
Evaluation of ischemic lesions after carotid artery stenting with diffusion-weighted imaging
2020-09-14 10:51MuratBeyhanBeratAcuErkanMehmetMuratrat
World Journal of Clinical Cases 2020年10期
Murat Beyhan,Berat Acu,Erkan Gökçe,Mehmet Murat Fırat
Murat Beyhan,Erkan Gökçe,Department of Radiology,Tokat Gaziosmanpasa University Faculty of Medicine,Tokat 60100,Turkey
Berat Acu,Department of Radiology,Eskisehir Osmangazi University Faculty of Medicine,Eskisehir 26480,Turkey
Mehmet Murat Fırat, Department of Radiology,Guven Hospital,Ankara 06540,Turkey
Abstract
Key words:Carotid artery stenosis;Carotid artery stenting;Diffusion-weighted imaging;Ischemia;Stroke
INTRODUCTION
Atherosclerosis of the carotid artery is a major cause of ischemic cerebrovascular disease[1].Stenosis in the proximal carotid artery secondary to atherosclerosis is among the leading causes of transient ischemic strokes and cerebral infarction.Carotid endarterectomy(CE)or carotid artery stenting(CAS)are the methods proposed to prevent ischemic strokes[2].CE is still the best treatment modality for symptomatic patients and patients with carotid stenosis of over 70%(North American Symptomatic Carotid Endarterectomy Trial,NASCET)[3].On the other hand,CAS should be used in patients with contralateral occlusion that poses high risk in surgery,patients with anatomical variations that cause technical difficulties in surgical accessing[such as high-placement internal carotid artery(ICA)bulb,history of prior neck dissection and presence of tracheostomy and radiation injury] or patients with serious comorbidities[4].Current medical guidelines suggest the use of embolic protection devices(EPDs)during CAS to prevent periprocedural ischemic events[5].
In diffusion-weighted imaging(DWI),Brownian movement of water in tissues and random movement of water molecules due to their kinetic(thermal)energies are visualized[6].Higher signal intensity in DWI shows lower water diffusion,which in turn is an early and sensitive indication of brain ischemia that develops as a result of irreversible cellular damage[7].Therefore,DWI has been proposed as a highly sensitive and robust method for the identification of new ischemic events during CAS[8].One advantage of using DWI during the interventions is the ability to provide pre- and post-treatment measurements of the lesion for comparison[9].Most ischemic lesions do not manifest themselves in clinical neurological events and are potentially reversible,as indicated by follow-up examinations using magnetic resonance imaging(MRI)[10].In the present study,number,volume and cerebral parenchymal and vascular distributions of newly detected ischemic lesions in cases with carotid artery stenosis revealed by DWI after CAS were evaluated retrospectively.
MATERIALS AND METHODS
Patients
The study included 64 cases that underwent CAS procedures between October 2006 and July 2012 in the Interventional Radiology Unit of the Radiology Department at Tokat Gaziosmanpasa University,Faculty of Medicine.Forty-seven of the cases(73.4%)were male,and seventeen(26.6%)were female.The average age was 67.96 ±8.03 years(range:42-84).Twelve of the cases(18.8%)had asymptomatic and fifty-two(81.2%)had symptomatic carotid stenosis.Demographic data and average stenosis rates of the cases with carotid artery stenosis are given in Table 1.The diagnoses of carotid stenosis in asymptomatic cases were made incidentally during examinations for other reasons.The most common comorbid diseases and risk factors in the cases were a history of hypertension(HT),diabetes mellitus(DM)and cerebrovascular disease.Accompanying comorbid diseases and their frequencies in carotid artery stenosis patients are given in Table 2.
In 5 cases,stenting was performed in different sessions due to bilateral ICA stenosis,and these cases were evaluated as two separate procedures.Upon detection of dissection in the ICA bulb,stenting was performed for one case.
The atherosclerotic plaques in the carotid arteries less than 1 cm were defined as short segments,while those greater than 1 cm were classified as long segments.The surface properties of plaques causing stenosis were also considered using digital subtraction angiography(DSA).These plaques were classified as regular surfaced,irregular surfaced and ulcerated plaques.Ulcerated plaques were defined as extension of contrast media beyond the vascular lumen within the plaque(Figure 1).Data regarding the side and location of carotid artery stenosis and the distribution of atherosclerotic plaque morphology are given in Table 3.
