
Treating severe periodontitis with staged load applied implant restoration:A case report
2020-09-14 10:51ShuHuaWangWangChengNiRenFeiWang
World Journal of Clinical Cases 2020年10期
Shu-Hua Wang,Wang-Cheng Ni,Ren-Fei Wang
Shu-Hua Wang,Wang-Cheng Ni,Ren-Fei Wang,School of Stomatology,Zhejiang Chinese Medical University,Hangzhou 310053,Zhejiang Province,China
Ren-Fei Wang,Hangzhou Dental Hospital,Hangzhou 310002,Zhejiang Province,China
Abstract
Key words:Severe periodontitis;Complete implant denture;Lack of bone mass;Temporary implants;Case report;Staging load
INTRODUCTION
Oral implantation in patients with severe periodontitis is a controversial topic[1,2].Though some cases[1-3]reported various treating methods(Table 1 and Table 2),one study[4]tried to skillfully use temporary implants in patients.There are two treatment methods available for patients with serious bone defects that require immediate dental implant surgery[5,6].The indication to conduct All-on-4 implant surgery is relatively wide because longer implants could be used in minimum bone volume.However,the bone plates should be placed high enough because abrasion cannot occur[7].Zygomatic implants can be used in patients if the zygomatic bone is stable enough for immediate restoration to be done[8].Technical requirements are relatively high due to the risk factors of zygomatic implantation surgery.Additionally,All-on-4 and zygomatic implants might impose limitations on long-term oral health maintenance.Therefore,these two treatments might not be suitable for young patients.
By using temporary implants for this case,transitional support was provided throughout the treatment.Studies have shown that temporary implants cause slight bone resorption but have little effect on the increment of bone mineral content.
CASE PRESENTATION
Chief complaints
A 49-year-old female patient was referred to the dental department of Zhejiang Chinese Medical University.
History of present illness
The patient was missing the majority of her teeth and had gingival atrophy and severe alveolar ridge atrophy.There was a long PFM bridge on teeth #11-14 and #21-24(Figure 1).
Imaging examinations
Cone beam computed tomography showed that the alveolar bone was absorbed to 1/3 of the root apex;the bond width of the maxillary anterior region was approximately 3 mm(Figure 2A).The labial bone was absorbed,and the bone height in both posterior areas was approximately 2 mm(Figure 2B).
FINAL DIAGNOSIS
Dentition defect;Severe periodontitis.
TREATMENT
Initial surgery
Surgical procedures overview:(1)Extract teeth #11,#12,#14,#17,#21,#22,#24,and#25;(2)Perform lateral maxillary sinus lifting on both sides;and(3)Perform guided bone regeneration in the maxillary anterior tooth area,insert temporary implants in the anterior tooth area,and perform immediate loading.

Table 1 Comparison of periodontal disease cases
Surgical procedures
Before surgery,the patient received a Cefradine capsule to relieve inflammation,a dexamethasone acetate tablet to relieve swelling,and a compound paracetamol tablet to relieve pain.After conducting regular disinfection and administering anesthesia,teeth #11,#12,#14,#17,#21,#22,#24,and #25 were extracted.After the teeth extraction sockets were cleaned,an incision was made in the middle of the upper alveolar crest,and a relaxant incision was made on the buccal side.A 10 mm×20 mm rectangular window was made at the maxillary sinus lateral wall(Figure 3A).The lowest margin of this window was 3-5 mm from the bottom of the maxillary sinus.The mucosa bottom of the maxillary sinus was turned inward and upward with a collagen membrane layer to make a new mucosa bottom.The bone augmentation material was put into the sinus floor making the lift height approximately 10 mm.
