
经皮穴位电刺激联合右美托咪啶对老年患者术后谵妄的影响
2020-04-03 13:33丁玲玲寇士顺王麒
中国医药导报 2020年4期
丁玲玲 寇士顺 王麒
[摘要] 目的 研究經皮穴位电刺激(TEAS)联合右美托咪啶(DEX)对老年患者术后谵妄(POD)的影响。 方法 选择2017年1月~2018年11月首都医科大学附属北京中医医院择期全麻下行椎弓根钉内固定手术的老年患者96例,依据随机数字表法将其分为DEX组(D组)和联合组(T组),每组48例。D组麻醉诱导前静脉输注DEX;T组在D组的基础上,联合使用TEAS,且两组均在手术结束前30 min停止上述处理。比较两组术后5 d内POD的发生情况、术中丙泊酚用量及术前1 d、术后1、5d神经元特异性烯醇化酶(NSE)、血清肿瘤坏死因子-α(TNF-α)、白细胞介素-6(IL-6)、超氧化物歧化酶(SOD)水平。 结果 两组谵妄发生率比较,差异无统计学意义(P > 0.05)。T组丙泊酚用量低于D组,差异有统计学意义(P < 0.05)。D组术后1、5 d NSE、TNF-α、IL-6水平高于术前1 d,SOD水平低于术前1 d,差异均有统计学意义(均P < 0.05);术后5 d NSE、TNF-α、IL-6水平低于术后1 d,SOD水平高于术后1 d,差异均有统计学意义(均P < 0.05)。T组术后1 d NSE、TNF-α、IL-6水平高于术前1 d,SOD水平低于术前1 d,差异均有统计学意义(均P < 0.05);术后5 d IL-6水平高于术前1 d,差异有统计学意义,术后5 d NSE、TNF-α、SOD水平与术前1 d比较,差异均无统计学意义(均P > 0.05)。术后5 d NSE、TNF-α、IL-6水平低于术后1 d,SOD水平高于术后1 d,差异均有统计学意义(均P < 0.05)。 结论 TEAS联合DEX并未降低老年患者POD的发生率,但可以减少术中丙泊酚用量,抑制炎性反应,降低脑损伤。
[关键词] 经皮穴位电刺激;右美托咪啶;术后谵妄;炎性反应
[中图分类号] R614 [文献标识码] A [文章编号] 1673-7210(2020)02(a)-0123-04
[Abstract] Objective To investigate the effect of transcutaneous electrical acupoint stimulation (TEAS) combined with Dexmedetomidine (DEX) on postoperative delirium (POD) in elderly patients. Methods From January 2017 to November 2018, 96 cases with elderly patients underwent pedicle screw internal fixation under elective general anesthesia in Beijing Hospital of Traditional Chinese Medicine, Capital Medical University were selected. According to the random number table method, they were devided into DEX group (group D) and combination group (group T), with 48 cases in each group. Group D was used DEX before anesthesia induction, while group T was used TEAS in combination on the basis of group D, and both groups stopped the above treatment 30 min before the end of the operation. The incidence of POD was compared within 5 d after operation. The does of Propofol was compared. Neuron-specific enolase (NSE), serum tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6) and superoxide dismutase (SOD) levels in the two groups were compared within 1 d before operation and 1, 5 d after operation. Results There was no significant difference in POD incidence between the two groups (P > 0.05). The dose of Propofol in group T were lower than that in group D, and the differences were statistically significant (P < 0.05). In group D, the levels of NSE, TNF-α, and IL-6 on 1, 5 d after operation were higher than those on 1 d before operation, while the levels of SOD were lower than that on 1 d before operation, with statistically significant differences (all P < 0.05). The levels of NSE, TNF-α, and IL-6 on 5 d after operation were lower than those on 1 d after operation, while the levels of SOD were higher than those on 1 d after operation, with statistically significant differences (all P < 0.05). In group T, the levels of NSE, TNF-α and IL-6 on 1 d after operation were higher than those on 1 d before operation, while the levels of SOD were lower than those on 1 d before operation, with statistically significant differences (all P < 0.05). The levels of IL-6 on 5 d after operation were higher than those on 1 d before operation, and the differences were statistically significant. The levels of NSE, TNF-α, and SOD on 5d after operation were not statistically significant compared with those on 1 d before operation (all P > 0.05). The levels of NSE, TNF-α, and IL-6 on 5 d after operation were lower than those 1 d after operation, while the levels of SOD were higher than those 1 d after operation, with statistically significant differences (all P < 0.05). Conclusion TEAS combined with DEX do not reduce the incidence of POD in elderly patients, but can reduce intraoperative Propofol dosages, inhibit inflammatory response and reduce brain injury.
