
Prevalence and predictors of nonalcoholic fatty liver disease in South Asian women with polycystic ovary syndrome
2021-01-13 07:43MohamedShengirSrinivasanKrishnamurthyPeterGhaliMarcDeschenesPhilipWongTianyanChenGiadaSebastiani
World Journal of Gastroenterology 2020年44期
Mohamed Shengir, Srinivasan Krishnamurthy, Peter Ghali, Marc Deschenes, Philip Wong, Tianyan Chen,Giada Sebastiani
Abstract BACKGROUND Polycystic ovary disease (PCOS) may be a risk factor for nonalcoholic fatty liver disease (NAFLD) due to common pathogenetic pathways, including insulin resistance and obesity. Both PCOS and NAFLD are more severe in South Asian women. Data on NAFLD in South Asian women with PCOS are lacking.
Key Words: Body mass index; Transient elastography; Controlled attenuation parameter; Hyperadrogenism; Alanine aminotransferase; Lifetime cardiovascular risk
INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD) is the most prevalent chronic liver disease, affecting 25% of the general adult population globally[1,2]. Nonalcoholic steatohepatitis (NASH), the progressive form of NAFLD leading to liver fibrosis and cirrhosis, currently represents the second indication for liver transplantation, with projections to become the leading indication in the next 10 years[3]. Importantly, NASH is already the leading indication for liver transplantation in women, with ethnic differences[4]. This alarming ascent would call for identification of higher risk groups, where screening strategies could be targeted more effectively, as recommended by several guidelines[2,5,6]. NAFLD is often associated with common extra-hepatic conditions, particularly cardiovascular disease which drives most of the mortality[7].
The prevalence of NAFLD may be higher in women with polycystic ovary syndrome (PCOS)[8]. PCOS represents the most frequent endocrinopathy in women of reproductive age. PCOS seems more frequent and severe in South Asian women[9]. Moreover, NAFLD is a major health issue in South Asian women, which is even more frequent if they emigrate to Western countries[10]. Some studies have observed an overlap between NAFLD and PCOS: In both conditions, metabolic comorbidities are relevant pathogenetic drivers[2]. In the context of PCOS, a more complex pathogenesis may account for a relationship between the two diseases, particularly hyperandrogenism[11]. Despite these considerations, the prevalence of NAFLD in PCOS varies largely between 5.5% and 73.3% across studies[12]. This discrepancy may be attributed to retrospective study design leading to selection bias and to varying diagnostic methods and definitions adopted for NAFLD. The majority of studies employed ultrasonography as diagnostic tool for NAFLD, which presents with intrinsic limitations including relatively low accuracy, inter-observer variation and inability of detecting hepatic steatosis involving less than 20%-30% of liver parenchyma[13]. Furthermore, there are limited data on the prevalence of significant liver fibrosis, which mirrors the spectrum of liver disease severity and provides a proxy for NASH prevalence.
创新是引领发展的第一动力。随着我国经济发展进入新常态,急需通过创新创业教育来提升创新水平,激发创新潜能,持续提供创新创业人才供给,以培育新的经济增长点。通过创新创业实践项目、创客空间头脑风暴等形式,积极营造进取向上的创新创业文化氛围,使创新创业和创客理念厚植于大学生的思想之中。同时,社区创客空间和高校创新创业平台将为初始创业者或高阶职业经理人提供知识技能的再培训、再训练,为全社会营造良好的创新创业环境和氛围。
Liver biopsy is still considered the gold standard for the diagnosis of NAFLD and associated liver fibrosis, but it is costly, invasive and with an intrinsic risk of sampling error, making it impracticable as a screening tool[14]. Transient elastography (TE) is an ultrasonography-based non-invasive method using liver stiffness as a surrogate for histologic liver fibrosis[15]. The controlled attenuation parameter (CAP) measures the degree of hepatic attenuation by hepatic fat and is measured simultaneously with liver stiffness measurement (LSM). As such, CAP measurement is a surrogate for hepatic steatosis[16]. In various clinical settings, TE with CAP presents with a good performance compared to liver histology for the detection of hepatic fibrosis and steatosis[16-19]. Thus far, there has been no study employing TE with CAP to screen for NAFLD and associated liver fibrosis in a PCOS population.
We employed TE with CAP in consecutive PCOS patients from South Asia as a part of a routine screening program with the following aims: (1) To assess prevalence and associated predictors of NAFLD; (2) To determine prevalence of significant liver fibrosis. Secondary aims included evaluation of lifetime cardiovascular risk and of other comorbidities associated with NAFLD.
MATERIALS AND METHODS
Study design and population
We performed a cross-sectional cohort study at the Department of Obstetrics and Gynecology of McGill University Health Centre (MUHC), which follows about 1000 active PCOS patients. At MUHC, there is a large population of South Asian women with PCOS. Between October 2018 and July 2019, consecutive South Asian adult patients with PCOS were invited to participate in the study by undergoing a TE examination with CAP as part of a screening program for liver disease. We included patients with PCOS defined by the modified Rotterdam criteria, after excluding other endocrine disorders. All patients met at least two criteria among clinical (hirsutism and/or other signs and symptoms of hyperandrogenism,i.e., acne/seborrhea and alopecia) and/or biochemical hyperandrogenism, ovulatory dysfunction and polycystic ovarian morphology[20]. Exclusion criteria were the following: (1) Positivity for hepatitis C virus antibody or hepatitis B virus (HBV) surface antigen; (2) History of pre-existing liver disease or new diagnosis at the screening visit (auto-immune hepatitis, primary biliary cholangitis, primary sclerosing cholangitis, hemochromatosis, Wilson’s disease, alpha-1 anti-trypsin); (3) History of hepatocellular carcinoma, liver transplantation or decompensated liver disease (ascites, hepatorenal syndrome, spontaneous bacterial peritonitis, hepatic encephalopathy, variceal hemorrhage); (4) Hazardous alcohol intake, as estimated by an Alcohol Use Disorders Identification Test (AUDIT-C) score ≥ 7[21]; (5) Pregnancy at time of recruitment; and (6) Failure of TE examination or unreliable measurement. All patients provided written informed consent for participation into the study. In order to validate the TE examination with CAP measurement in our cohort, we also reported the CAP values from another routine screening program for liver fibrosis running at MUHC. As part of routine assessment at our centre, patients with chronic HBV undergo CAP quantification during TE examination for LSM. We included only female patients aged < 50 years old with chronic HBV, as an appropriate comparator to our PCOS population. We chose this validation group as young patients with chronic HBV have been reported to have low prevalence of NAFLD[22,23]. The Research Ethics Board of the Research Institute of the MUHC approved the study (study code 2019-4584), which was conducted according to the Declaration of Helsinki.