Four Osstem mini implants(Ms System Fixture,Osstem Implant Co.Ltd.,Korea),which were used as a support temporary denture,were implanted into the areas of teeth #12,#14,#22,and #24(Figure 3B).The temporary mini implants were inserted into alveolar bone instead of the bone graft.A 0.5 g autogenous bone mixed with Bio-Oss bone(Bio-Oss,Geistlich Pharma AG,Switzerland)filled the right maxillary anterior bone defect area.Then a 25 mm×25 mm Bio-Gide periosteum(Bio-Gide,Geistlich Pharma AG,Switzerland)covered the top.Teeth #17 and #25 were each made into an auto-tooth bone,which filled the left maxillary anterior bone defect area,and were covered with 25 mm×25 mm Bio-Gide periosteum.The collagen membrane was placed 1.5 mm away from the adjacent tooth in case the membrane was exposed and contaminated.The soft tissue was covered carefully with a relaxant notchviaabsorbed suture(4/0)to hold together the whole membrane.Temporary teeth #14-24 were placed in the maxillary anterior area.The postoperative X-ray showed that the temporary implants were placed properly(Figure 4).

Table 2 The cases comparison of periodontal disease treatments
First subsequent visit(2 wk after the initial surgery):Lateral maxillary sinus lifting on the left side
Before surgery,the patient received a Cefradine capsule to relieve inflammation,a dexamethasone acetate tablet to relieve swelling,and a compound paracetamol tablet to relieve pain.After conducting regular disinfection and administering anesthesia,the periodontal flap procedure was done in the areas of teeth #16 and #17.Then maxillary sinus elevation surgery was conducted with 0.5 g Bio-Oss bone meal that filled the bone defected area.A 25 mm×25 mm bone membrane covered the top,and an absorbed suture was used to close the wound carefully.
Second subsequent visit(5 wk after the initial surgery):Mandibular immediate loading
Examination:Some pigmentation was found on the maxillary CAD/CAM resin crowns.The implants were stable.There was not an uncomfortable feeling when the implants were tapped,and the surrounding gingiva had no abnormalities.Atrophied alveolar bone was found on teeth #32,#34,#36,#37,#42,#43,#44,#45,and #46.These teeth were severely loose.There was not an uncomfortable feeling when tapped,and oral hygiene was acceptable.The open range of the mouth was 3.5 fingers.There wasn't any temporomandibular joint pain,bouncing,or noise.Cone beam computed tomography revealed the bone quality of the mandibular was still acceptable.
Surgical procedures:(1)Cleaned resin crowns and gum and removed pigment with a polishing needle;(2)Before surgery,the patient received a Cefradine capsule to relieve inflammation,a dexamethasone acetate tablet to relieve swelling,and a compound paracetamol tablet to relieve pain.The patient gargled chlorhexidine twice for 3-5 min each time;(3)After conducting regular disinfection and administering anesthesia,the gingiva was reconstructed.Teeth #32,#34,#36,#37,#42,#43,#44,#45,and #46 were extracted.Teeth extraction sockets were cleaned deeply,and granulation tissue was removed.An incision and an access flap were made in the mandibular region.After preparing the implant sockets,teeth #33,#35,#37,#43,#45,and #47 were implanted with SP 14.0 mm×14 mm,4.5 mm×11 mm,5.0 mm×9.5 mm,4.0 mm×14 mm,4.5 mm×12.5 mm,and 5.0 mm×9.5 mm permanent implants(Element Implant Mc Inicell,Thommen Medical AG,Switzerland)(Figure 5A).The torsion force was set at 35 Ncm.Teeth #33,#35,#43,and #45 were placed in multidental abutments,while teeth #37 and #47 were placed in abutments.Bio-Oss bone meal(Bio-Oss,Geistlich Pharma AG,Switzerland,0.5 g)filled the areas of teeth #33,#43,and #45.Collagen plugs were placed in the areas of teeth #44 and #46.An absorbed suture was used to close the wound carefully;(4)After surgery,the abutments were removed and model transfer levers were placed in the areas of teeth#33,#35,#43,and #45.An X-ray showed that the implants were inserted in an acceptable position,and the implants combined with the model transfer levers firmly(Figure 5B).The models were copied and CAD/CAM resin crowns were made;and(5)We tried on CAD/CAM resin crowns,performed immediate loading,and polished and fixed resin crowns.Routine postoperative care and medical advice were provided after surgery.
