
急性冠脉综合征非手术治疗患者血清尿酸及B型纳尿肽水平与GRACE评分的相关性及其预测价值
2016-06-21 15:12刘京锋王学东
实用医院临床杂志 2016年4期
刘京锋,汪 钰,王学东
(北京市和平里医院CCU病房,北京 100013)
急性冠脉综合征非手术治疗患者血清尿酸及B型纳尿肽水平与GRACE评分的相关性及其预测价值
刘京锋,汪 钰,王学东
(北京市和平里医院CCU病房,北京 100013)
目的 探讨非手术治疗的急性冠脉综合征(acute coronary syndrome,ACS)患者的血清尿酸(UA)及B型钠尿肽(BNP)水平与全球急性冠状动脉事件注册(GRACE)评分的相关性及对远期预后的预测价值。方法 未行手术治疗的ACS患者291例,入院后立即测定其血清尿酸及BNP水平,根据GRACE评分将患者分为高危组95例、中危组121例和低危组75例,随访发病6个月的主要心血管不良事件(MACE)的发生情况,分析UA、BNP水平与GRACE评分间的相关性及三者对MACE发生的预测价值。结果 高危组UA及BNP高于中危组及低危组,差异有统计学意义(P< 0.01),UA、BNP均与GRACE评分呈线性正相关。结论 非手术治疗的ACS患者血清UA及BNP水平与GRACE评分呈正相关;血清UA、BNP水平及GRACE评分可有效预测MACE的发生风险。
急性冠脉综合征;尿酸;BNP;GRACE评分
急性冠脉综合征(acute coronary syndrome,ACS)是最常见的致死性冠状动脉粥样硬化性心脏病[1],主要包括不稳定性心绞痛、非ST段抬高心肌梗死和ST段抬高心肌梗死三类。国内大多数ACS患者仍为药物保守治疗[2],早期对这些患者进行风险评估,有助于指导后续的诊疗过程并评价预后[3]。血清尿酸(uric acid,UA)是嘌呤代谢的副产物,其升高可能会促进ACS进展[4,5]。B型钠尿肽(B-type natriuretic peptide,BNP)主要是由心肌细胞分泌,能够反映心肌缺血程度和心功能情况[6]。近年来,全球急性冠状动脉事件注册(global registry of acute coronary events,GRACE)评分在多项研究中表现出对ACS患者住院死亡和出院后6个月内死亡的预测能力[7,8]。本研究探讨非手术治疗的ACS患者血清UA、BNP水平与GRACE危险评分的相关性,及其对6个月内主要心血管不良事件(major adverse cardiac event,MACE)的预测价值。
1 资料与方法
1.1 一般资料 2010年7月至2014年12月就诊于我院心内科和CCU的ACS患者297例。入选标准:①符合美国ACC/AHA 2006年发布的ACS诊断和治疗指南[9]中的诊断标准;②年龄18岁以上的男性或非妊娠期女性;③未经手术且不准备行手术治疗;④均签署知情同意书。排除标准:①既往心肌梗死患者;②急慢性心功能不全,左室射血分数小于45%;③存在严重的肝、肾、肺疾病或重症感染、肿瘤等;④存在心脏瓣膜病、心肌病、肺栓塞;⑤既往心房纤颤史或起搏器植入术后;⑥近半年内重大外伤、手术史。
1.2 方法 采集患者人口学信息、冠状动脉疾病相关危险因素、既往病史及生命体征等资料。患者入院后3小时内以EDTA抗凝管采集肘静脉血,分离血清,于-70 ℃冰箱中保存,检测血清UA、BNP、肝肾功、血常规等,计算每例患者的GRACE评分。6个月后以门诊随访和电话随访相结合的方式进行随访。
1.3 观察指标 终点事件为发病6个月内的MACE事件,包括:心源性死亡、非致死性心肌梗死、心力衰竭、再发心绞痛等。其余在随访过程未能观察到患者出现终点事件的记为截尾。根据GRACE危险评分分组、UA、BNP正常与否分组,统计各类MACE发生情况。
1.4 统计学方法 采用SPSS 20.0统计软件进行统计分析。计量资料以均值±标准差表示,组间差异的比较采用单因素方差分析;计数资料以率表述,采用卡方检验;相关性分析中方差齐的计量资料采用Pearson相关,方差不齐采用Spearman秩相关。P< 0.05为差异有统计学意义。
2 结果
2.1 基线情况 6例患者在6个月随访时因无法联络脱落,共有291例患者进入最后分析。患者年龄45~89岁,其中男169例,女124例,不稳定型心绞痛145例、非ST段抬高心肌梗死93例和ST段抬高心肌梗死53例。既往高血压病165例,2型糖尿病107例,高脂血症53例。有吸烟史者192例,饮酒史者178例。根据GRACE评分危险等级分组,其中低危组(<108分)75例,中危组(108~140分)121例,高危组(>140分)95例。高危组UA及BNP高于低危组,BNP高于中危组,差异均有统计学意义(P< 0.01),见表1。