Outcome measures
The primary outcomes of the study were: (1) Prevalence and associated predictors of NAFLD; and (2) Prevalence of significant liver fibrosis. Any grade NAFLD (> 5% of hepatocytes) was defined as CAP ≥ 288 decibels per meter (dB/m)[19], and significant liver fibrosis (stage ≥ F2 out of 4) as TE measurement ≥ 8.0 kilopascals[24-26]. We also explored the use of the recently proposed cut-off of 302 dB/m to diagnose any grade NAFLD[18].
Secondary outcomes were evaluation of the lifetime cardiovascular risk through the atherosclerotic cardiovascular risk equation, according to American College of Cardiology/American Heart Association guidelines[27]and extra-hepatic diseases linked to NAFLD. Sleep apnea and hypothyroidism were diagnosed on the basis of clinical history. Chronic kidney disease (CKD) was defined as estimated glomerular filtration rate < 60 mL/min/1.73 m2, calculated using the CKD-Epi formula, as per KDIGO guidelines[28,29].
TE examination
TE examination was performed on a 4-h fasting patient by two experienced operators. The standard M probe was first used in all patients. The XL probe was used in case of failure with M probe. Examinations were considered valid if the operator was able to obtain at least 10 validated measures and the interquartile range of those measures was < 30% of the median[17,30]. Given recent data on the lack of effect of probe type and steatosis on LSM, we did not use adjusted cut-off values[18].
Serum biomarkers
The simple biomarker hepatic steatosis index (HSI) was calculated and the standard cut-off value of 36 was used to diagnose NAFLD[31,32]. The simple fibrosis biomarkers fibrosis-4 (FIB-4), aspartate aminotransferase (AST)-to-Platelets Ratio Index (APRI) and NAFLD fibrosis score were computed, as previously described[33-35].
Clinical and biological parameters
Anthropometric, clinical, and biochemical measurements and data were collected at recruitment. Family history of liver and cardiovascular diseases was also recorded. Regular physical exercise was defined as at least 150 min of moderate aerobic exercise[5]. The diagnosis of diabetes was based on treatment with antidiabetic drugs or the International Diabetes Federation definition[36]. Any alcohol intake was defined as a score ≥ 5 by the AUDIT-C questionnaire. Biological parameters, collected at time of recruitment, included: AST, alanine aminotransferase (ALT), gamma-glutamyl transferase, platelets, bilirubin, albumin, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglycerides, insulin and glycosylated hemoglobin, C-reactive protein. All patients were screened for pre-existing liver disease with the following: HBV and hepatitis C virus serologies, anti-nuclear antibody, anti-mitochondrial antibody, anti-smooth muscle antibody, ferritin, ceruloplasmin, alpha-1-antitrypsin. Elevated ALT was defined as ALT > upper limit of normal (ULN) of 24 IU/L, as previously described for South Asian women[37]. Patients were classified into three groups according to their measured body mass index (BMI) values, and cut-off values from Asian guidelines were used for this categorisation; lean < 23 kg/m2, overweight 23-25 kg/m2, obese > 25 kg/m2. Waist circumference values exceeding 80 cm was used as the cut-off value for central obesity[38]. Insulin was used to compute the homeostasis model for assessment of insulin resistance (HOMA-IR) index (fasting insulin (mIU/L) X fasting glucose (mmol/L)/22.5)[39]. HOMA-IR > 1.9 was considered indicative of insulin resistance. A patient was defined as metabolically abnormal in presence of any among diabetes, hypertension or hyperlipidemia (triglycerides ≥ 1.7 mmol/L and/or high-density lipoprotein < 1.3 mmol/L), while the absence of all three conditions defined a metabolically normal patient. The following hormonal parameters were evaluated for the diagnosis of biochemical hyperandrogenism: Total testosterone, bioavailable testosterone and sex hormone-binding globulin. Free androgen index (FAI) was calculated as the ratio of total testosterone levels in nmol/L to sex hormone-binding globulin levels in nmol/L × 100 (%)[40]. A FAI > 5 was considered indicative of hyperandrogenism.
Statistical analysis
We compared characteristics of study subjects by NAFLD status using Student’st-test for continuous variables and Pearson’sχ² or Fisher's exact test for categorical variables. Multivariate logistic regression modelling was employed to identify factors predictive of NAFLD. Results were reported as adjusted odds ratio (aOR) with 95% confidence interval (CI). Covariates were includeda prioribased on their clinical relevance or on their significance in univariate analysis (P< 0.10). Final models were adjusted for duration of PCOS, BMI, HOMA-IR, FAI > 5 and ALT > 24 IU/L. The corrected Akaike information criteria (AIC) and the Bayesian information criteria (BIC) were calculated and compared among the models to determine which one had the best goodness-of-fit measure. A lower AIC and/or BIC was indicative of a better fit. The performance of BMI, ALT and FAI to predict NAFLD was measured as area under the receiver operating characteristic curve (AUC). Standard errors of AUC were calculated by DeLong method. A concordance analysis between CAP and HSI was carried out using the kappa score, with results interpreted as follows: Less than 0, less than chance agreement; 0.01–0.20, slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement and 0.81–0.99, almost perfect agreement[41]. Pairwise correlation was employed to test the association of serum fibrosis biomarkers (FIB-4, APRI and NAFLD fibrosis score) with LSM. All tests were two-tailed and with a significance level of α = 0.05. Statistical analyses were performed using STATA 13.1 (STATA Corp. LP, College Station, TX, United States).
