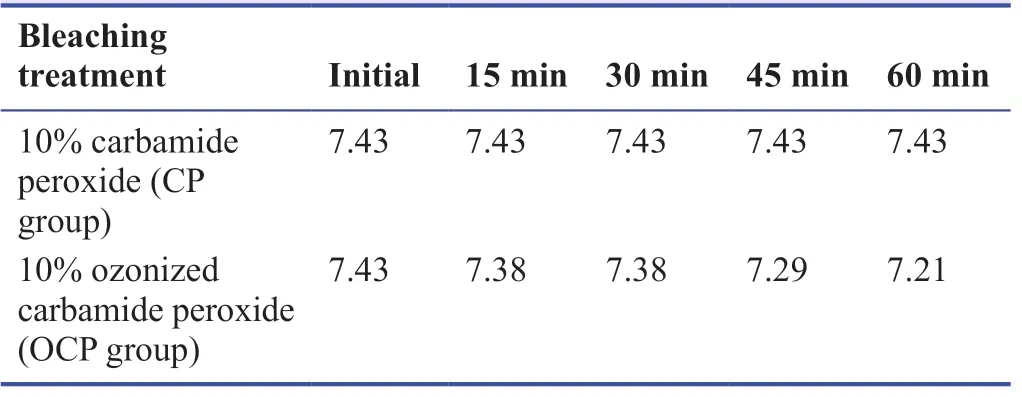
Table 2:pH values according to treatments and evaluation times
color change (ΔL*, Δa*, Δb*, ΔEab, ΔE00 and ΔWID) results
The variation of parameters L*, a*, and b* over time (Table 4), as well as the values of ΔEab, ΔE00and ΔWIDshow that there was no significant difference between the groups (P> 0.05).
DIscUssION
The data from this study shows that all the evaluated treatments delivered effective tooth bleaching, thus accepting the null hypothesis.Carbamide peroxide (10%) in tray is recognized for its bleaching effectiveness due to its potential for color change4,5and its safety.4The results showed that it had significant effects on the brightness parameters (L*), the reduction of reddish (a*) and yellowish (b*) hues, an average change of 10 shade colors based on the Vita Classical scale, and a clinically perceptible color change by CIEL*a*b*, CIEDE2000, and WID, even with use for 7 days, which was less than what is usually employed clinically (about 14 days of use1, depending on the initial color of the teeth (longer protocol for darker teeth, and shorter for lighter teeth).The values of ΔEabwere > 2.7,24,25and they were considered clinically perceptible.This was also observed for the values of ΔE00andWID, which were above the limits of perceptibility and acceptability,23,24denoting the teeth bleaching effectiveness during 7 days of treatment.Some authors reported that the isolated use of ozone did not promote effective bleaching6,13,27; however, this study showed that ozone promoted tooth bleaching with the same effective-ness as 10% carbamide peroxide bleaching treatment in tray.
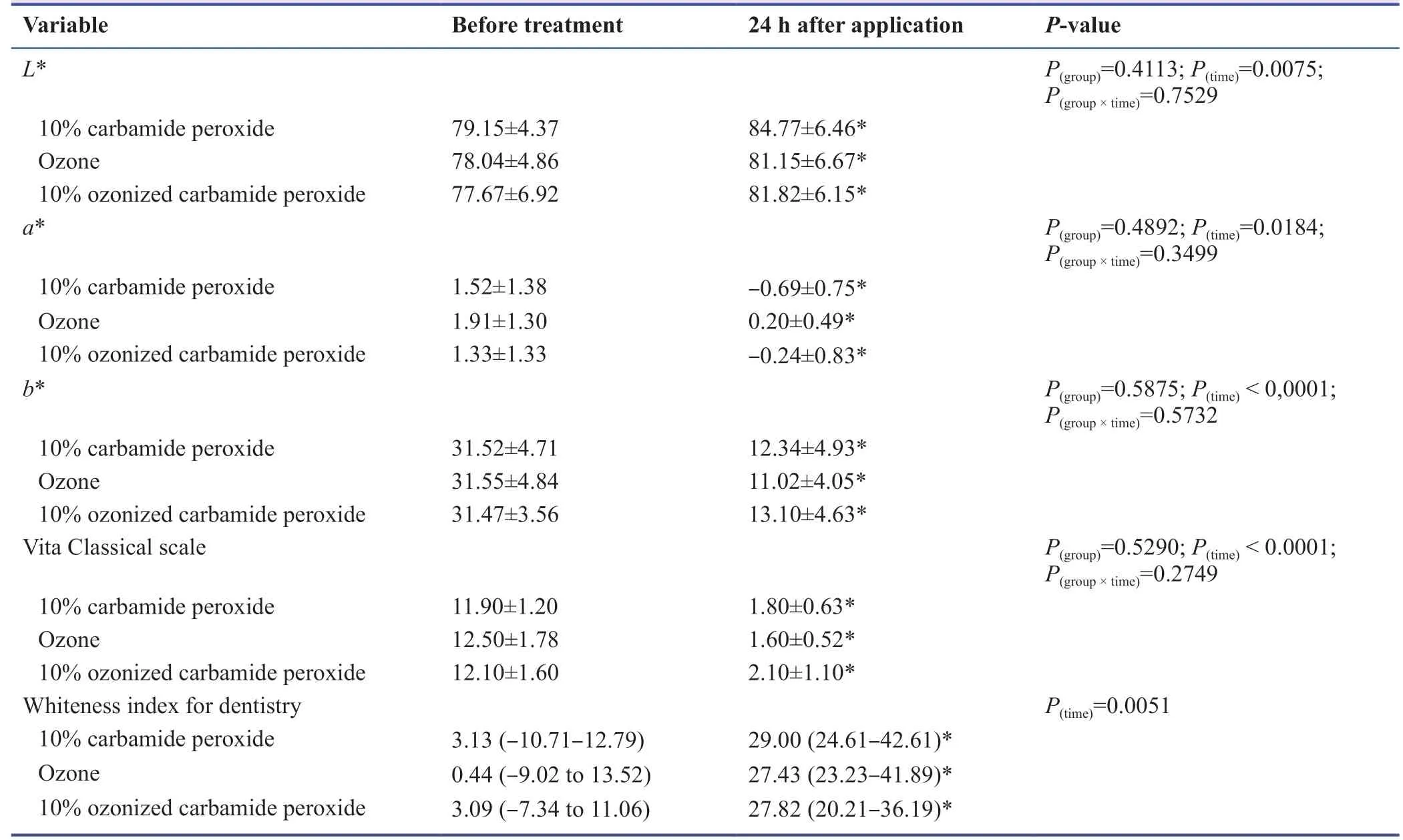
Table 3:color parameters, Vita classical scale and Whiteness Index for Dentistry depending on the treatments or groups and the evaluation times

Table 4:Variation in color based on the parameters L*, a*, and b* by cIELab, cIEDE 2000, and WID systems according to different treatments or groups
The differences in results reported by different studies can be justified by factors that influence the oxidative effect of ozone.Factors such as reduced ozone application time – from only 40 seconds,134 minutes in the group where only ozone was applied, and 80 seconds repeated three times in the group where ozone and a bleaching gel were used6– can justify such results.Another factor that may contribute to the ineffectiveness of ozone in bleaching with the use of trays is the design of the trays used.Adjusting the trays to the dental structures (as a “well-fitted” tray) restricts the free flow of ozone, preventing the direct contact of ozone with the vestibular surface of the anterior teeth.27Thus, there is the need to ensure internal relief for effective ozone circulation inside the trays, as performed in this study.
In addition to these factors, the ozone concentration of 140 ppm used in the Ozotop unit in the study by Zanjani et al.6can be cited; the lack of suction capacity limited the use of a higher concentration of ozone.It was also found that the isolated application of ozone was effective in bleaching tetracyclinestained mouse teeth by using it for 3 and 5 minutes.16