Ethical considerations
The study was approved by the Ethics Committee of the Tokat Gaziosmanpasa University Faculty of Medicine(No:B.30.2.GOU.0.01.00.00/219).
2007年,Orsouw等[27]提出的CRoPS在文库制备时采用了扩增片段长度多态性的技术,利用2种限制性内切酶将玉米自交系基因组DNA断开,之后经过连接接头与再次扩增片段长度多态性处理,为2个自交系依次添加用以区分的标签,把2组样本结合在一起测序.CRoPS可被应用在基因组含多重复序列且DNA多态性较差的物种.现阶段CRoPS已被应用在玉米SNP开发[27-28]和群体遗传学研究领域[29-30].
CAS procedure
CAS procedure was employed because of ICA occlusion in 10 cases and because of serious comorbid diseases and risk factors in other cases.All procedures were performed under the supervision of an anesthesia team.In all cases but one(case No:4),“Angioguard RX”(Cordis Endovascular,Santa Clara,CA,United States)distal protection devices were used.Dissection,vasospasm or unfavorable anatomy,such as the type and length of aortic arches and excessive tortuosity of the carotid arteries,were the factors limiting the use of EPDs.Therefore,EPD was not used in one case(case No:4)who underwent CAS because of stenosis due to dissection in ICA bulb.In all other cases,“Angioguard RX” EPDs were used.Stenting was performed to assure that 1-2 cm normal segments in the proximal and distal segments of the plaque were covered.When the targeted stent opening could not be achieved by the radial force of the stent,balloon angioplasty was performed in appropriate cases with post-dilatation(all cases except for No:4,11 and 89).Surgical procedure in our patients was completed in about 30 min.
Radiologic evaluation
All patients were examined using DSA before CAS.DSA examination was conducted using a GE Innova 3100(Milwaukee,WI,United States)angiography device.Images were obtained using 1000×1000 and 750×750 matrices.Stenosis rate was determined by NASCET on DSA.In the NASCET method,stenosis rate was calculated as a percentage using the diameters of ICA in the maximum stenosis area and in a more distal normal area.Stenosis measurements were performed at the segments with the highest stenosis among the images taken from lateral and anterior-posterior projections in“GE Advantage Windows Workstation 4.3.” All cases had two routine DWI examinations,1 h before and 1 h after the procedure using a 1.5 T MR machine(Signa Excite HD 12.0 M5B software;GE Healthcare,Milwaukee,WI,United States,2005).A neurovascular head-neck coil(General Electric,1.5 T,8 Ch)was used in the imaging.The images were evaluated using DWI and FLAIR sequences(repetition time:8800,echo time:155.8,number of extractions:1.5,slice thickness:5 mm,gap distance:1.5 mm,field of view:24 cm×24 cm,matrix:288×288).Diffusion gradients were activated in all three orthogonal planes usingb=0 andb=1000 s/mm² values(in DWI,repetition time:8000,echo time:81.5,number of extractions:1.0,slice thickness:5 mm,gap distance:1.5 mm,field of view:28 cm×28 cm,matrix:160×160).DWIs obtained before and after CAS were evaluated retrospectively by two radiologists experienced in neuroradiology work in“GE Advantage Windows Workstation 4.2.” Ischemic lesions detected in the DWI taken in the first hour after the operation were considered new lesions.Also,ischemic lesions detected in DWI carried out for symptomatic cases manifesting neurological finding during the followups within 5-24 h were assumed to emerge due to CAS,and they were considered new ischemia.No new lesions were observed in the patients due to CAS after the first 24 h.Ischemic lesions that appeared after the procedure were seen in TRACE images as hyperintense areas,but they were observed as hypointense areas representing diffusion limitations in apparent diffusion coefficient mapping.Using the TRACE images,the lesion volume was calculated as cm3using“Volume Viewer” software and producing reformat images.Although the size of the ischemic areas was determined using the largest diameters taken in three dimensions,it was considered that the affected area could be determined more accurately through measuring the volume rather than the size since the lesions of cortical-subcortical location have irregular shapes.