RESULTS
After applying exclusion criteria (Figure 1), 101 patients were included into the present study. The XL probe was employed in 19 (18.8%) cases, while the standard M probe was used in all other patients. The failure rate of TE examination (1%) was similar to previous studies[17]. The characteristics of the study population are reported in Table 1. Only 2 out of 101 included patients reported any alcohol intake. Twelve (11.9%) patients were overweight (BMI: 23–25 kg/m2), and 72 (71.3%) were obese (BMI > 25 kg/m2). Central obesity was present in 97 (96%) cases. Elevated ALT was observed in 23 (22.8%) patients.
Prevalence of NAFLD and significant liver fibrosis
The mean CAP value in the study population was 266.9 dB/m (standard deviation 63.0). In our validation group of 125 female patients with chronic HBV aged < 50 years, we found a much lower mean CAP value of 214 dB/m (standard deviation 55.5). Prevalence of NAFLD was 39.6% in the study population of PCOS women, compared to only 8% in the validation group of female patients with chronic HBV. By employing the cut-off of 302 dB/m, the prevalence of NAFLD in PCOS women was 29.7%. Table 1 depicts the characteristics of patients with and without NAFLD, with relative univariate analysis. All patients with NAFLD were metabolically abnormal (Figure 2). By HSI, prevalence of NAFLD was 39.6%. The number of observed agreements between HSI and CAP was 66 (65.3%) for the 288 dB/m and 60 (59.4%) for the 302 dB/m cut-off, respectively. The kappa-value was 0.34 (standard error: 0.08; 95%CI: 0.17-0.50) and 0.25 (standard error: 0.08; 95%CI: 0.10–0.40), compatible with a “fair” strength of agreement. Prevalence of significant liver fibrosis in the cohort was 6.9%. In patients with NAFLD, the prevalence of significant liver fibrosis was 15%, compared to only 1.6% among those without NAFLD. Table 2 depicts the main characteristics of patients with significant liver fibrosis. The prevalence of NAFLD and significant liver fibrosis was higher in obese patients compared to those overweight or lean (Figure 3A). As showed in Figure 3B, the prevalence of NAFLD was significantly higher in patients with hyperandrogenism (P= 0.007), insulin resistance (P< 0.001) and elevated ALT (P= 0.001). Given the known association between false positive results of LSM and elevated ALT, we conducted a sensitivity analysis by excluding patients with elevated ALT[42]. First, no patient had ALT > 10 times the ULN. Second, among the 9 patients with ALT > 2 times the ULN, 3 had significant liver fibrosis. If we would exclude these patients from the analysis, the prevalence of significant liver fibrosis would be 4.3%. Among the serum fibrosis biomarkers, APRI was the only one showing a significant correlation with LSM (Figure 4).
Predictors of NAFLD by multivariate analysis
Table 3 illustrates the multivariate analyses for predictors of NAFLD by CAP cut-offs of 288 and 302 dB/m. After adjustments, independent predictors of NAFLD were higher BMI (aOR: 1.30, 95%CI: 1.13-1.52;P< 0.001), hyperandrogenism (aOR: 5.32, 95%CI: 1.56-18.17;P= 0.008) and elevated ALT (aOR: 3.54, 95%CI: 1.10-11.47;P= 0.035). When the cut-off of 302 dB/m was applied, higher BMI (aOR: 1.33, 95%CI: 1.14-1.55;P< 0.001) and hyperandrogenism (aOR: 3.54, 95%CI: 1.00-12.57;P= 0.049) were independently associated with NAFLD. These models had lower AIC and BIC values than others, hence providing support for their use. The performance of BMI, FAI and ALT to predict NAFLD is reported in Figure 5. There was no difference in performance among the three predictors: AUC was 0.808 (standard error: 0.045; 95%CI: 0.719-0.897) for BMI, 0.761 (standard error: 0.049; 95%CI: 0.665-0.858) for FAI, and 0.722 (standard error: 0.054; 95%CI: 0.615-0.828) for ALT.