[Key words] Transcutaneous electrical acupoint stimulation; Dexmedetomidine; Postoperative delirium; Inflammation reaction
术后谵妄(POD)是老年患者术后常见的中枢神经系统并发症,表现为术后出现急性、一过性、非特异性的意识水平、注意力、认知、感知能力改变及睡眠觉醒周期紊乱,其发生率为12%~53%[1-2],严重影响患者的术后康复、住院时间,且有进一步发展为老年痴呆的可能性[3]。既往研究显示[4-5],经皮穴位电刺激(TEAS)可以降低POD的发生,且右美托咪啶(DEX)也可以降低POD的发生率[6-7],但二者联合应用却没有报道,故本研究拟评价TEAS联合DEX对老年患者POD的预防效果,为临床提供参考。
1 资料与方法
1.1 一般资料
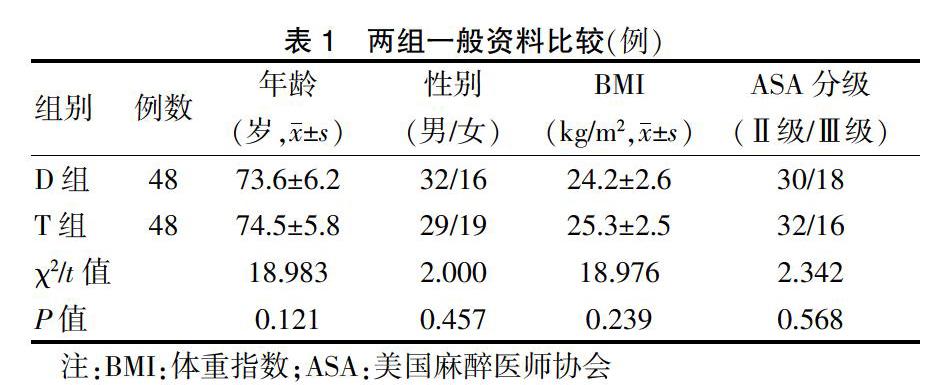
选择2017年1月~2018年11月首都医科大学附属北京中医医院(以下简称“我院”)择期全麻下行椎弓根釘内固定手术的老年患者96例。依据随机数字表法将其分为DEX组(D组)和联合组(T组),每组48例。两组一般资料比较,差异无统计学意义(P > 0.05),具有可比性,见表1。本研究经我院医学伦理委员会批准,所有受试者签署知情同意书。
纳入标准:①年龄>65岁;②预估手术时间>2 h;③美国麻醉医师协会(ASA)分级Ⅰ~Ⅲ级;③患者本人能够正常交流。排除标准:①体重指数(BMI)<18 kg/m2或BMI>30 kg/m2者;②皮肤感染、DEX应用有禁忌证者;③不愿接受TEAS、不能配合完成调查问卷者。
1.2 方法
T组:麻醉诱导前30 min给予TEAS预处理。乙醇对百会穴、神庭及双侧内关、合谷穴进行局部脱脂,不干凝胶电极贴片贴于穴位,连接LH402韩式TEAS仪(北京普康医药科技发展有限公司),频率为2/100 Hz,采用疏密波(疏波2 Hz、密波30 Hz),电流强度以患者能耐受的最大电流为适度,在3~20 mA之间调节。DEX(扬子江药业集团有限公司,批号:19010431)200 μg稀释至50 mL,以0.5 μg/(kg·h)静脉泵注10 min,再以0.3 μg/(kg·h)恒速维持。随后进行常规麻醉诱导,直至手术结束前30 min停止上述两项处理。D组:处理同方法T组,但不给予电流刺激。
麻醉诱导与维持:靶控输注丙泊酚(四川国瑞药业,批号:91A07101)使血浆靶浓度维持0.6~3.0 μg/mL,静脉注射舒芬太尼(宜昌人福药业有限责任公司,批号:90A06221)3 μg/kg和罗库溴铵(浙江仙居药业股份有限公司,批号:190504)0.6 μg/kg,气管插管行机械通气,术中根据脑电双频指数(BIS)监测及血流动力学调整麻醉深度。
1.3 观察指标
1.3.1 谵忘评定 术后5 d内两组行意识模糊评定量表(CMA)[8]包括:①意识状态急性改变或波动;②注意力障碍;③意识水平改变;④思维混乱。当①、②、③或①、②、④为阳性时,诊断为POD。
1.3.2 麻醉药用量 记录两组手术全程使用丙泊酚的剂量。
1.3.3 生化指标检测 两组术前1 d、术后1、5 d采集静脉血5 mL,酶联免疫吸附试验(ELISA)测定神经元特异性烯醇化酶(NSE,货号:ab217778)、肿瘤坏死因子-α(TNF-α,货号:ab181421)、白细胞介素-6(IL-6,货号:ab100562)、超氧化物歧化酶(SOD,货号:ab202410)水平,试剂盒均购自Abcam公司。