Third subsequent visit(29 wk after the initial surgery):Removed temporary implants,performed immediate loading on the maxillary and permanent artificial teeth(with plastic base)
Treatment:(1)Before surgery,the patient received a Cefradine capsule to relieve inflammation,a dexamethasone acetate tablet to relieve swelling,and a compound paracetamol tablet to relieve pain.The patient gargled chlorhexidine twice for 3-5 min each time;(2)After removing the maxillary resin crowns,conducting regular disinfection,and administering anesthesia,the implant sockets were prepared,and the mini Osstem implant was removed.Implant surgery was performed in the areas of teeth #11,#13,#15,#16,#21,#23,#24,and #26,and we placed permanent implants(Element Implant Mc Inicell,Thommen Medical AG,Switzerland)with SP 14.0 mm×11 mm,4.0 mm×11 mm,4.5 mm×11 mm,5.0 mm×9.5 mm,4.0 mm×11 mm,4.0 mm×11 mm,5.0 mm×12.5 mm,and 5.0 mm×9.5 mm separately(Figure 6A).The abutments were placed carefully after implantation.The torsion force was set from 25 Ncm to 30 Ncm in the area of tooth #23,whereas in the areas of teeth #11,#13,#15,#16,#21,#24 and #26,the torsion force was 35 Ncm.An absorbed suture(4/0)was used to close the wound carefully;(3)The X-ray post-surgery showed that all implants were placed in an acceptable position as well as had satisfactory primary stability(Figure 6B);(4)The maxillary and mandibular were mocked up,and the resin crowns were worn until the next day;and(5)Routine postoperative care and medical advice were provided after surgery.
Fourth subsequent visit(29 wk after the initial surgery):Performed immediate loading via artificial tooth(with plastic base)
The protective caps were removed,and temporary dentures in the areas of teeth #11,#13,#15,#16,#21,#24,#26,#33,#35,#37,#43,#45 and #47 were tried on.The position was acceptable.We fixed the screw,blended,polished,and sealed the dentures.
Fifth subsequent visit(37 wk after the initial surgery):Mocked up mandibular and temporary CAD/CAM resin crown bridge were made

Figure 2 Image examinations before operation.A:Stomatographic tomography of patient before operation;B:Cone beam computed tomography image of patient before operation.
The temporary dentures were removed to make final models.The permanent abutments with temporary crowns were made,and gingival repair will be conducted in the next stage.Patient wore temporary dentures that were sealed with resin.
Sixth subsequent visit(39 wk after the initial surgery):Wore temporary CAD/CAM resin crown bridge for gingival repair
The temporary dentures,abutments in maxillary,and the healing caps in the areas of teeth #16 and #26 were removed.After placing permanent abutments and trying on the temporary prosthesis,the shape and the crown contour of the temporary prosthesis were restored.The height of the crown was adjusted and changed the placement.The temporary crown from the area of tooth #23 was removed(Figure 7).Then,the flow resin was used to recover the crown length of the anterior mandibular temporary zirconia prosthesis.As a result,occlusion of the maxillary and mandibular restorations was adjusted(Figure 8A),and maxillary temporary crowns were permanently cemented(Figure 8B).
OUTCOME AND FOLLOW-UP
The patient has a normal bite and has not complained about swelling,pain,food impaction,or discomfort.None of the dentures are loose.During the oral inspection and percussion test,both upper and lower jaws did not exhibit loose implants.Fracture phenomenon was not present in the upper crown,and none of the crowns were loose.The patient displayed excellent oral hygiene and is satisfied with her smile(Figure 8C).
DISCUSSION
In this case,the loss of the maxillary alveolar crest reached class V level,which means the patient was supposed to undergo incremental bone therapy before the implant procedure[9].To speed up the rate of healing and maintain oral function as well as appearance,bone treatment therapy was performed throughout the implantation procedures.