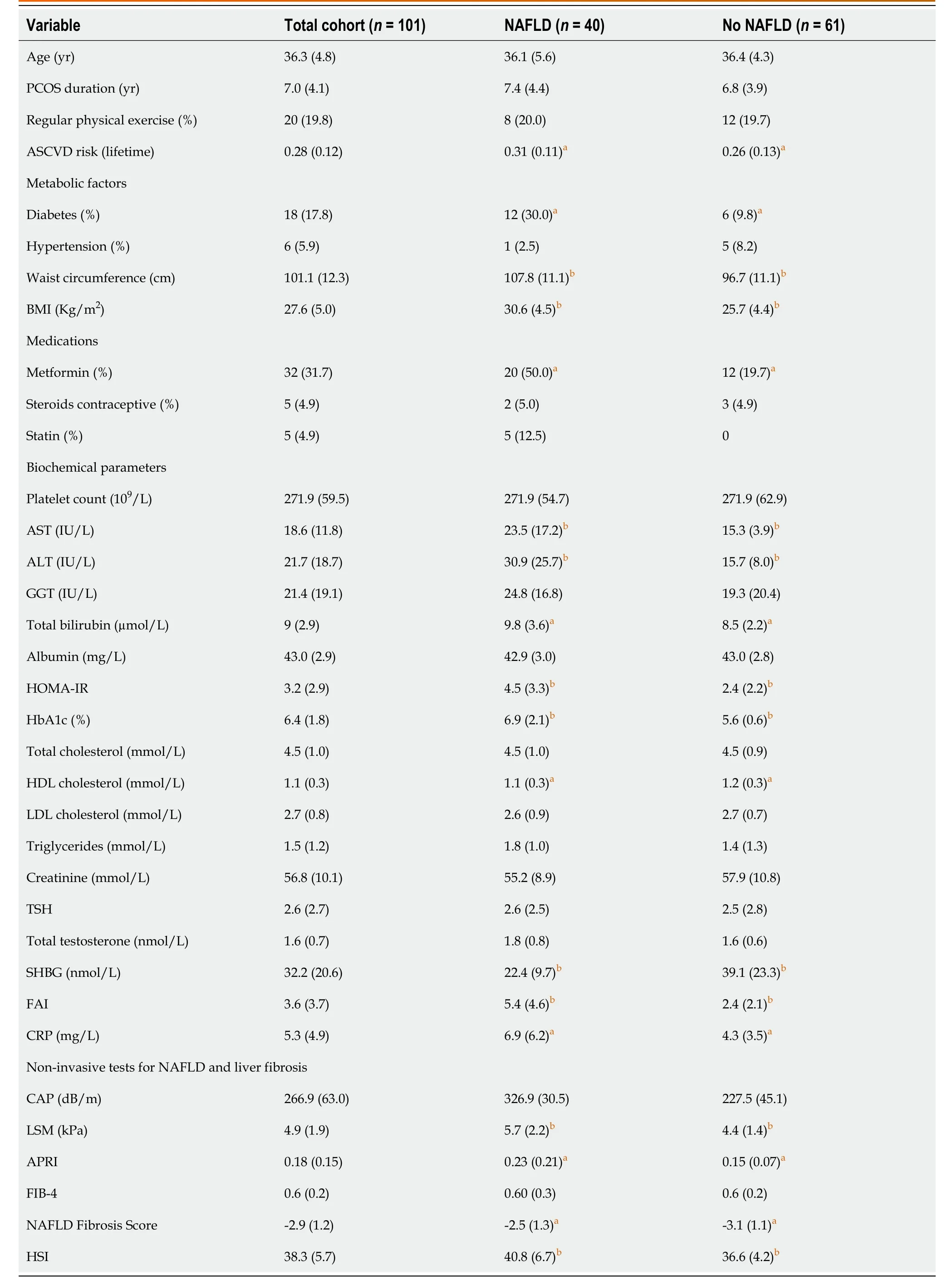
Table 1 Demographic, clinical, biochemical, and pharmacological characteristics of the study population (n = 101) and univariate analyses by outcome status, that is presence of nonalcoholic fatty liver disease
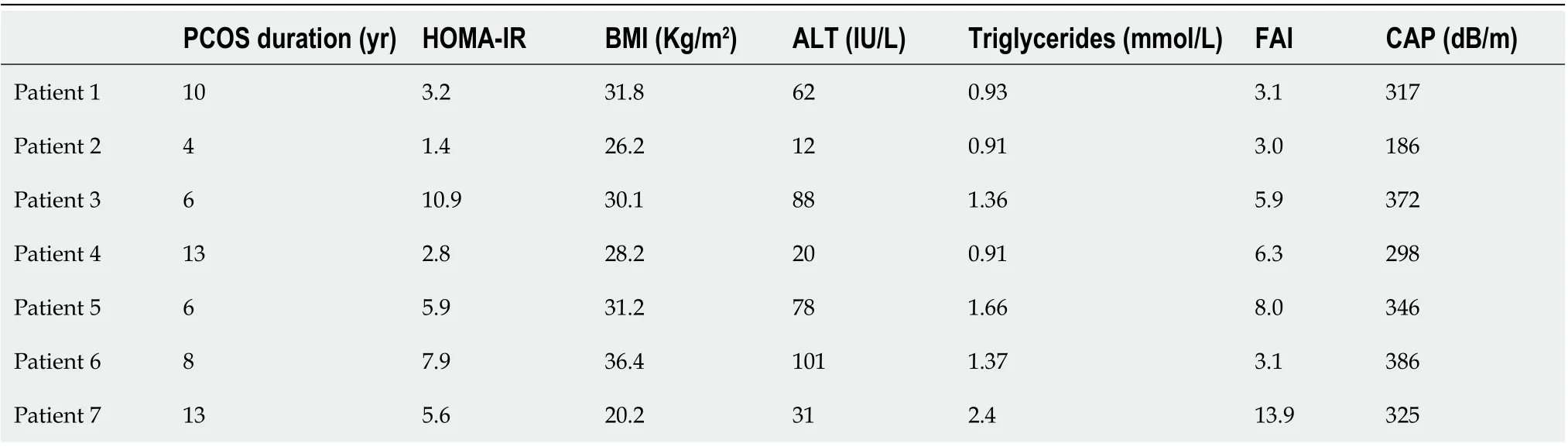
Table 2 Demographic, clinical and biochemical characteristics of patients with significant liver fibrosis (n = 7)

Table 3 Multivariate analysis of factors associated with nonalcoholic fatty liver disease
Cardiovascular risk and other extra-hepatic complications
The atherosclerotic cardiovascular risk was higher in patients with NAFLD (Table 1). Only 12.5% of patients with NAFLD were on statin treatment. There was no difference in the prevalence of hypothyroidism among patients with NAFLD (25.0%) and those without NAFLD (31.1%). There was one case of sleep apnea (1.6%) and one case of CKD (1.6%) among patients with NAFLD.