Ozone is produced naturally from oxygen via molecular photodissociation in activated oxygen atoms, which react with other oxygen molecules.This radical transitional anion quickly becomes protonated and generates hydrogen trioxide, which, in turn, decomposes into an even more powerful oxidizer, the hydroxyl radical, giving ozone gas a higher oxidizing potential.28This effect may justify the minimal reduction in the pH of ozonized carbamide peroxide after 60 minutes (from 7.43 to 7.21).In addition, chromophore groups present in the tooth structure can be broken down by ozone to form smaller molecules, resulting in tooth bleaching via one of the following three mechanisms:a) bonding mechanism, which occurs by the double bonding of ozone to form ozonide in the presence of non-aqueous solvents; however, if water is present, ozone is hydrolyzed to other products by cleaving the double bond that would have occurred; (b) a replacement mechanism, where an atom or functional group is replaced by another; (c) a cleavage mechanism, in which a carbon-carbon link is separated to produce organic composite fragments.11,20
Aqueous ozone facilitates a high level of biocompatibility in oral epithelial human cells, gingival fibroblast cells, and periodontal cells,11,20while gaseous ozone makes the inhalation toxic to the lungs and other organs28; thus, a suitable system for application of ozone as a bleaching agent is required.20Administration in gaseous form requires a sealing and suction system to avoid inhalation and adverse effects,29like the trays that were developed and adapted for this study.In this respect, it was ensured that ozone remained in constant flux on the enamel structure with direct application, which may also have contributed to the significant results of color change.In contrast with other studies that used other types of systems, such as machines, in which the lack of suction capacity limited the use of a higher ozone concentration,6or the use of a rectangular box with side openings for input and output7and trays with an unsuitable design that did not allow the continuous circulation of ozone over the teeth.27Because of the significant difference between the proposed treatments, the use of ozone appears to have advantages for shorter application durations to the dental structure and the absence of cytotoxic effects on the pulp over the use of agents containing peroxide.10
This type of tray could have led to dehydration of the teeth during the application of ozone (which enables a “false bleaching” at the end of the procedure), but the evaluation was performed after damping the teeth in artificial saliva for 24 hours.Clinically, dehydration during in-office bleaching may also be related to sensitivity,30but some clinical studies report that the application of ozone or its combination with bleaching agents can minimize this effect.9,31
The combination of ozone and 10% carbamide peroxide gel applied in the in-office treatment has proven effective in teeth bleaching, although not better than the results of the other evaluated bleaching treatments.Only ozone may have been effective for bleaching since it was applied using the tray, and it remained in contact with the occlusal and lingual surfaces of the teeth, where the effect of carbamide peroxide applied to the vestibular faces was minor or absent.Some studies have shown that the use of low concentrations of hydrogen peroxide (between 6% and 20%)32,33or carbamide (between 15% and 40%)34for in-office use is unsatisfactory given the borderline or minimal color change, unless they were associated with the use of light.35On the other hand, the use of low peroxide concentrations has been a safety recommendation for bleaching procedures1; and control agencies have recommended gels in lower concentrations.36Ozone appeared to satisfactorily facilitate tooth bleaching when combined with 10% carbamide peroxide for in-office application; clinically perceptible values in the ΔEab, ΔE00, andWIDparameters were obtained.
