
良性阵发性位置性眩晕复位后不同残余症状危险因素分析
2020-10-13 12:23孙相波卞春梅
中国现代医生 2020年24期
孙相波 卞春梅

[摘要] 目的 研究良性阵发性位置性眩晕患者手法复位后不同残余症状的发生率,并对相关危险因素进行分析。方法 随机选取2018年1月~2019年12月在我院就诊并确诊为BPPV的患者172例,收集临床资料,统计残余头晕、走路不稳、颈部不适发生率,并针对不同残余症状采用多元Logistic回归分析进行危险因素分析。 结果 ①172例患者复位成功后出现残余症状者84例,残余症状发生率48.84%(84/172),其中残余头晕发生率57.14%(48/84)、走路不稳发生率60.71%(51/84)、颈部不适发生率29.76%(25/84);②多因素Logistic回归分析显示年龄、复位次数、焦虑状态是BPPV复位后残余头晕的独立危险因素(P<0.05),病程、复位次数、焦虑状态是BPPV复位后残余走路不稳的独立危险因素(P<0.05),病程、复位次数是BPPV复位后残余颈部不适的独立危险因素(P<0.05)。 结论 BPPV复位后存在头晕、走路不稳和颈部不适三个主要残余症状,残余头晕的独立危险因素为年龄、复位次数和焦虑状态,走路不稳的独立危险因素为病程、复位次数和焦虑状态,残余颈部不适的独立危险因素为病程、复位次数,这为早期针对性识别各残余症状提供帮助,有助于临床针对性治疗BPPV复位后残余症状。
[关键词] 危险因素;良性阵发性位置性眩晕;残余症状;手法复位
[中图分类号] R764.3 [文献标识码] B [文章編号] 1673-9701(2020)24-0069-05
[Abstract] Objective To study the incidence of different residual symptoms after manual reduction in patients with benign paroxysmal positional vertigo, and to analyze related risk factors. Methods 172 patients who were diagnosed as BPPV in our hospital from January 2018 to December 2019 were randomly selected and their clinical data were collected. The incidence of residual dizziness, walking instability, neck discomfort was counted. Multiple logistic regression analysis was used for risk factor analysis of different residual symptoms. Results ①In 172 patients after successful manual reduction, 84 patients developed residual symptoms. The incidence of residual symptoms was 48.84%(84/172), of which the incidence of residual dizziness was 57.14%(48/84), the incidence of unstable walking was 60.71%(51/84), and the incidence of neck discomfort was 29.76%(25/84). ②Multivariate logistic regression analysis showed that age, number of reduction and anxiety status were independent risk factors for residual dizziness after BPPV reduction(P<0.05). The course of disease, the number of reduction and the state of anxiety were independent risk factors for residual walking instability after BPPV reduction(P<0.05). The course of disease and the number of reduction were independent risk factors for residual neck discomfort after BPPV reduction(P<0.05). Conclusion There are three main residual symptoms of dizziness, walking instability and neck discomfort after BPPV reduction. The independent risk factors for residual dizziness are age, number of reductionand and anxiety state. The independent risk factors for walking instability are course of disease, number of reduction and anxiety status. The independent risk factors for residual neck discomfort are the course of disease and the number of reductions. This provides early targeted identification of each residual symptom and helps clinically treat residual symptoms after BPPV reduction.