表1 基线情况比较
*与低危组比较,P< 0.01;#与中危组比较,P< 0.01
2.2 MACE发生率 6个月随访时,共有70例(24.05%)患者发生MACE。GRACE危险评分中危组及高危组的MACE发生率显著高于低危组(中危组:χ2=8.047,P< 0.01;高危组:χ2=19.051,P< 0.001; UA升高组MACE发生率高于UA正常组(χ2=14.766,P< 0.001); BNP升高组MACE发生率高于正常组(χ2=8.791,P= 0.003),见表2。
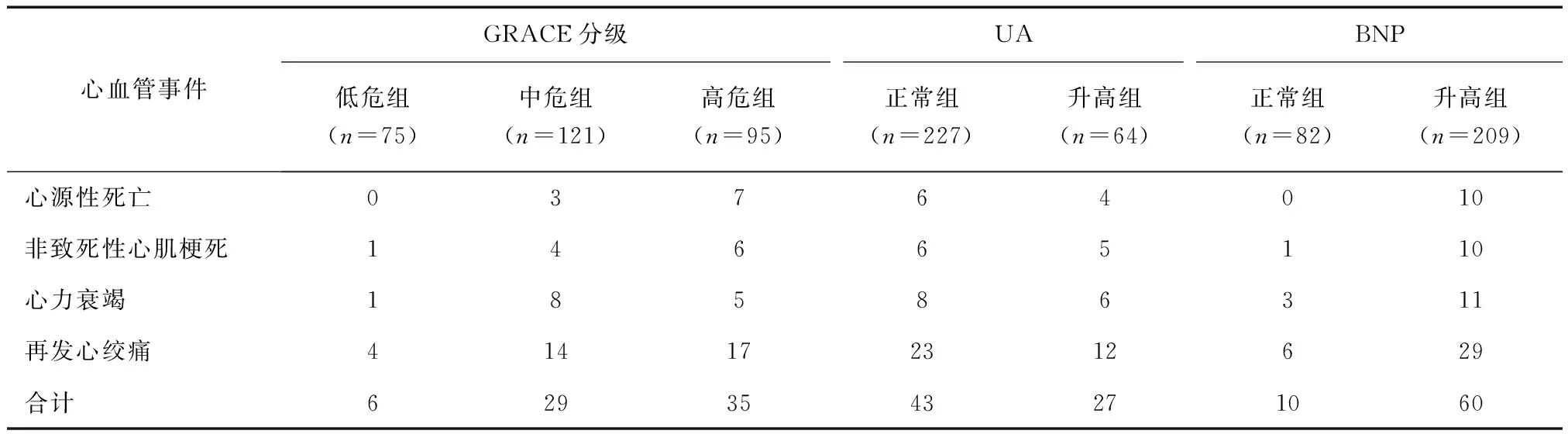
表2 患者发病6个月时MACE比较 (n)
2.3 UA、BNP与GRACE评分的相关性分析 非手术治疗的ACS患者的UA及BNP水平与GRACE危险评分均呈线性正相关(r=0.204,r=0.733,均P< 0.001),即随着患者UA或BNP水平的升高,其GRACE危险评分的分层也提高。
3 讨论
ACS一直是临床研究和循证指南关注的重点[10]。欧美最新的国际指南均推荐从急诊室接诊便对患者进行风险评估,筛选出MACE事件高危患者[11,12],进行重点关注和治疗,从而改善患者预后。考虑到国内多数基础医院并无开展冠脉造影或介入手术的资质及发病就诊延迟的存在[13,14],大部分ACS患者是未接受手术治疗的,因此本次研究将目标人群定在内科保守治疗的ACS患者。
目前,临床中评价ACS患者风险的有方法有GRACE危险评分、TIMI评分和PURSUIT评分等,相对其他方法,GRACE风险评分能更好地评估MACE的风险[15]。但由于缺少对神经体液因素及氧化应激反应的指标,难以涵盖ACS患者复杂的临床病情,从而影响GRACE危险评分的推广应用。
UA作为OX通路活性的生物标志物,一定程度上能反映冠脉血管氧化应激损伤程度[16],近年来被多项研究证实在多种心血管疾病中具有显著的预测价值[17,18]。BNP作为心室细胞分泌的重要神经体液指标,近年来逐渐被重视。Bassan等[19]的研究显示心肌梗死及周围区域缺血损伤心肌细胞BNP的合成与分泌增加,BNP能在一定程度上反映心肌缺血的程度。Radwan等[20]的研究发现BNP与左室射血分数及TIMI评分密切相关,有一定预后判断价值。
本研究发现,对于未行手术治疗的ACS患者,不同的GRACE危险分组的MACE发生率存在显著差异,随着GRACE评分的增高,MACE的发生率逐渐升高。而UA及BNP水平与GRACE危险评分呈正相关性,可以从神经体液因素及氧化应激反应的指标的角度进一步补充GRACE危险评分,可在临床中进一步推广应用。
综上所述,对于未行手术治疗的ACS患者在入院时进行GRACE危险评分,并进行UA及BNP的检测,能更为全面地评估发病6个月内MACE事件的发生可能。但考虑到本研究是在单中心进行,且样本量有限,可能存在选择偏倚。同时由于条件限制,未选择更长半衰期的氨基末端B型利钠肽前体(NT-proBNP)作为检测指标以更为准确的评价BNP水平,对未来应开展多中心、大样本的研究,选择更为适宜的检测方式进一步探索非手术治疗的ACS患者MACE事件风险预测指标。
[1] Amabile N,Hammas S,Fradi S,et al.Intra-coronary thrombus evolution during acute coronary syndrome:Regression assessment by serial optical coherence tomography analyses [J].Annales de Cardiologie et d'Angéiologie,2013,62(12):374-375.
[2] Swahn E,Alfredsson J.Invasive Treatment of non-st-segment elevation acute coronary syndrome:cardiac catheterization/revascularization for all[J].Revista Espaola de Cardiología (English Edition),2014,67(3):218-221.
