
Heparin-binding protein combined with human serum albumin in early assessment of community-acquired pneumonia: A retrospective study
2023-09-24 05:44JingLiuYingZhangYuWeiLuoYiYuHongShuoWangBinLiuYanTaoZheng
Journal of Acute Disease 2023年4期
Jing Liu ,Ying Zhang ,Yu-Wei Luo ,Yi-Yu Hong ,Shuo Wang ,Bin Liu✉ ,Yan-Tao Zheng✉
1Department of Emergency,Zhujiang Hospital,Southern Medical University,China
2Clinical Laboratory,The Third Affiliated Hospital of Southern Medical University,China
ABSTRACT Objective:To investigate the application of heparin-binding protein along with albumin (HBP+ALB) in evaluating the severity of community-acquired pneumonia (CAP) and compares it with single HBP,white blood cells (WBCs),C-reactive protein (CRP),and procalcitonin (PCT).Methods:A total of 226 patients with CAP admitted to the Emergency Department of Zhujiang Hospital,Southern Medical University,Guangdong,China,between March 1,2021,and March 1,2022,were enrolled.The patients were grouped into two groups: mild CAP (n=175) and severe CAP (sCAP)(n=51).Patients' characteristics and laboratory data were obtained.ROC curve and the value of the area under the curve (AUC) were used to evaluate the predictive values of HBP,ALB,WBC,CRP,and PCT.Results:WBC count,CRP,PCT,HBP,creatinine,and D-dimer were higher in the sCAP group,while ALB was lower in the sCAP group (P<0.05) than those in the mild CAP group.The AUCs of WBC,CRP,PCT,HBP,and HBP+ALB were 0.633 (95% CI: 0.545-0.722,P<0.05),0.635 (95% CI: 0.542-0.729,P<0.05),0.705 (95% CI: 0.619-0.791,P<0.05),0.809 (95% CI: 0.736-0.883,P<0.05),and 0.889 (95% CI: 0.842-0.936,P<0.05),respectively.Conclusions: HBP+ALB has a higher predictive value than single HBP,PCT,CRP and WBC used alone for the early assessment of CAP.
KEYWORDS: Community-acquired pneumonia;Heparin-binding protein;Albumin;Procalcitonin;White blood cell count;C-reactive protein
1.Introduction
Community-acquired pneumonia (CAP) refers to the inflammation of pulmonary parenchyma (including the alveolar wall),occurring outside of hospital environment,including pneumonia caused by pathogens with a clear incubation period after admission[1].CAP is one of the most common infectious diseases threatening human health worldwide.It has an annual incidence of 5.16/1 000-33/1 000 in the United States[2].The in-hospital mortality rate for severe CAP (sCAP) has been reported to be 25%-50%[3].However,the severity of CAP is often overlooked by clinicians,which may lead to inappropriate treatment protocols[4].It may induce a poor prognosis.Therefore,early evaluation and diagnosis of sCAP are very important[5].
Various methods have recently been developed to assess and predict the severity of CAP.Some common scoring systems to determine the severity of CAP include the CURB-65 score,pneumonia severity index,and national early warning score[6].The CURB-65 scoring system is a relatively simple assessment tool;however,its accuracy is lower.Pneumonia severity index can more accurately stratify the severity of CAP patients;however,it is a more complex and timeconsuming calculation method[7,8].Biological markers used to predict the severity of CAP include procalcitonin (PCT),C-reactive protein (CRP),interleukin-6,and other novel or traditional biological markers[9].Heparin-binding protein (HBP) is a new inflammatory predictor,which is being increasingly used for predicting infectious diseases.HBP begins to increase immediately after inflammation or infection and can be used to predict organ failure[10].Albumin (ALB) is used as a conventional indicator of human nutritional status and systemic inflammation.Previous studies have shown that ALB is associated with mortality in CAP[11,12].In addition,human serum ALB is also closely related to the biological efficiency of antibiotics.This study investigates the application of HBP along with ALB (HBP+ALB) in evaluating the severity of CAP and compares it with single HBP,white blood cells (WBCs),CRP,and PCT.