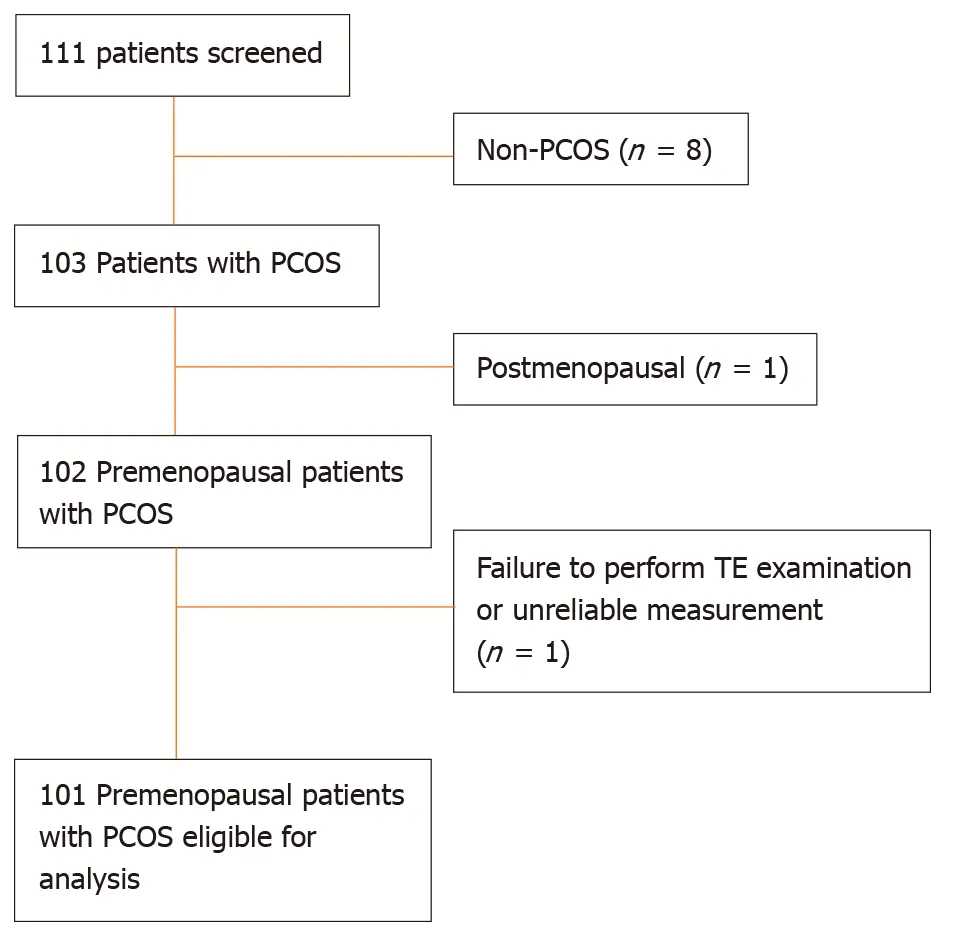
Figure 1 Flow chart displaying the selection of participants in the study cohort. PCOS: Polycystic ovary syndrome; TE: Transient elastography.
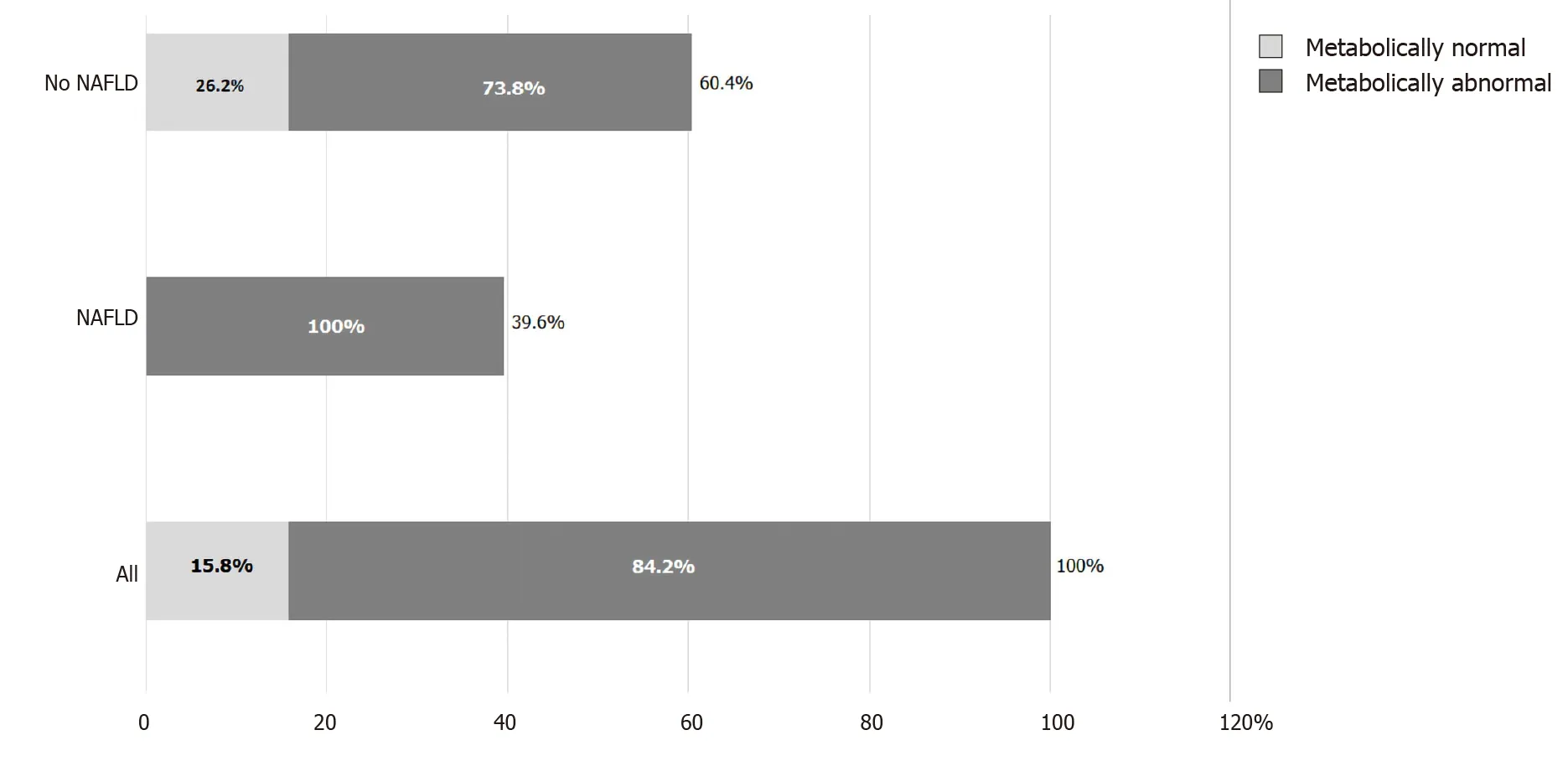
Figure 2 Distribution of metabolically normal and abnormal patients by nonalcoholic fatty liver disease category. NAFLD: Nonalcoholic fatty liver disease.