Table 1 Gender distribution,clinical appearance and average stenosis rate in patients with carotid artery stenosis
Statistical analysis
Descriptive data were given as mean ± standard deviation,while categorical data were expressed asn(%).χ2test was used to compare categorical variables between the study groups.The variables with continuous distribution based on expressing normal or non-normal distribution were analyzed using paired samplesttest,independent two samplesttest or Mann-WhitneyUtest among two groups and one-way analysis of variance test among three groups.Spearman correlation analysis was used to evaluate the relationships between variables.Pvalues below 0.05 were considered statistically significant.Analyses were performed using SPSS software(IBM SPSS Statistics 19,SPSS Inc.,an IBM Co.,Armonk,NY,United States).
RESULTS
In 20(31.2%)of the 64 cases on which CAS was performed,39 new ischemic lesions were observed.When all cases undergoing CAS were evaluated,the mean number of new lesions was 0.62.New ipsilateral lesions(Figures 2 and 3)were found in 17 of 64 cases(26.5%)after CAS,while 3 cases(4.6%)had new contralateral lesions(Figure 4)and one case(1.5%)had bilateral lesions.The average volume of new ischemic lesions calculated by the two radiologists was 1.10 cm³.Lesion numbers,locations and volumes reported by the two observers were not statistically different(P=0.602;paired samplesttest).New ischemic lesions were of occipital and frontal lobe locations and were most common in middle cerebral artery(MCA)and posterior cerebral artery(PCA)territories.Distributions of new ischemic lesions in DWI after CAS by location and vascular distribution areas are given in Table 4.After the CAS procedure,15 cases(23.4%)were found to have new ischemic lesions without any neurological symptoms and were considered silent ischemias.On the other hand,5 cases(7.8%)were found to have symptomatic indications after the procedure.Technical details of CAS procedures,ischemic lesion numbers and complications are listed in Table 5.Three of the symptomatic cases healed without sequelae in their follow-ups while sequelae(minimal muscle loss)was observed in 2 patients.In symptomatic patients,time to symptom development,neurological symptoms and prognosis are given in Table 6.
Thirty-three plaques causing carotid artery stenosis(51.6%)were in the right carotid artery,while 31 of them(48.4%)were in the left.Most of the plaques were observed in the ICA bulb.In terms of plaque morphologies,it was determined that the majority of plaques causing stenosis were long segmented and ulcerated.In addition,the stenosis rate was higher in the symptomatic group(74.69%)than in the asymptomatic group(68.33%).
Regarding gender distribution,14 of the new lesions were in men and six in women.The volumes of the lesions were significantly higher in men than in women(P=0.039;Mann WhitneyUtest).The number of ischemic lesions observed in DWI was significantly associated with plaque sizes over 1 cm and with stenting in the left carotid artery(P=0.042;Mann WhitneyUtest andP=0.032;independent samplesttest,respectively).The average stenosis rate in the carotid artery was 78.87 ± 10.67 in regular-surfaced plaques,81.43 ± 10.27 in irregular-surfaced plaques and 64.07 ± 16.23 in ulcerated plaques.Carotid stenosis rate was significantly lower in cases with ulcerated plaques(P<0.001;one-way analysis of variance).

Table 2 Accompanying comorbid diseases and risk factors for cases with carotid artery stenosis
DISCUSSION
It is recognized that CAS can cause new ischemic lesions detected by DWI in the range of 22%-54%[11].DWI lesions associated with CAS also occur in the cerebral cortex,mostly in watershed areas[12].In our study,the prevalence of post-CAS DWI lesions was 31.2%,which was close to the lower limits in the literature.Instead of watershed areas,new ischemic lesions were observed in cerebral cortex,MCA and PCA territories in more than half the cases in the present study.