2.Patients and methods
2.1.Study design and setting
Patients diagnosed with CAP in the emergency department of Zhujiang Hospital,Southern Medical University,Guangdong,China,were included in the study.Patients diagnosed as CAP between March 1,2021,and March 1,2022,were enrolled.
2.2.Inclusion and exclusion criteria
The inclusion criteria were as follows: (i) over 18 years of age,male or female;(ⅱ) met the international guideline diagnostic criteria of CAP;(ⅲ) completely preserved clinical data,and (ⅳ) easily available information on biochemical indicators.
2.3.Ethical statement
The study was approved by the Ethics Committee of Zhujiang Hospital,Southern Medical University,Guangdong,China.The Ethical approval number was 2022-KY-306.All methods were performed in accordance with the Declaration of Helsinki.
2.4.Definitions
The following were used as the diagnostic criteria of sCAP[13]: (i) consciousness disorder;(ⅱ) respiratory rate ≥ 30 times/min;(ⅲ) PaO2<60 mmHg,PaO2/FiO2<300,mechanical ventilation required;(ⅳ) systolic pressure <90 mmHg;(v) septic shock;(ⅵ) involvement of bilateral or multiple pulmonary lobes,or ≥50% expansion of the lesion within 48 h after admission,as shown by the chest X-ray;(ⅶ) oliguria,with a urine volume of <20 mL/h,or <80 mL/4 h,or dialysis treatment needed owing to acute renal failure.Those meeting one or more of the above criteria can be diagnosed as sCAP.Other patients can be diagnosed with mild CAP (mCAP).
HLB+ALB: We used SPSS software to merge and calculate the severity of heparin binding protein,ALB,and pneumonia,and used regression analysis to obtain a new variable.
2.5.Data compilation
General clinical data of the patients,including their name,sex,age,smoking history,and complications;information on biochemical indicators,including WBCs,CRP,PCT,HBP,ALB,creatinine (Cr),and serum sodium concentration (Na+);information on imaging examination,including pleural effusion and chest CT findings;and data on treatment,including mechanical ventilation,use of vasoactive drugs,length of stay in the hospital,and admission to the intensive care unit,were collected.The cases were grouped into mCAP and sCAP based on the diagnostic criteria of sCAP.
2.6.Statistical analysis
The SPSS statistical software was used for statistical analysis.When the measurement data conformed to the normal distribution,the mean±standard deviation was used to express the data.Thet-test was used for the intergroup comparison.The median and quartile were used for the non-normal distribution data.The Mann-WhitneyUtest was used for the intergroup comparison.Counting data were expressed in percentages.Chi-square test and Fisher exact probability test were used for comparison between the groups.The difference was statistically significant withP<0.05.MedCalc was used to draw the receiver operating characteristic curve (ROC),calculate the area under the ROC curve (AUC),and evaluate the significance of each index in predicting the severity of CAP patients.
3.Results
3.1.Comparison of baseline data between the two groups
A total of 226 patients with CAP were included in the study (Figure 1).The baseline characteristics of patients are enumerated (Table 1).Among these,138 were men and 88 were women,with an average age of (68.1±18.7) years.In addition,175 of these patients had mCAP and 51 had sCAP.The average age of the patients with sCAP was (73.1±15.9) years,higher than that of the patients with mCAP [(66.6±19.3) years],but it had no statistical significance (P>0.05).There was no significant difference among the patients of mCAP and sCAP groups in terms of sex,smoking history,complications,and pleural effusion (P>0.05).WBCs,CRP,PCT,HBP,Cr,and D-dimer of sCAP groups were higher than those of the mCAP group in the community (P<0.05).ALB of the patients with sCAP was lower than that of the patients with mCAP (P<0.05).