Other studies that combined ozone with bleaching agents did not show the enhancement of bleaching compared with ozonefree bleaching treatments,13not even after employing different ozone application times (4 or 19 minutes, respectively) in combination with 35%10or 37.5%11hydrogen peroxide.Al-Omiri et al.8suggested that ozone enhanced the bleaching response after application for 60 seconds immediately after the application of 38% hydrogen peroxide, in addition to keeping this mix for another 20 minutes on the teeth.In another study, Al-Omiri et al.9described this potentiation in their study that applied 38% hydrogen for 20 minutes and ozone for 60 seconds.
This study suggests that ozone may have potentialized the 10% carbamide peroxide bleaching because it was applied for a shorter duration (total 3 hours of application) than in case of the conventionally applied carbamide peroxide for the 8 hours every day group (which totaled 56 hours of application).However, the benefits and costs of applying each treatment should be considered.
According to the pH value analysis, neutrality was maintained within 60 minutes; however, there was a slight decrease in values, which was possibly associated with the free radical release.Although the use of ozone alone or in combination with low concentration carbamide peroxide for in-office dental bleaching following the adopted protocols facilitated favorable changes in color, they must be evaluated in clinical trials to not only prove their effectiveness but also their safety of use.28It is important to consider the potential for soft tissue irritation, sensitivity of teeth, and acceptance of treatment by patients.It can be concluded that ozone and 10% ozonized carbamide peroxide for in-office use could promote tooth bleaching with clinically perceptible and acceptable altered chromaticity.
Author contributions
Study conception and design:RTB; data acquisition:TRFZFND, FUFC, CPT, FLBA, FMGF; data interpretation:TRFZFND, FUFC, RTB; data analysis:CPT, FLBA; manuscript writing:TRFZFND, FUFC, CPT, RTB; manuscript revision:CPT, FLBA, FMGF.All authors approved the final version of the manuscript.
conflicts of interest
The authors have no financial, economic, commercial, and/or professional interests related to the topics presented in this manuscript.
Open access statement
This is an open access journal, and articles are distributed under the terms of the Creative Commons AttributionNonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.©Article authors (unless otherwise stated in the text of the article) 2022.All rights reserved.No commercial use is permitted unless otherwise expressly granted.
Additional file
Additional file 1:Informed consent form (template).
- Medical Gas Research的其它文章
- Current research progress of isoflurane in cerebral ischemia/reperfusion injury:a narrative review
- Comparative analgesic, hemodynamic, pain and duration of sensory and motor block effects of dexmedetomidine, granisetron, and nitroglycerin added to ropivacaine in intravenous anesthesia for forearm surgeries:a randomized clinical study
- Effects of different fresh gas flows and different anesthetics on airway temperature and humidity in surgical patients:a prospective observational study
- Hydrogen-rich bath with nano-sized bubbles improves antioxidant capacity based on oxygen radical absorbing and inflammation levels in human serum
- In vivo microelectrode monitoring of real-time hydrogen concentration in different tissues of rats after inhaling hydrogen gas
- spuriously low end tidal carbon dioxide in capnometry:Nafion tube malfunction in end tidal carbon dioxide module blamed for near mishap!