[Key words] Risk factors; Benign paroxysmal positional vertigo; Residual symptoms; Manual reduction
良性阵发性位置性眩晕(Benign paroxysmal positional vertigo,BPPV)是周围性眩晕中最常见的疾病,治疗首选耳石复位,经复位后部分患者虽然眩晕和眼震消失,但仍遗留头晕、走路不稳及颈部不适等残余症状[1-2],症状持续数天到数月不等,严重影响患者身心健康及生活质量。针对残余症状发生的相关危险因素,目前国内外研究[3-5]尚不能完全统一,并且多局限于对残余头晕(Residual dizziness,RD)危险因素进行研究,而忽视了其他残余症状。本研究通过回顾我院172例BPPV患者的临床资料,对残余头晕、走路不稳、颈部不适三大典型残余症状的危险因素进行分析,为临床针对性预防与治疗BPPV不同残余症状提供参考,现报道如下。
1 资料与方法
1.1 一般资料
选取2018年1月~2019年12月在我院就诊并确诊的BPPV患者172例,均经手法复位成功并有完整随访记录。其中男71例,女101例,平均年龄(52.15±13.91)岁,后半规管BPPV受累137例,水平半规管BPPV 32例,其他BPPV类型3例。成功复位后1 d內复查有无残余症状,残余症状主要为头晕、走路不稳、颈部不适[1],所有患者分别以残余头晕、走路不稳、颈部不适进行分组,其中以残余头晕分组:有残余头晕者48例,无残余头晕者124例;以走路不稳分组:有走路不稳者51例,无走路不稳者121例;以颈部不适分组:有颈部不适者25例,无颈部不适147例。
1.2 诊断与排除标准
诊断标准按照中华医学会耳鼻咽喉头颈外科学分会《良性阵发性位置性眩晕诊断与治疗指南(2017)》[6]。排除标准:有严重腰间盘突出症、强直性脊柱炎等肌肉骨骼系统病变,不能行手法复位者;有脑出血、脑梗等严重中枢神经系统疾病者;有颅脑外伤及手术史者;言语交流障碍、重度耳聋、严重视力障碍者;合并梅尼埃病、突发性耳聋、前庭神经炎等疾病者;位置性眩晕持续时间超过31 d者。
1.3 方法
根据位置试验判断BPPV类型,采用相应手法复位方法,后半规管BPPV患者均采用Epley法复位,水平半规管BPPV患者均采用Barbecue法复位,前半规管BPPV采用Yacovino法复位,混合半规管BPPV首先复位诱发眩晕及眼震强烈的半规管,间隔3~5 d再行其他半规管复位。每次复位可视患者耐受情况,重复数次直到无眩晕无眼震出现为止。
Epley法复位:①患者坐于治疗床上,头向患侧转45°;②迅速躺倒头悬于床下30°;③患者头向对侧转90°;④同侧方向再转90°,面朝下与仰卧位呈135°角;⑤起身坐起,头下倾20°。每个位置观察至少半分钟。Barbecue法复位:①患者仰卧位,面朝上;②头迅速向健侧转90°,身体左侧卧位;③头再向健侧转90°,呈面向下俯卧位;④头再向健侧转90°,呈患侧在下的侧卧位;⑤继续向健侧转90°,回到位置1。每个位置观察至少半分钟。Yacovino法复位:①患者仰卧位,头正位垂直悬于床下至少30°;②30 s后头迅速上抬下颏抵至上胸部;③30 s后起身坐起,头下倾20°。治愈标准:患者位置性眩晕消失,位置试验时无眩晕及眼震[6]。
1.4 评价指标
登记患者年龄、性别、诱因、受累半规管、病程(复位前眩晕持续时间)等指标,完成焦虑抑郁量表,并统计复位次数。成功后1 d复查无位置性眩晕,记录有无残余头晕、走路不稳、颈部不适。