Despite the advent of stent technology,thromboembolic events remain obstacles to be overcome in endovascular therapy.Although stenotic carotid lesions have fragile thrombotic and atherosclerotic components that are vulnerable to fragmentation,these particulates are responsible for most of the neurological events that can develop during the stenting process[13].Cerebral embolism may be observed in most diagnostic,invasive and surgical procedures performed in supra-aortic vessels.Most of these embolisms are clinically silent and in only a few cases do clinically persistent strokes develop.For this reason,DWI is used as a marker for clinical strokes after neurovascular interventions.In a study by Hauthet al[14],22 of 105 cases(21%)developed 64 new ischemic lesions in DWI after CAS procedures.Fifty-five of these lesions were reported as ipsilateral,and nine were contralateral.Lövbladet al[9]found new ipsilateral lesions in 4 of 19 patients,and neurological symptoms were observed in 2 of these 4 patients.Broussaliset al[11]performed CAS for 65 out of 110 cases due to symptomatic carotid stenosis.In their studies,new ischemic lesions were detected in 8 cases after CAS,and all lesions were clinically silent ischemia.Jaegeret al[15]reported new ipsilateral lesions in 20 of 70 cases(29%)after CAS,and new contralateral lesions in 6 cases(9%).They found that the mean number of ipsilateral lesions after the intervention was 2.6,and the number of contralateral lesions was 1.2.Forty-seven of the lesions detected after intervention(80%)were in frontal and parietal lobes.Fiftytwo of the 59 newly diagnosed lesions(88%)were found in ACA and MCA territories.In our study,17 of 64 cases after CAS(26.5%)had new ipsilateral lesions,while 3 cases(4.6%)had new contralateral lesions and one(1.5%)had bilateral lesions.The mean number of ipsilateral lesions after the intervention was 1.94,while that of contralateral ones was 1.5.Twenty-nine of them(74.3%)were in occipital,frontal and parietal lobes.Twenty-three of the 39 new lesions(59%)were in MCA and PCA territories.The higher number of new ischemias observed by Jaeger suggests that process-related microembolisms develop more frequently[15].Since ischemic lesions were observed in watershed areas in 28.1% of our cases,hemodynamic factors along with the microembolisms were also established as factors for the development of new ischemias.

Figure 1 Fifty-five-year-old female patient with long segment ulcerated plaque(Patient no.25).A:Appearance on digital subtraction angiography of long segment,irregular surfaced,ulcerated plaque(orange arrow)that caused 70% stenosis that originated from left common carotid artery distal region and extended to internal carotid artery bulb;B:Stenosis and ulcerated plaque disappeared on common carotid artery injection after carotid artery stenting.
Jaegeret al[15]showed that wire or catheter manipulations could lead to new lesions.In the present study,the number of new ischemic lesions was higher in cases where stenting was applied to the left carotid artery.Difficulty in accessing the left common carotid artery,longer access time and an increase in the number and length of manipulations may explain the higher number of ischemic lesions on the left.
Mathuret al[16]showed that longer or multiple stenosis events are independent determinants for stroke.Broussaliset al[11]detected plaque ulceration in the carotid artery in 17 out of 107 cases(15.9%).Similarly,the number of new lesions detected by DWI in our study was significantly higher in long plaque segments(> 1 cm).In addition,plaque ulceration was observed in 27 cases(42.2%),and the carotid stenosis rate was lower in these cases.In the group with asymptomatic carotid stenosis,the rate of stenosis was lower,and ulceration was evident in two-thirds of the cases.
It is recognized that the tendency for atherosclerosis is high in men,while in women the tendency increases after menopause and reaches levels close to men in advanced age[17].Since men constituted three quarters of the cases in the present study,such a finding lends support to the idea that atherosclerosis risk is higher in men.
Using DWI,Tahaet al[18]determined 117 new ischemic lesions in 42 of 95 patients after CAS and found that 3 patients had strokes(two minor and one major ischemia)on the ipsilateral side.Clinically silent ischemias were observed in the remaining patients.The formation of new embolic lesions was lower in proximal flow reverse protection compared to double balloon protection(33%vs48.4%,respectively).However,the respective volumes of the new ipsilateral ischemic lesions were 0.13 cm³and 0.08 cm³.Ruffinoet al[19]found 15 new ipsilateral ischemic lesions in seven of 23 patients after CAS(30.4%)with an average lesion volume of 0.076 cm³.In the present study,however,the average lesion volumes measured by the two observers were 1.10 cm3.The average lesion volumes determined by the two observers were not significantly different.