DISCUSSION
This study, performed in a cohort of consecutive South Asian women with PCOS undergoing a routine screening program for liver disease, showed that NAFLD is a frequent comorbidity. To our knowledge, this is the first study to adopt TE with CAP to investigate NAFLD in PCOS women. TE with CAP is already commonly used in other at-risk populations[43-45]. We also showed that, despite their young age, women with PCOS and NAFLD could have significant liver fibrosis, possibly indicating the coexistence of NASH, the progressive counterpart of NAFLD. Finally, PCOS patients with NAFLD had higher cardiovascular risk score, which should be taken into account for overall risk stratification.
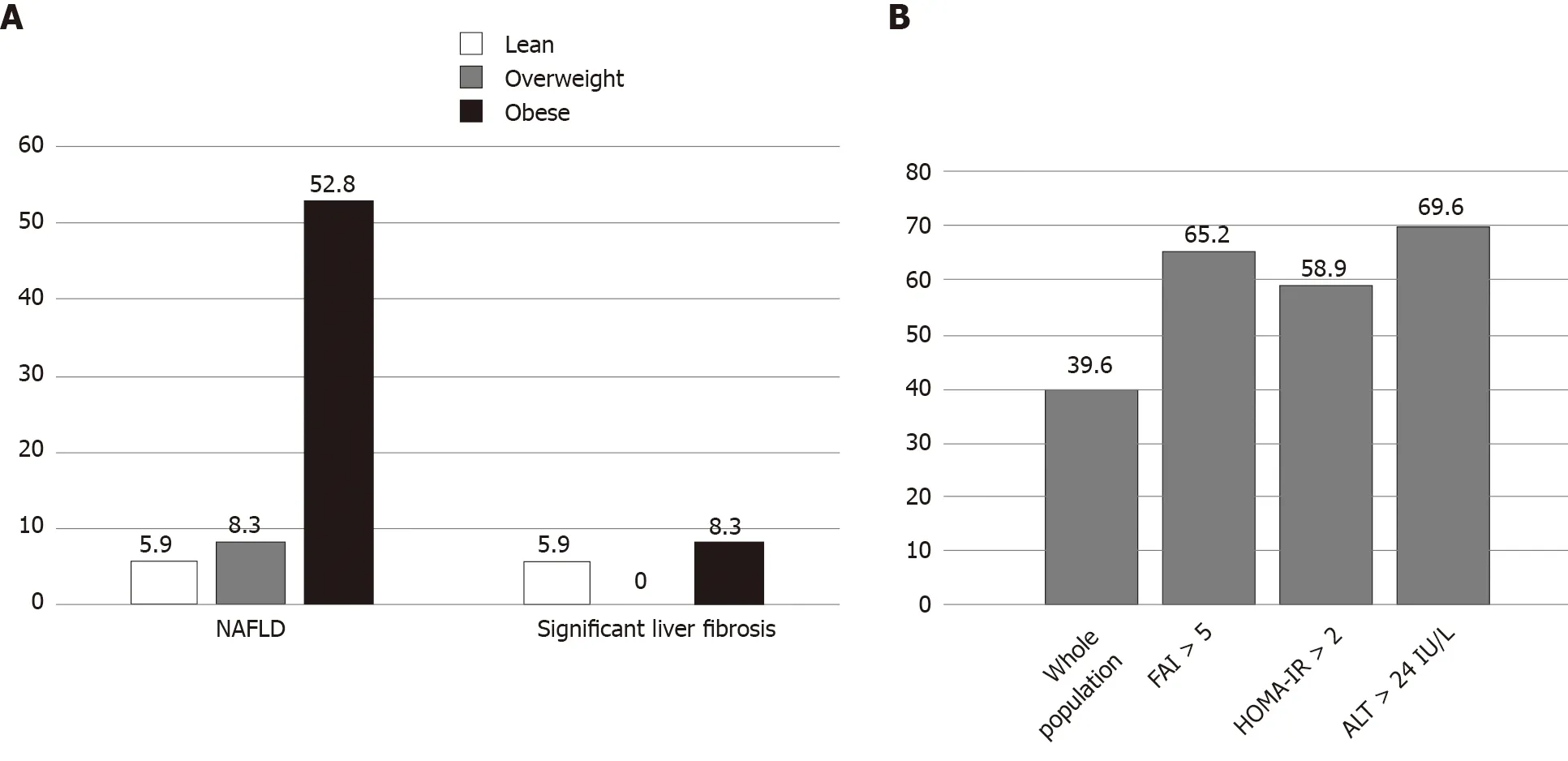
Figure 3 Prevalence of nonalcoholic fatty liver disease and significant liver fibrosis. A: Prevalence of nonalcoholic fatty liver disease (NAFLD), severe NAFLD and significant liver fibrosis according to body mass index category; and B: Prevalence of NAFLD according to patients’ characteristics. NAFLD: Nonalcoholic fatty liver disease; ALT: Alanine aminotransferase; HOMA-IR: Homeostasis model for assessment of insulin resistance.