1.4统计学方法
采用SPSS 11.0统计学软件进行数据分析,计量资料用均数±标准差(x±s)表示,两组间比较采用t检验;重复测量资料比较采用重复测量方差分析;计数资料用百分率表示,组间比较采用χ2检验。以P < 0.05为差异有统计学意义。
2 结果
2.1 两组POD发生率及丙泊酚用量比较
D组有6例(12.5%)发生POD,T组有5例(10.4%)发生POD,两组POD发生率比较,差异无统计学意义(P > 0.05)。T组术中丙泊酚用量[(1240±26)mg]低于D组[(1430±38)mg],差异有统计学意义(P < 0.05)。
2.2 两组生化指标比较
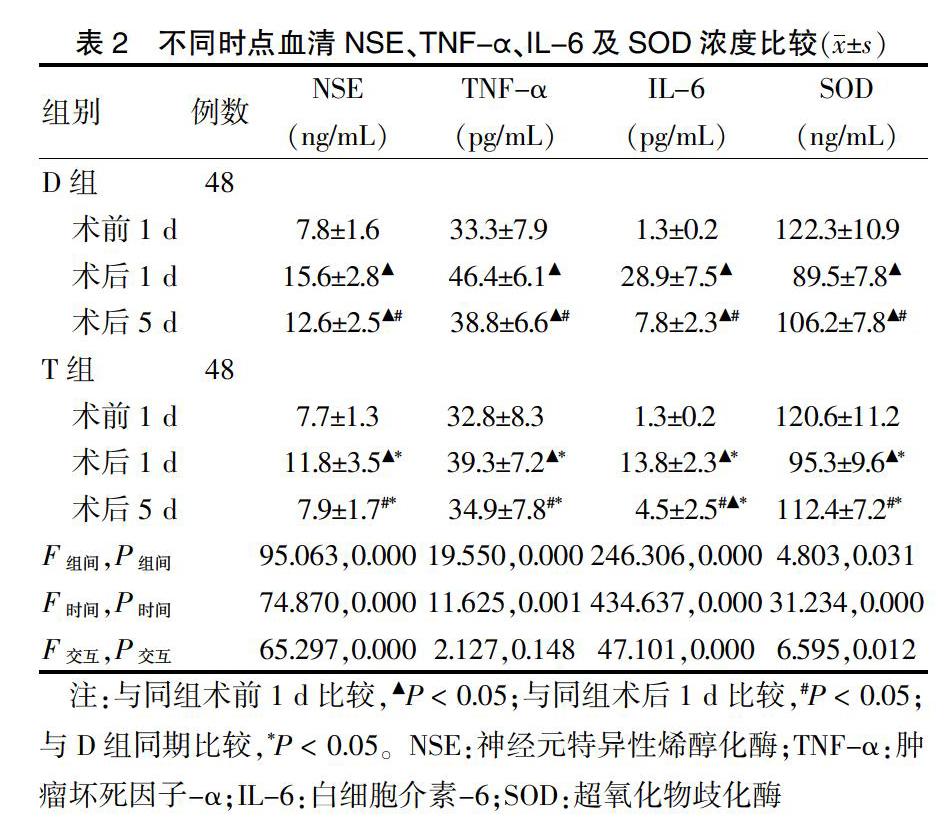
两组组间、不同时间比较,差异有统计学意义(P < 0.05); NSE、IL-6、SOD交互作用比较,差异有统计学意义(P < 0.05)。
D组术后1、5 d NSE、TNF-α、IL-6水平高于术前1 d,SOD水平低于术前1 d,差异均有统计学意义(均P < 0.05);术后5 d NSE、TNF-α、IL-6水平低于术后1 d,SOD水平高于术后1 d,差异均有统计学意义(均P < 0.05)。T组术后1 d NSE、TNF-α、IL-6水平高于术前1 d,SOD水平低于术前1 d,差异均有统计学意义(均P < 0.05);术后5 d IL-6水平高于术前1 d,差异有统计学意义(P < 0.05)。术后5 d NSE、TNF-α、SOD水平与术前1 d比较,差异均无统计学意义(均P > 0.05)。术后5 d NSE、TNF-α、IL-6水平低于术后1 d,SOD水平高于术后1 d,差异均有统计学意义(均P < 0.05)。
T组术后1、5 d NSE、TNF-α、IL-6水平均低于D组,SOD水平均高于D组,差异均有统计学意义(均P < 0.05)。
3 讨论
研究显示[9],高龄是POD的独立高危因素,年龄每增加1岁,POD发生率增加2%。近期有研究认为,POD与手术创伤应激引起的炎性反应相关[9-10]。外科手术带来的创伤会释放各种炎症介质,激活机体各种体液级联系统,增加IL-6、TNF-α等促炎因子水平,使大脑血脑屏障受损,激活大脑星形胶质细胞及小胶质细胞,导致神经不良反应,引起谵妄[10]。
针刺百会、内关、合谷穴可以改善血管性痴呆患者的认知功能,可能与改善脑血流与脑代谢功能、减少神经细胞损伤有关。百会穴有枕大神经分支,左右颞浅动、静脉和左右枕动、静脉吻合网。现代医学研究证实[11-12],针刺百会穴具有改善脑部血液循环,修复神经元,增强记忆力,抗抑郁等作用。中医学认为针刺神庭可清利头目、安神宁志,治疗与神志有关的病症。而且神庭、百会穴位置在额、颞、顶三叶的投射区,此位置与人的高级思维、记忆、精神密切相关,针刺上述穴位可以提高患者术后恢复质量[13-16]。动物试验发现[17],TEAS刺激内关、合谷穴可减轻脑缺血大鼠模型的脑水肿程度,降低术后认知障碍的发生率,改善预后。DEX是美托咪啶的右旋异构体,是一种新型的高选择性α2肾上腺素受体激动剂,在大脑及神经保护方面有一定作用。有研究显示[18-22],突触后α2肾上腺素受体具有增强前额叶皮质活动、调节注意力和行为,与谵妄的发病有关。CAM[8]简单实用,已成为临床使用最广泛的谵妄评估工具,且多作为POD的评估诊断工具。该量表具有高敏感性和特异性,适用于非精神心理专业的医生和护士筛查譫妄[8,24],可间接反映中枢神经系统损伤的程度,是特异性的生化指标之一[25],是检测神经元死亡数量的有效指标,是神经元受损的直接标志物[25]。