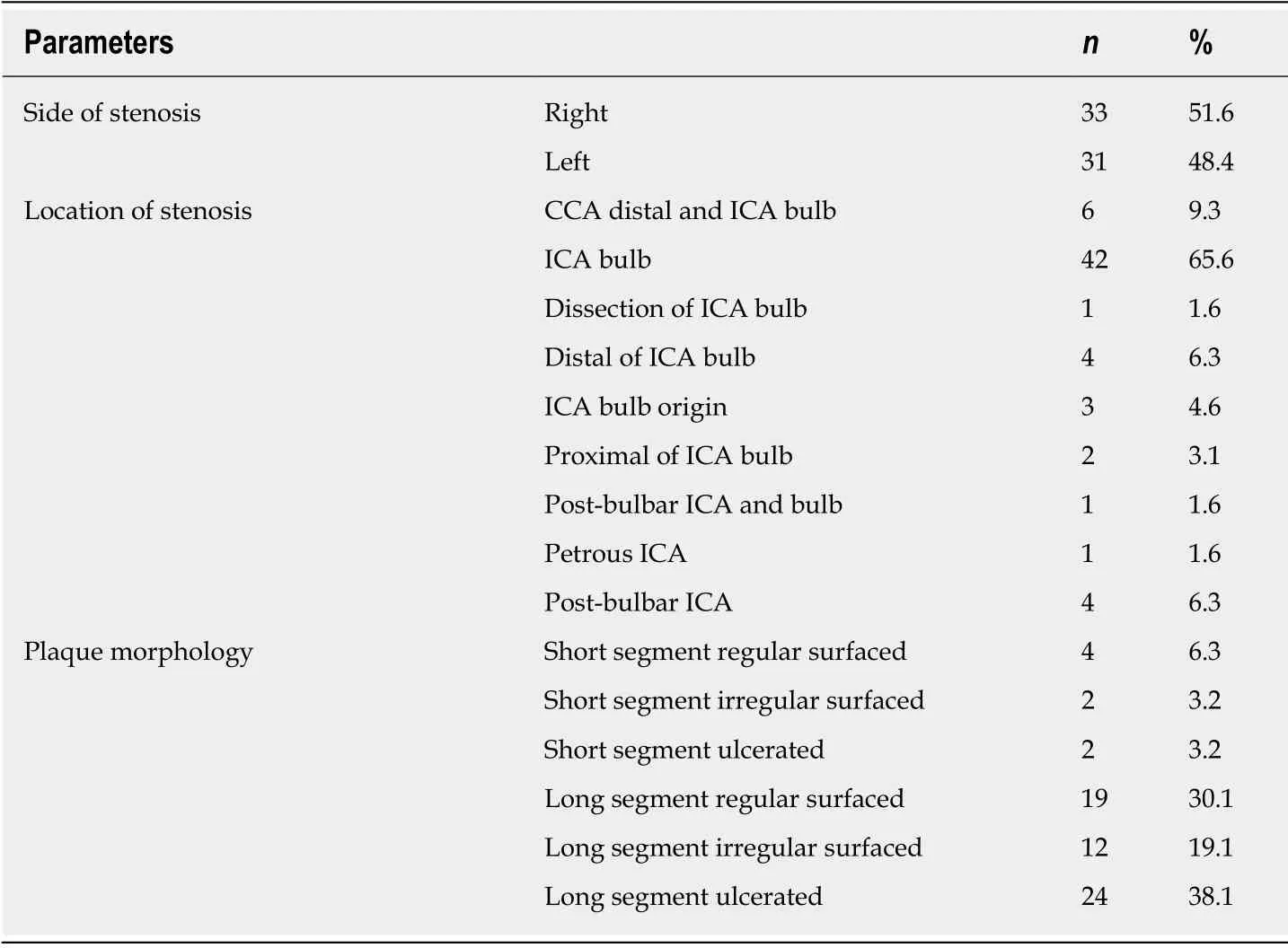
Table 3 Side and location of carotid artery stenosis and distribution of atherosclerotic plaque morphology
Yanet al[20]reported that the most common risk factors for the development of ischemia were HT followed by smoking and coronary artery disease.Fukumitsuet al[21],on the other hand,found that the most common risk factors for ischemia development,in decreasing order,were HT,hyperlipidemia and DM.In accordance with the literature,HT was the most common risk factor in the present study for ischemia development followed by DM and cerebrovascular disease history.