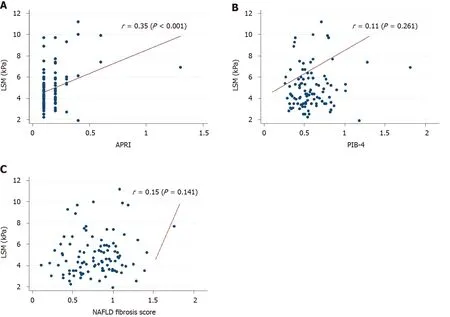
Figure 4 Scatterplot depicting the correlation between liver stiffness measurement. A: Aspartate aminotransferase-to-Platelets Ratio Index; B: Fibrosis-4; and C: Nonalcoholic fatty liver disease fibrosis score. NAFLD: Nonalcoholic fatty liver disease; APRI: aspartate aminotransferase-to-Platelets Ratio Index; FIB-4: Fibrosis-4.
NAFLD affects one quarter of the general population globally[1,2]. NASH is now the second indication for liver transplantation in North America, predicted to become the leading indication within the next 10 years[46]. This will soon impact on the physiognomy of liver transplant waiting lists and on organ supply[47]. As such, there is an urgent need for diagnostic and treatment strategies. The prevalence of NAFLD increases in populations at risk, including those with type 2 diabetes and obesity[2]. NAFLD is often a clinically silent disease until end-stage complications arise. Early identification and risk stratification for those at higher risk for fibrosis progression could help institute interventions to prevent NAFLD progression, and ultimately reduce liver-related morbidity and mortality.
NAFLD is frequent in women with PCOS. Patients with PCOS may be at higher risk for NAFLD due shared pathophysiological features with NAFLD, including insulin resistance, chronic inflammation, dyslipidemia[48]. Moreover, hyperandrogenism likely represents a unique and independent risk factor for NAFLD in this population[11]. Finally, alteration in gut microbiota has been linked to disease severity in both PCOS and NAFLD, thus acting as an additional potential pathogenic bridge between the two conditions[49,50]. In our routine screening program for liver disease, we reported a prevalence of NAFLD at 39.6% and such diagnosis was confirmed in many cases by another non-invasive method, namely the biomarker HSI. This figure is higher than that reported for the general population, where the prevalence of NAFLD is 25%[51,52]. Previous estimates of NAFLD prevalence among PCOS patients ranged widely, between 5.5% and 73.3% across studies[12]. In the present study, we have included a homogeneous population of South Asian women, as both PCOS and NAFLD prevalence vary across ethnicities[53]. South Asian women have been reported to have more severe PCOS symptoms at younger age, with greater insulin resistance than Caucasians[54]. Moreover, NAFLD seems a major health issue in South Asian women, with high rates of advanced liver fibrosis, particularly if they emigrate to Western countries[10]. Previous studies were either of retrospective nature or have employed less accurate diagnostic tools, such as ultrasound or simple serum biomarkers[13,32,55]. In the present study, we employed TE with CAP to investigate the prevalence of both NAFLD and significant liver fibrosis. We have adopted a cut-off value reported as optimal to detect any grade steatosis[19]and we have also applied a recently reported higher cut-off[18]. Significant liver fibrosis affected 6.9% of our cohort, which suggests the co-existence of a progressive disease, namely NASH[2]. Of note, there was a poor correlation between LSM and NAFLD fibrosis score or FIB-4, likely because these two biomarkers incorporate age in their formula, while our study population was young. Conversely, APRI, which does not include age in its formula, had a significant correlation with LSM. Our data suggest that the simple fibrosis biomarker APRI may be preferable to FIB-4 and NAFLD fibrosis score in young PCOS patients.
We found that BMI, hyperandrogenism and ALT were independent predictors of NAFLD. Among them, BMI had the highest AUC to predict NAFLD. This finding underlines the relevance of obesity and associated metabolic conditions. Indeed, in our study population all patients with NAFLD were metabolically abnormal. South Asians have a higher proportion of visceral fat distribution and are more likely to have dyslipidemia than Western patients[56]. However, South Asian patients with NAFLD have an overall lower BMI compared to Caucasians[57]. Other factors contributing to NAFLD in this ethnic group may include genetic variants of the patatin-like phospholipase domain-containing 3 protein, physical inactivity, reduced disease awareness, late diagnosis, as well as sociocultural factors in comparison with Western patient populations[56]. Indeed, in our cohort of young women, only 19.8% were practicing regular physical exercise. Hyperandrogenism measured by FAI was also an independent predictor of NAFLD. Our finding confirms previous data that high FAI correlates with liver disease markers and is a PCOS-specific feature that further increases the risk of NAFLD[12]. Elevated ALT was also an independent predictor of NAFLD on multivariate analysis. Although only 22.8% of patients had elevated ALT, this finding indicates that liver enzyme abnormalities in patients with PCOS and no known pre-existing liver disease should prompt further investigations, including tests for etiologies of chronic liver disease and subsequent referral for TE examination to evaluate the degree of liver fibrosis. Indeed, in our cohort 21.7% of patients with elevated ALT had significant liver fibrosis on TE examination, compared to only 2.6% of patients with normal ALT. On the other hand, 60% of the patients with NAFLD had normal ALT. These figures are in line with data from the general population and suggest the development of NAFLD may be occult[58,59]. This finding emphasizes the need for sensitive diagnostic tools in this at-risk population. Currently, guidelines recommend routine screening strategies for NAFLD in at-risk individuals, such as those with type 2 diabetes and metabolic comorbidities, particularly in case of elevated ALT[5,6]. It is further recommended that at-risk populations should be looked for liver fibrosis using non-invasive markers (serology-based or TE) to quantify the risk of progression to liver cirrhosis[2]. A similar strategy may be applicable in patients with PCOS, whereby those with obesity, elevated ALT or hyperandrogenism should undergo liver fibrosis assessment.