焦虑抑郁评估采用医院焦虑抑郁量表(Hospital anxiety and depression scale,HADS),包括焦虑与抑郁评分,各有7个条目,其中第1、3、5、7、9、11、13条目评估焦虑状态,第2、4、6、8、10、12、14条评估抑郁状态,每个条目0到3分。焦虑、抑郁单个评分范围0~21分,单个因素评分以≥8分即存在焦虑或抑郁状态,总得分≥12分即具有显著临床精神症状[7]。
1.5 统计学方法
采用SPSS17.0统计学软件进行分析,计量资料组间比较采用单因素方差分析,计数资料比较采用χ2检验,危险因素分析采用多元Logistic回归分析,P<0.05为差异有统计学意义。
2 结果
2.1 不同残余症状发生率
172例患者复位成功后出现残余症状者84例,残余症状发生率48.84%(84/172),残余症状主要为头晕、走路不稳、颈部不适[1],其中以残余头晕分组:有残余头晕者48例,无残余头晕者124例,残余头晕发生率57.14%(48/84);以颈部不适分组:有走路不稳者51例,无走路不稳者121例,走路不稳发生率60.71%(51/84);以颈部不适分组:有颈部不适者25例,无颈部不适147例,颈部不适发生率29.76%(25/84)。所有患者中合并两种残余症状者占35.71%(30/84),以头晕合并走路不稳最多,合并三种残余症状者占5.95%(5/84)。
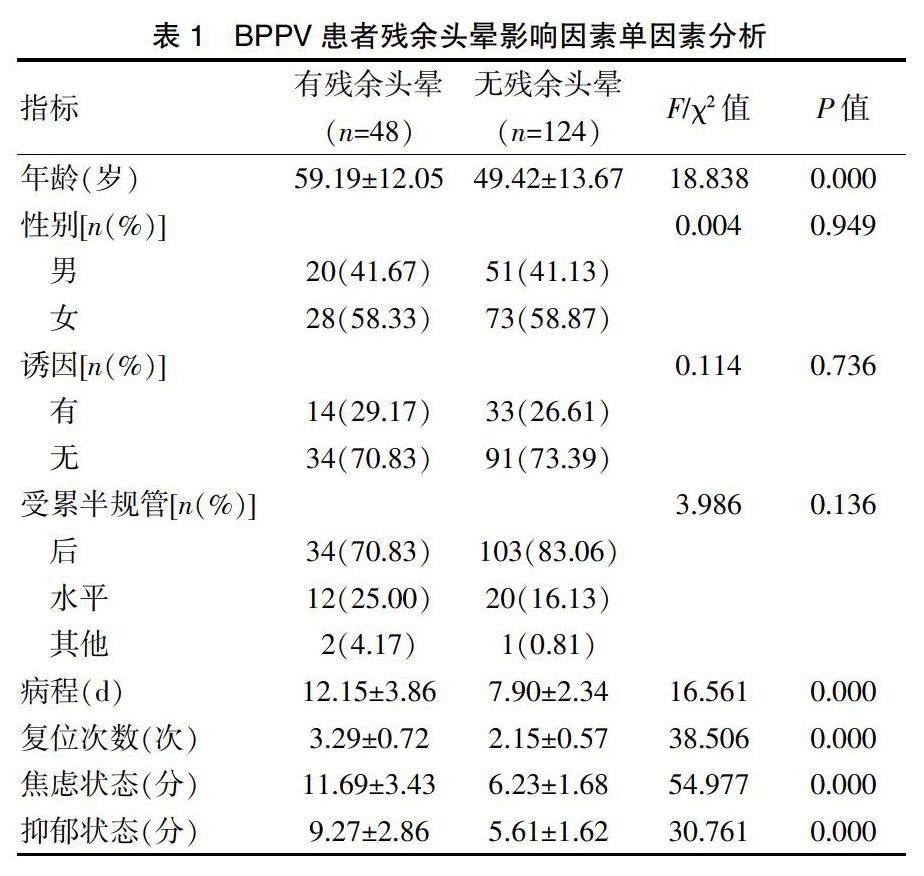
2.2 残余头晕危险因素分析
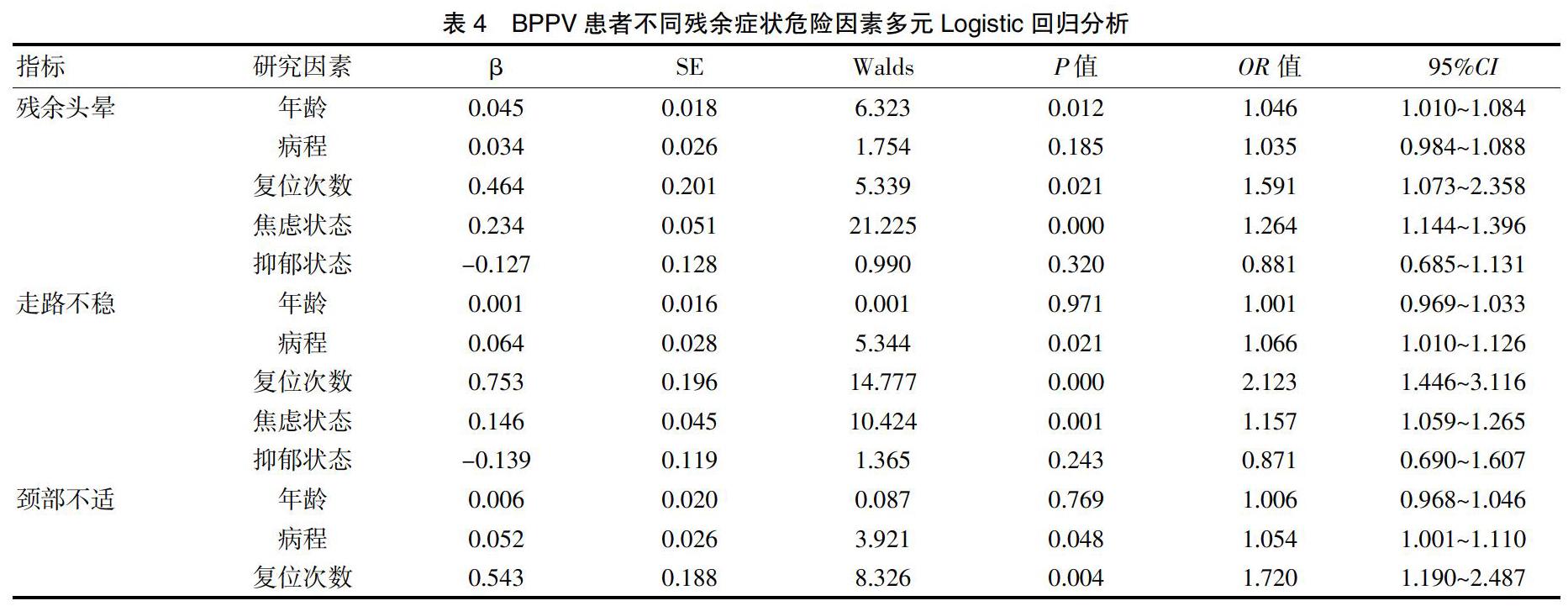
单因素分析显示,有残余头晕组与无残余头晕组年龄、病程、复位次数、焦虑状态、抑郁状态的差异有统计学意义(P<0.05),而性别、诱因、受累半规管的差异无统计学意义(P>0.05)(表1)。对影响因素年龄、病程、复位次数、焦虑状态、抑郁状态进行多因素Logistic回归分析,结果显示年龄、复位次数、焦虑状态是BPPV复位后残余头晕的独立危险因素(P<0.05)。见表4。
2.3 走路不稳危险因素分析
[5] Seo T,Shiraishi K,Kobayashi T,et al. Residual dizziness after successful treatment of idiopathic benign paroxysmal positional vertigo originates from persistent utricular dysfunction[J]. Acta Otolaryngol,2017,137(11):1149-1152.
[6] 良性阵发性位置性眩晕诊断与治疗指南(2017)[J]. 中华耳鼻咽喉头颈外科杂志,2017,52(3):173-177.
[7] Zigmond AS,Snaith RP.The hospital anxiety and depression scale[J]. Acta Psychiatr Scand,1983,67(6):361-370.
[8] 刘晓薇,孙敬武,张波,等. 良性阵发性位置性眩晕成功复位后残余头晕的危险因素分析[J]. 听力学及言语疾病杂志,2018,26(2):148-151.
[9] 张姝,徐凌,高伟,等.良性阵发性位置性眩晕手法复位后残余症状的相关因素分析[J].听力学及言语疾病杂志,2019,27(4):364-369.
[10] Teggi R,Giordano L,Bondi S,et al. Residual dizziness after successful repositioning maneuvers for idiopathic benign paroxysmal positional vertigo in the elderly[J]. Eur Arch Otorhinolaryngol,2011,268(4):507-511.