[3] Cannon CP,Brindis RG,Chaitman BR,et al.2013 ACCF/AHA key data elements and definitions for measuring the clinical management and outcomes of patients with acute coronary syndromes and coronary artery disease:a report of the American College of Cardiology Foundation/American Heart Association Task Force on clinical data standards (writing committee to develop acute coronary syndromes and coronary artery disease clinical data standards) [J].Journal of the American College of Cardiology,2013,61(9):992-1025.
[4] Fang J,Alderman MH.Serum uric acid and cardiovascular mortality:the NHANES I epidemiologic follow-up study,1971-1992 [J].Jama,2000,283(18):2404-2410.
[5] Sinan Deveci O,Kabakci G,Okutucu S,et al.The association between serum uric acid level and coronary artery disease [J].International journal of clinical practice,2010,64(7):900-907.
[6] Kreiger G.A basic guide to understanding plasma B-type natriuretic peptide in the diagnosis of congestive heart failure [J].Medsurg nursing:official journal of the Academy of Medical-Surgical Nurses,2007,16(2):75-79.
[7] Eagle KA,Lim MJ,Dabbous OH,et al.GRACE Investigators A validated prediction model for all forms of acute coronary syndrome:estimating the risk of 6-month postdischarge death in an international registry[J].JAMA,2004,291(22):2727-2733.
[8] Abu-Assi E,Ferreira-González I,Ribera A,et al.Do GRACE (Global Registry of Acute Coronary events) risk scores still maintain their performance for predicting mortality in the era of contemporary management of acute coronary syndromes[J].American heart journal,2010,160(5):826-834.e3.
[9] Krumholz HM,Anderson JL,Brooks N H,et al.ACC/AHA Clinical Performance Measures for Adults With ST-Elevation and Non-ST-Elevation Myocardial Infarction:A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Performance Measures on ST-Elevation and Non-ST-Elevation Myocardial Infarction) [J].Circulation,2006,47(5):236-265.