The present study has some limitations.First,the failure of the DWI series taken before and after CAS to pass through the same planes might have caused errors in the number,localization and dimensions of the lesions.Second,the patient population was relatively small.Third,although the size was taken as the ischemic area with the largest diameter in three planes,volume measurement was performed rather than size measurement since the lesion shape was irregular especially in corticallysubcortically located lesions.Fourth,the study was retrospective.
In conclusion,new ischemic lesions may appear in the main arterial territories due to CAS.They may also occur in watershed areas.Difficulty in accessing the left common carotid artery,the increased number of manipulations and the long intervention time could explain the high number of ischemic lesions on the left.In addition,more ischemic lesions could be seen in long segment plaques.

Table 4 Location and distribution by vascular territories of ischemic lesions which developed after carotid artery stenting based on diffusion-weighted imaging

Table 5 Technical properties,ischemic lesion numbers and complications in carotid artery stenting procedures

Table 6 Time to symptom development,neurological symptoms and prognosis in symptomatic patients after carotid artery stenting

Figure 2 Seventy-six-year-old male patient with new ipsilateral ischemic lesion after left carotid artery stenting(Patient No.29).A-B:Focal acute ischemic lesion in the occipital lobe cortical-subcortical surface that is hyperintense in diffusion-weighted imaging(arrow)but hypointense in apparent diffusion coefficient mapping(arrow);C:Ischemic lesion volume(2.730 cm³)measured by the first observer is illustrated.

Figure 3 Sixty-eight-year-old male patient with two new ipsilateral ischemic lesions after left carotid artery stenting(Patient No.19).A-B:Focal acute ischemic lesion in the left middle frontal gyrus cortical surface that is hyperintense in diffusion-weighted imaging(arrow)but hypointense in apparent diffusion coefficient mapping(arrow);C:Ischemic lesion volume(0.263 cm³)measured by the first observer is illustrated;D-E:Focal ischemic lesion during acute phase in the left superior frontal gyrus lateral cortical surface that is hyperintense in diffusion-weighted imaging(arrow)but hypointense in apparent diffusion coefficient mapping(arrow);F:Ischemic lesion volume(0.577 cm³)measured by the second observer is illustrated.
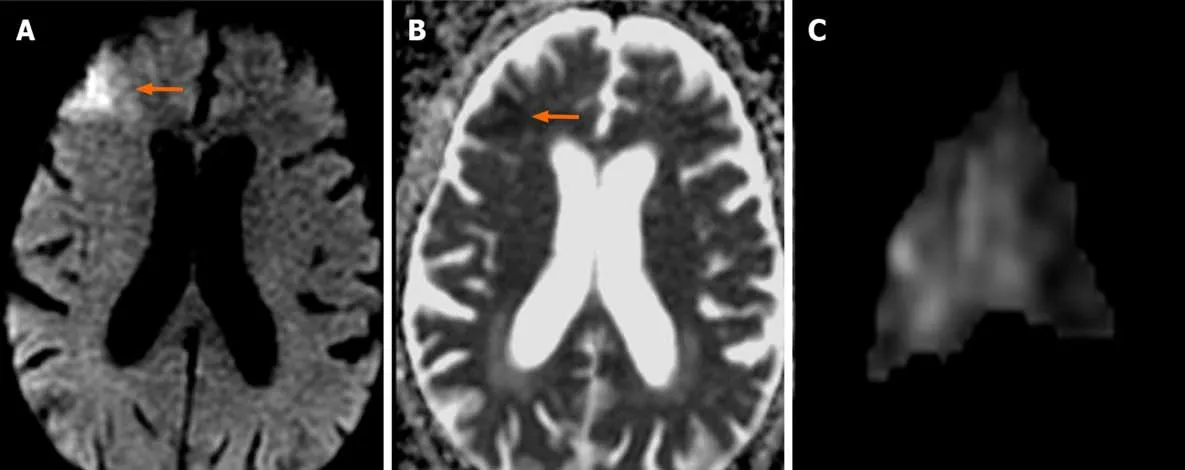
Figure 4 Eighty-four-year-old male patient with new contralateral ischemic lesion after left carotid artery stenting(Patient No.26).A-B:Focal acute ischemic lesion in the right middle frontal gyrus cortical-subcortical surface that is hyperintense in diffusion-weighted imaging(arrow)but hypointense in apparent diffusion coefficient mapping(arrow);C:Ischemic lesion volume(5.506 cm³)measured by the first observer is illustrated.