本研究结果提示TEAS联合DEX可以减少丙泊酚用量,降低血清炎性因子水平。虽然TEAS联合DEX可以减轻中枢神经元损伤但并未降低老年患者POD发生率,这可能与本研究选择DEX有关,因为DEX改善POD的作用明显[18-19],可能使得TEAS的作用不是很明显,也可能与本研究样本量偏小有关,期望今后能开展大样本多中心的进一步研究探讨。
[参考文献]
[1] Bryson GL,Wyand A. Evidence based clinical update:general anesthesia and the risk of delirium and postoperative cognitive dysfunction [J]. Can J Anaesth,2006,53(7):669-677.
[2] Silverstein JH,Timberger M,Reich DL,et al. Central nervous system dysfunction after non-cardiac surgery and anosthesia in the elderly [J]. Anesthesiology,2007,106(3):622-628.
[3] Aldecoa C,Bettelli G,Bilotta F,et al. European Society of Anaesthesiology evidence-based and consensus based gui-deline on postoperative delirium [J]. Eur J Anaesthesiol,2017,34(4):192-214.
[4] 张陈麟,朱玲丽,严栋.电针对老年患者全身麻醉术后认知功能恢复的影响[J].上海针灸杂志,2015,34(2):132-134.
[5] 杨星月,赵宏,刘佳,等.针刺在国内外腰痛指南中的应用现状[J].中国针灸,2019,39(8):908-912.
[6] Duan X,Coburn M,Rossaint R,et al. Efficacy of perioperative dexmedetomidine on postoperative delirium:systematic review and meta-analysis with trial sequential analysis of randomised controlled trials [J]. Br J Anaesth,2018, 121(2):384-397.
[7] Kim JA,Ahn HJ,Yang M,et al. Intraoperative use of dexmedetomidine for the prevention of emergence agitation and postoperative delirium in thoracic surgery:A randomized-controlled trial [J]. Can J Anaesth,2019,66(4):371-379.