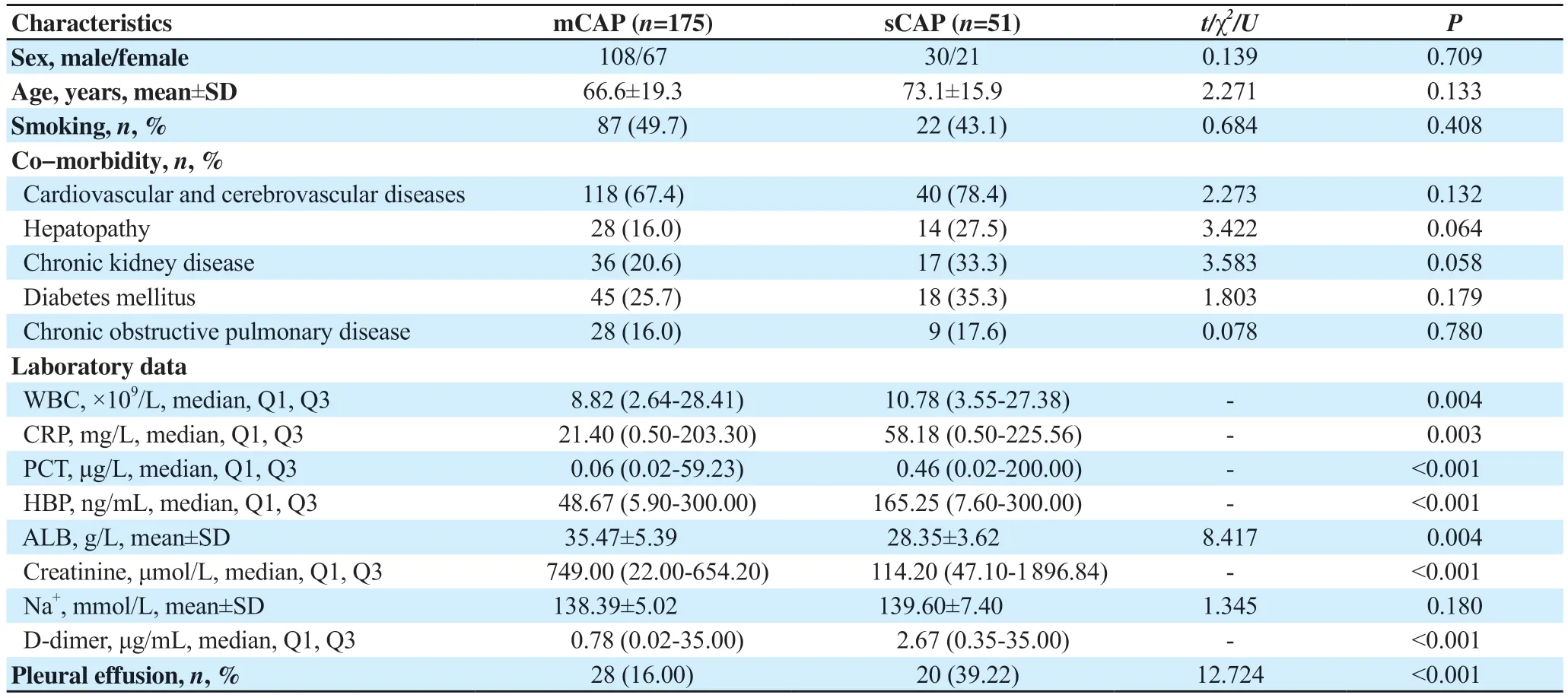
Table 1.Baseline characteristics (n=226, n,%)
3.2.Comparison of ROC curves predicted by different factors for the severity of CAP patients
Table 2 shows the ROC analysis of each inflammatory index to evaluate the severity of CAP.The ROC curve is shown in Figure 2.The AUC of the WBC score was 0.633 (95%CI: 0.545-0.722) and its truncation value was 9.7×109/L;The AUC of the CRP score was 0.635 (95%CI: 0.542-0.729) and its truncation value was 48.87 mg/L;the AUC of the PCT score was 0.705 (95%CI: 0.619-0.791) and its truncation value was 0.19 μg/L;the AUC of the HBP score was 0.809 (95%CI: 0.736-0.883) and its truncation value was 99.56 ng/mL;and the AUC of the HBP+ALB score was 0.889 (95%CI: 0.842-0.936).

Table 2.ROC analysis of inflammatory markers to predict the severity of CAP.