The relationship between the maxilla and the mandible is similar to two conical columns,which taper off from the bottom to the top[10].The basal bone is wider than the alveolar process in the mandible,and the bone resorption is in the direction of the vestibular groove after tooth loss[11].As a result,the resorption of the vertical bone contributed to the increased width in the mandibular.Moreover,the proximal,medial and distance of the edentulous mandible also increased because the basal bone is located near the intermediate region.Bone absorption of alveolar processes can seriously affect the relationship in vertical,horizontal,and sagittal directions[12].The edentulous jaw will cause a more severe maxillary and mandibular bone resorption disorder,usually includes a severe mismatch between the maxillary and mandibular bone,similar to class III mismatch in sagittal and horizontal directions[13].

Figure 3 Intraoral photo during initial surgery.A:Buccal rectangular window at maxillary sinus lateral wall;B:Four Osstem mini implants in the maxillary bone.
Fixed bridge prosthesis selection
Vertical bone augmentation has several advantages,one being the ability to achieve the natural perforation of the anterior maxillary short crown through the adherent mucosa[14].Compared to removable dentures,fixed prosthesis is simple in design and fabrication.Additionally,it can be used to complete the superstructure with allceramic prostheses[15].All of these advantages would make surgery more economically beneficial,minimize injuries,and provide a functional retainer that allows patients to sequence bone augmentation therapy.
Implantation of temporary implants
To increase the success rate of implant surgery,a fixed prosthesis supported by simultaneous implants would release the patient's discomfort.Immediate loading of temporary implants not only allows patients to obtain a satisfactory occlusal recovery during immediate implantation but also plays an important role in avoiding mechanical loading in the incremental tissue area.Also,it is forbidden to wear a mucosa-supported removable partial denture after incremental tissue surgery.
CONCLUSION
In conclusion,indications for staged implant loading include:(1)Iinsufficient bone mass for immediate restoration;(2)Multiple disciplines required;(3)Occlusal retention or reconstruction;and(4)Necessity for temporary restoration of teeth.

Figure 4 Postoperative X-ray showing that the temporary implants were placed properly.

Figure 5 The examinations during permanent implant surgery in mandibular bond.A:Permanent implants in the mandibular bone;B:Postoperative X-ray of implants with model transfer levers.
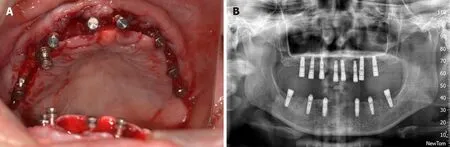
Figure 6 The examination during permanent implant surgery in maxillary bond.A:Permanent implants in the maxillary bone during surgery;B:X-ray showing all permanent implants were placed properly.
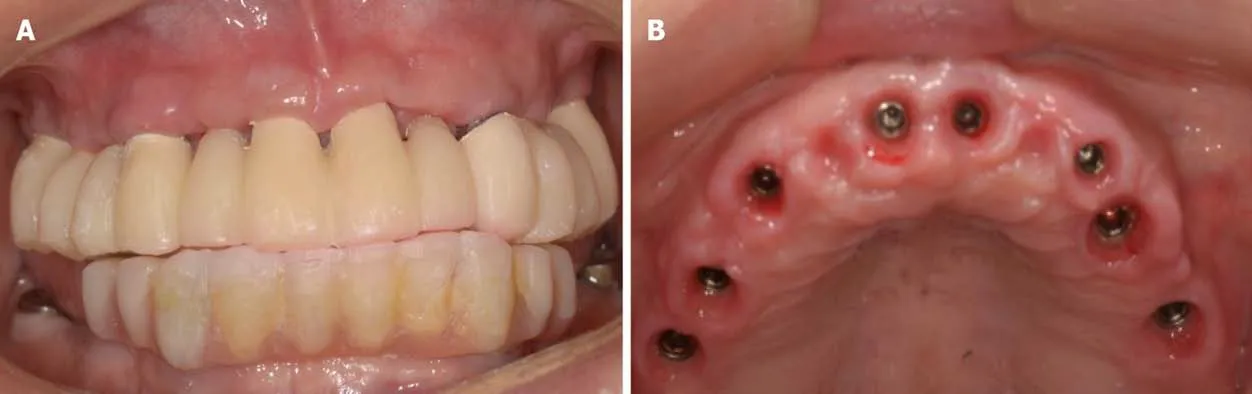
Figure 7 Intraoral photo after full-mouth temporary restoration.A:Temporary CAD/CAM full mouth prosthesis;B:Gingival condition after the temporary restoration was removed.