[8] Sepulveda E,Franco JG,Trzepacz PT,et al. Delirium diagnosis defined by cluster analysis of symptoms versus diagnosis by DSM and ICD criteria:diagnostic accuracy study [J]. BMC Psychiatry,2016,16:167.
[9] Yang Y,Zhao X,Dong T,et al. Risk factors for postoperative delirium following hip fracture repair in elderly patients:asystematic review and meta analysis [J]. Aging Clin Exp Res,2017,29(2):115-126.
[10] Neerland BE,Hsll RJ,Seljeflot I,et al. Associations between delirium and preoperative cerebrospinal fluid creactive protein,interleukin-6,and interleukin-6 receptor in individuals with acute hip fracture [J]. J Am Geriatr Soc,2016,64(7):1456-1463.
[11] Chen LP,Wang FW,Zuo F,et al. Clinical research on comprehensive treatment of senile vascular dementia [J]. J Tradit Chin Med,2011,31(3):178-181.
[12] Liu F,Li ZM,Jiang YJ,et al. A meta-analysis of acupuncture use in the treatment of cognitive impairment after stroke [J]. J Altern Complement Med,2014,20(7):535-544.
[13] 陆斌,王麒,丁玲玲.经皮穴位电刺激对腹腔镜胆囊切除术患者术后早期恢复质量的影响[J].中国医药导报,2019,16(13):112-115,119.
[14] 李莉,呂艳,翟翔隽,等.右美托咪定对穴位电刺激产妇分娩镇痛效果的影响[J].中外医学研究,2018,16(4):1-3.
[15] 区燕云,李冬芬,何煜才,等.经皮穴位电刺激配合康复锻炼干预方案对危重症多发性神经病患者下肢运动功能的改善效果[J].中国医药科学,2019,9(1):180-182,186.
[16] 吴晓珲,陈文婷.经皮穴位电刺激辅助全麻对老年心脏手术患者术后免疫功能和认知功能的影响[J].中国医药导报,2019,16(9):145-148,157.
[17] Feng X,Yang S,Liu J,et al. Electroacupuncture ameliorates cognitive impairment through inhibition of NF-κB-mediated neuronal cell apoptosis in cerebral ischemia-reperfusion injured rats [J]. Molecular Medicine Reports,2013,7(5):1516-1522.
[18] Su X,Meng ZT,Wu XH,et al. Dexmedetomidine for prevention of delirium in elderly patients after non-cardiac surgery:A randomised,double-blind,placebo-controlled trial [J]. Lancet,2016,388(10 054):1893-1902.
[19] 丁玲玲,张宏,米卫东,等.右美托咪啶对老年患者在机器人辅助腹腔镜手术麻醉苏醒期及术后认知功能的影响[J].中南大学学报:医学版,2015,40(2):129-135.
[20] 李莉,吕艳,翟翔隽,等.右美托咪定对穴位电刺激产妇分娩镇痛效果的影响[J].中外医学研究,2018,16(4):1-3.
[21] 刘军,董友靖.右美托咪定对心肌缺血-再灌注损伤大鼠的心肌保护作用及机制[J].临床和实验医学杂志,2018, 17(23):2476-2479.
[22] Deiner S,Luo X,Lin HM,et al. Intraoperative infusion of dexmedetomidine for prevention of postoperative delirium and cognitive dysfunction in elderly patients undergoing major elective noncardiac surgery:A randomized clinical trial [J]. JAMA Surg,2017,152(8):e 171 505.
[23] Leung JM,Leung CW,Leung CM,et al. Clinical utility and validation of two instruments(the Confusion Assessment Method Algorithm and the Chinese version of Nursing Delirium Screening Scale)to detect delirium in geriatric inpatients [J]. Gen Hosp Psychiatry,2008,30(2):171-176.
[24] 魏风,陈俭.神经元特异性烯醇化酶在颅脑损伤中的研究进展[J].医学综述,2012,18(1):13-15.
[25] Kessler FH,Woody G,Portela LV,et al. Brain injury markers(S100B and NSE)in chronic cocaine dependents [J]. Braz J Psychiatry,2007,29(2):134-139.
(收稿日期:2019-11-05 本文编辑:刘明玉)
猜你喜欢
中外医疗(2017年2期)2017-03-20
中国现代医生(2016年30期)2017-03-02
中国医学创新(2017年2期)2017-02-23
医学信息(2016年35期)2017-02-23
中国医药科学(2016年1期)2016-03-12
现代仪器与医疗(2015年3期)2015-07-06
中国现代医生(2015年4期)2015-03-11
心脑血管病防治(2014年2期)2014-07-18