[10] Arbab-Zadeh A,Nakano M,Virmani R,et al.Acute coronary events[J].Circulation,2012,125(9):1147-1156.
[11]Amsterdam EA,Wenger NK,Brindis RG,et al.2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes:a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [J].Journal of the American College of Cardiology,2014,64(24):139-228.
[12]Roffi M,Patrono C,Collet JP,et al.2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation [J].European heart journal,2015:320.
[13]中华医学会心血管病学分会,中华心血管病杂志编辑委员会.非ST段抬高急性冠状动脉综合征诊断和治疗指南[J].中华心血管病杂志,2012,40(5):353-367.
[14]王枫岭,解金红,司荣圣,等.急诊PCI抢救急性心肌梗死在基层医院的扩展性分析[J].中国心血管病研究杂志,2005,3(6):419-422.
[15]D′Ascenzo F,Biondi G.TIMI,GRACE and alternative risk scores in Acute Coronary Syndromes:a meta-analysis of 40 derivation studies on 216,552 patients and of 42 validation studies on 31,625 patients [J].Contemporary Clinical Trials,2012,33(3):507-514.
[16]Akpek M,Kaya MG,Uyarel H,et al.The association of serum uric acid levels on coronary flow in patients with STEMI undergoing primary PCI [J].Atherosclerosis,2011,219(1):334-341.
[17]Tamariz L,Agarwal S,Soliman EZ,et al.Association of Serum Uric Acid With Incident Atrial Fibrillation (from the Atherosclerosis Risk in Communities [ARIC] Study) [J].American Journal of Cardiology,2011,108(9):1272-1276.
[18]Kojima S,Sakamoto T,Ishihara M,et al.Prognostic Usefulness of Serum Uric Acid After Acute Myocardial Infarction (The Japanese Acute Coronary Syndrome Study) [J].American Journal of Cardiology,2005,96:489-495.
[19]Bassan R,Potsch A,Maisel A,et al.B-type natriuretic peptide:a novel early blood marker of acute myocardial infarction in patients with chest pain and no ST-segment elevation [J].European Heart Journal,2005,26(3):234-240.
[20]Radwan H,Selem A,Ghazal K.Value of N-terminal pro brain natriuretic peptide in predicting prognosis and severity of coronary artery disease in acute coronary syndrome [J].Journal of the Saudi Heart Association,2014,26(4):192-198.
Correlation between serum uric acid/BNP levels and GRACE score in patients with acute coronary syndrome and its predictive value
LIU Jing-feng,WANG Yu,WANG Xue-dong
(Department of CCU,Beijing Hepingli Hospital,Beijing 100013,China)
Objective To investigate the relationship between levels of serum uric acid/B-type natriuretic peptide (BNP) and global registry of acute coronary events (GRACE) risk score in patients with acute coronary syndrome (ACS) and their predictive value for long-term prognosis.Methods The serum uric acid,BNP and GRACE were measured in 291 patients who were diagnosed as ACS and not treated by surgery.The main adverse cardiovascular events (MACE) were followed up for a six mouths.The correlation between serum levels of uric acid/BNP and GRACE scores was analyzed.The predictive value of MACE was evaluated as well.Results According to GRACE score,ACS patients were divided into high,medium and low risk groups.Serum uric acid and BNP levels in high risk group were significantly higher than that in another 2 groups (P< 0.01).The levels of serum uric acid and BNP were both linearly correlated with GRACE scores.Conclusion In ACS patients without surgical treatment,the higher levels of serum uric acid and BNP are,the higher the GRACE scores are.Serum levels of uric acid/BNP and GRACE scores are positively correlated with the risk of MACE.
Acute coronary syndrome; Serum uric acid; BNP; Global registry of acute coronary events
R541.4
A
1672-6170(2016)04-0067-03
2016-02-10;
2016-04-19)
猜你喜欢
茶道(2022年3期)2022-04-27
昆明医科大学学报(2021年6期)2021-07-31
基层中医药(2021年1期)2021-07-22
中国医学影像技术(2021年2期)2021-03-30
云南医药(2019年3期)2019-07-25
基层中医药(2018年8期)2018-11-10
中国医药指南(2017年3期)2017-11-13
实验与检验医学(2017年3期)2017-06-27
哈尔滨医药(2015年5期)2015-12-01
西南国防医药(2015年11期)2015-02-28