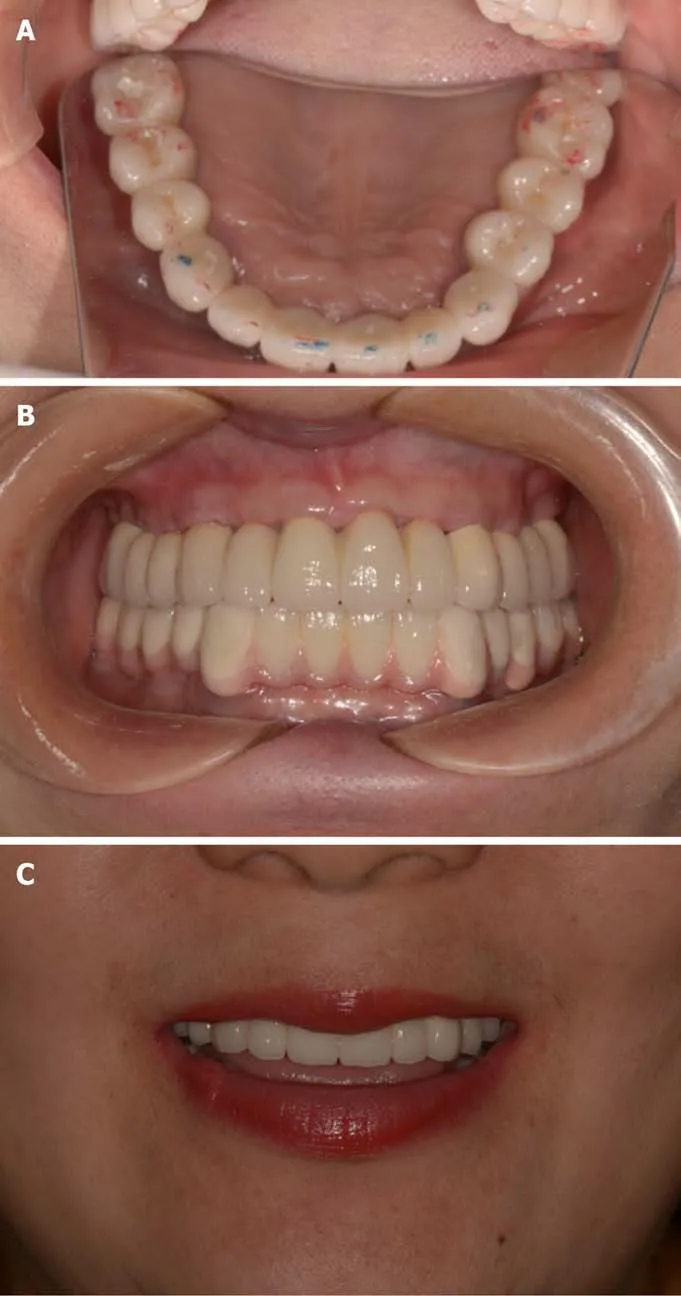
Figure 8 Intraoral photo of permanent outcomes.A:Maxillary and mandibular restorations after the occlusal adjustment;B:Intraoral photo of zirconia prosthesis;C:Patient's outward appearance and smile after the final procedure.
 World Journal of Clinical Cases2020年10期
World Journal of Clinical Cases2020年10期
- World Journal of Clinical Cases的其它文章
- French Spine Surgery Society guidelines for management of spinal surgeries during COVID-19 pandemic
- Prophylactic and therapeutic roles of oleanolic acid and its derivatives in several diseases
- Macrophage regulation of graft-vs-host disease
- Antiphospholipid syndrome and its role in pediatric cerebrovascular diseases:A literature review
- Remotely monitored telerehabilitation for cardiac patients:A review of the current situation
- Keystone design perforator island flap in facial defect reconstruction