ARTICLE HIGHLIGHTS
Research background
Carotid artery stenting(CAS)is a relatively less-invasive method in high grade carotid artery stenosis.New symptomatic or asymptomatic cerebral ischemia lesions can develop due to CAS.Diffusion-weighted imaging(DWI)can be used to determine the number and volume of new ischemic lesions.In the present study,cerebral locations,vascular distribution areas and volumes of ischemic lesions that developed due to CAS were evaluated using DWI.
Research motivation
The frequency and size of new ischemias that can develop due to CAS in cases with carotid artery stenosis can be determined using DWI,and thus precautions can be taken against complications that might arise during the follow-up period.
Research objectives
Cerebral locations,vascular distributions and volumes of new ischemic lesions that developed due to CAS were investigated.In addition,associations between stenosis rate,morphology of the plaque causing the stenosis and new lesion development were studied.
Research methods
The study included 64 cases that underwent CAS procedures at Tokat Gaziosmanpasa University,Faculty of Medicine,Department of Radiology,between October 2006 and July 2012.Demographic data,average stenosis rate,accompanying comorbid diseases and their frequencies and distribution of atherosclerotic plaque morphology of patients who had DSA due to CAS were evaluated.DWI images after CAS were evaluated retrospectively by two experienced neuroradiologists in a comparative manner.The number of new lesions and their volumes were determined.Associations between the number of new lesions and the side of the stenosis and those between gender and plaque morphologies were studied.
Research results
Thirty-nine new lesions were observed in 20 of 64 cases(31.2%)with CAS.The lesions were ipsilateral in 17 cases(26.5%)and contralateral in 3 cases(4.6%).The average volume of the new ischemic lesions was determined as 1.10 cm³ by two observers.The most common locations for the new ischemic lesions were occipital and frontal lobes.In terms of watershed areas,they were common in middle cerebral artery and posterior cerebral artery territories.Silent ischemias were found in 15 cases(23.4%)after CAS procedures,while 5 cases(7.8%)had symptomatic ischemias.
Research conclusions
New CAS-originated ischemic lesions are predominantly observed in main arterial territories,but they may also be seen in watershed areas.The higher number of ischemic lesions located on the left side could be explained by the difficulty of accessing the left common carotid artery,the higher number of attempts and longer intervention time.Despite lower stenosis rates,ischemic lesions can be more frequent in ulcerated plaques.
Research perspectives
The number,size and localizations of new lesions that can develop due to CAS can be determined through DWI.Thus,arising symptoms can be determined and managed effectively.
ACKNOWLEDGEMENTS
We thank Osman Demir for the help with the statistical analyses.
猜你喜欢
湘潮(上半月)(2022年7期)2022-12-06
作物学报(2022年2期)2022-11-06
中国种业(2022年8期)2022-08-19
种子(2021年8期)2021-09-23
猪业科学(2021年3期)2021-05-21
少先队活动(2020年12期)2021-01-14
浙江农业学报(2020年12期)2020-12-29
中华诗词(2019年1期)2019-11-14
福建基础教育研究(2019年10期)2019-05-28
求学·理科版(2017年3期)2017-04-27
 World Journal of Clinical Cases2020年10期
World Journal of Clinical Cases2020年10期
- World Journal of Clinical Cases的其它文章
- French Spine Surgery Society guidelines for management of spinal surgeries during COVID-19 pandemic
- Prophylactic and therapeutic roles of oleanolic acid and its derivatives in several diseases
- Macrophage regulation of graft-vs-host disease
- Antiphospholipid syndrome and its role in pediatric cerebrovascular diseases:A literature review
- Remotely monitored telerehabilitation for cardiac patients:A review of the current situation
- Keystone design perforator island flap in facial defect reconstruction