[11] Micarelli A,Viziano A,Alessandrini M. A comprehensive inaight into the rehabilitative treatment of persistentbenign paroxysmal positional vertigo[J]. J Int Adv Otol,2017,13:147.
[12] D"Silva LJ,Staecker H,Lin J,et al. Retrospective data suggests that the higher prevalence of benign paroxysmal positional vertigo in individuals with type 2 diabetes is mediated by hypertension[J]. J Vestib Res,2016,25(5-6):233-239.
[13] Kim HA,Lee H. Autonomic dysfunction as a possible cause of residual dizziness after successful treatment in benign paroxysmal positional vertigo[J]. Clin Neurophysiol,2014,125(3):608-614.
[14] Pollak L,Segal P,Stryjer R,et al. Beliefs and emotional reactions in patients with benign paroxysmal positional vertigo:A longitudinal study[J]. Am J Otolaryngol,2012, 33(2):221-225.
[15] Giommetti G,Lapenna R,Panichi R,et al. Residual dizziness after successful repositioning maneuver for idiopathic benign paroxysmal positional vertigo:A review[J].Audiol Res,2017,7(1):178.
[16] 孫慧,万秀明,贾庆霞,等. 良性阵发性位置性眩晕患者合并抑郁焦虑研究进展[J]. 中国老年学杂志,2017, 37(10):2594-2596.
[17] 孙利兵,郑智英,王斌全,等. 前庭康复训练对良性阵发性位置性眩晕复位后残余症状的疗效分析[J]. 临床耳鼻咽喉头颈外科杂志,2017,31(12):897-900,905.
[18] Horak FB. Postural compensation for vestibular loss and implications for rehabilitation[J]. Restor Neurol Neurosci,2010,28(1):57-68.
(收稿日期:2020-05-22)
猜你喜欢
中国实用医药(2016年27期)2016-11-30
科技资讯(2016年19期)2016-11-15
中国实用医药(2016年25期)2016-11-03
中国实用医药(2016年24期)2016-10-17
中国实用医药(2016年20期)2016-08-11