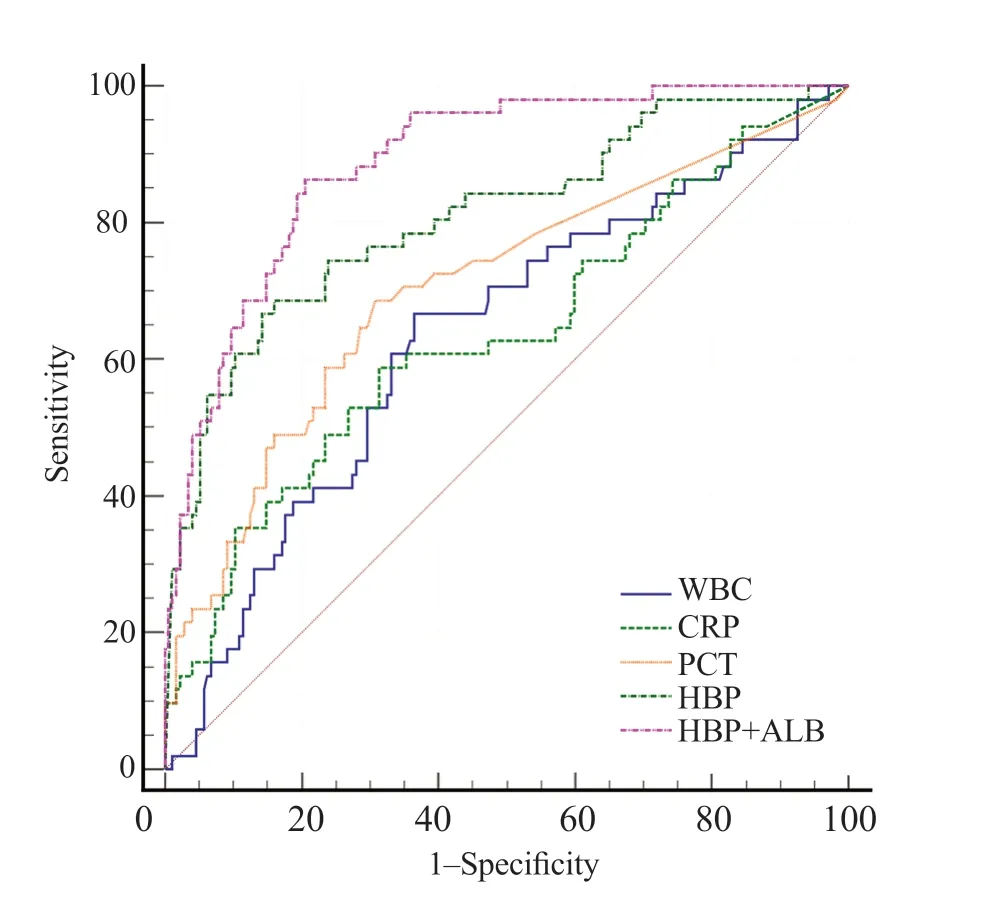
Figure 2.ROC curve for predicting the severity of CAP,WBC,white blood cell;CRP,C-reactive protein;PCT,procalcitonin;HBP,heparin-binding protein;ALB,albumin;HBP-ALB: heparin-binding protein-albumin.
4.Discussion
CAP is an acute pulmonary infection caused by a variety of pathogens.The morbidity and mortality of CAP in developing countries are much higher than those in developed countries.Its immunopathology is characterized by an acute lower respiratory inflammatory response regulated by cytokines or other inflammatory mediators[14].It is currently recognized as one of the major public health problems.It has been identified as the third most common cause of death worldwide.The annual incidence of CAP in the elderly has been reported to be 0.33%-4.6%[15,16].sCAP is induced by the aggravated inflammatory reaction in the lung tissue and has high morbidity and mortality[3,17].Therefore,timely and effective assessment of the condition of CAP patients and the formulation of a reasonable and effective diagnosis and treatment plan is very important.
In this study,the levels of HBP+ALB in patients with CAP were compared with those of the patients with other inflammatory markers (HBP,WBC,CRP,and PCT).sCAP patients were older than those of the mCAP patients.In addition,WBCs,CRP,PCT,HBP,Cr,and D-dimer of sCAP patients were higher than those of the mCAP patients.The level of ALB of patients with sCAP was lower than that of the patients with mCAP.CRP increases in all infections,stress reactions,and tumor diseases.This study found that the AUC of CRP for predicting the sCAP was 0.635.But a recent study conducted by Chenet al.[8]found that the concentration of CRP in patients with mCAP was not significantly different from that in patients with sCAP.Therefore,more clinical studies are needed to confirm the predictive value of CRP in CAP.
PCT,secreted by parathyroid C cells,comprises 116 amino acids and can be detected 2 h after infection[18].Studies have shown that PCT has a good diagnostic value in predicting the severity and prognosis of CAP.HBP,also known as azuroxine or cationic 37 kDa antibacterial protein (CAP37),is a multifunctional immunomodulatory protein[19].It has extensive antibacterial activity.In addition,it shows chemotaxis and can activate monocytes and macrophages.It can also increase vascular permeability,which plays an important role in the prediction of infectious diseases.HBP is an important player in the pathophysiology of organ dysfunction induced by sepsis[10].HBP is a marker of nonspecific systemic inflammatory reaction.CAP caused by various pathogens can be increased in the early stage,and the degree of increase is positively correlated with the degree of inflammatory reaction.Therefore,HBP of sCAP is significantly higher than that of mCAP.Huanget al.demonstrated that the level of plasma HBP significantly increased in children with sCAP on admission and that HBP may be a better predictor of disease progression in children with sCAP than routine biomarkers[14].In this study,the AUC for HBP for predicting the sCAP was 0.809.
Patients with sCAP were predicted to have more WBCs than the average number (AUC: 0.633) and PCT (AUC: 0.705),which was similar to that reported by Caiet al.[20].ALB is the main protein of the human plasma and is synthesized by the liver,which plays an important role in the inflammatory response and oxidative stress.The synthesis of ALB significantly decreased in the acute phase of the inflammatory reaction.Release of inflammatory mediators and chemokines increases the permeability of the cell membrane,resulting in ALB loss through its leakage from capillaries[21,22].Leeet al.demonstrated that ALB is an independent risk factor in 28-day mortality in patients with CAP,with an odds ratio of 0.37[23].Mehulet al.conducted a prospective study and showed that the ratio of blood urea nitrogen to ALB is an independent risk factor for poor prognosis in CAP[24].
We found that HBP+ALB was superior to HBP,PCT,CRP,and WBC in the diagnostic prediction of the severity of CAP.This study is a retrospective analysis of the clinical data of 226 patients with CAP,which showed that HBP+ALB is highly valuable in the assessment of CAP severity (AUC: 0.889).In fact,HBP+ALB has a higher predictive value than that of HBP alone (AUC: 0.709).Both HBP and ALB can be obtained directly from laboratory indicators without conducting any further calculations.It also helps to avoid any increase in the financial burden of patients.
In summary,HBP combined with ALB at admission can predict the severity of CAP.Clinicians can evaluate the severity of CAP based on the level of HBP+ALB,and then make an early diagnosis and propose appropriate treatment.However,this study failed to completely rule out the interference of the test results of patients with CAP who had been treated with antibiotics and other drugs outside the hospital,and further research is still needed.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Authors’contributions
JL,YZ,and YWL contributed to the conception and design of the study,data analysis and interpretation,and the drafting and substantial revision of this manuscript.YYH and SW contributed to the acquisition of data.YTZ and BL revised the manuscript and design of the study.All authors read and approved the final manuscript.
 Journal of Acute Disease2023年4期
Journal of Acute Disease2023年4期
- Journal of Acute Disease的其它文章
- Biochemical indicators and the Peradeniya Organophosphate Poisoning scale in prediction and prognosis of organophosphorus poisoning: An observational prospective study
- Clinical profile of febrile encephalopathy patients at a tertiary care hospital in India: A retrospective study
- Effects of long COVID-19 among young adults in Turkey: A crosssectional study
- Epidemiology of animal bite injuries in North of Fars province in Iran
- Clinical and epidemiological features of pelvic fractures presenting to the emergency department in a tertiary health care hospital in south India: A retrospective study
- Central venous catheterization-related complications in a cohort of 100 hospitalized patients: An observational study