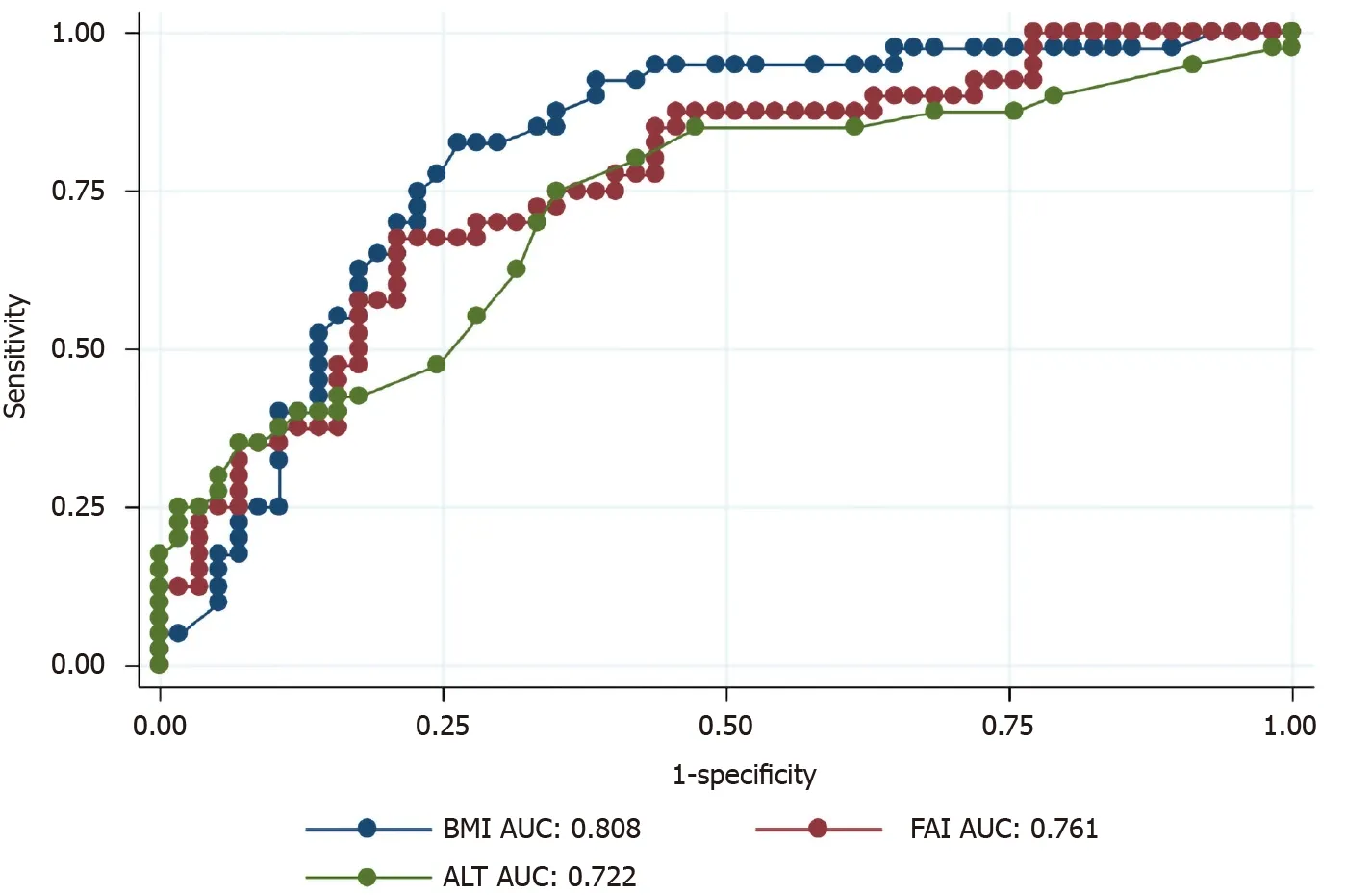
Figure 5 Area under the curve of body mass index, free androgen index and alanine aminotransferase for prediction of nonalcoholic fatty liver disease. BMI: Body mass index; ALT: Alanine aminotransferase; AUC: Area under the curve; FAI: Free androgen index.
We found that young South Asian patients with PCOS and NAFLD have an increased lifetime risk of atherosclerotic cardiovascular risk. Emerging data support the concept that NAFLD is a multisystem disease affecting a variety of extra-hepatic organ systems. Recent evidences indicate an increased risk of all-cause mortality and a strong link between NAFLD and extra-hepatic diseases, such as cardiovascular disease, hypothyroidism and sleep apnea[60]. Cardiovascular disease risk prediction in younger female patients has been more challenging than in older or male patients. Decisions to implement primary prevention measures are often consequently hindered in this patient population. Our study sheds new insights in the understanding of cardiovascular risk profile in young female population from NAFLD perspective. Our findings should be taken into consideration for risk stratification, especially after transition of women with PCOS to menopause, and for consideration of statin therapy.
Our study presents with several strengths, including the well-characterized homogeneous population and the use of a validated and accurate diagnostic method. The enrollment of consecutive patients minimizes the risk of selection bias. Some limitations of our study should be acknowledged. First, the cross-sectional study design did not allow us to capture the dynamics and associated factors of the disease in a longitudinal fashion. Second, the unavailability of genetic variants of the patatinlike phospholipase domain-containing 3 and other polymorphisms linked to hepatic steatosis prevented us from understanding their contribution to the pathogenesis of NAFLD in PCOS. Third, we included only South Asian women, so we cannot speculate on applicability of our findings to other ethnicities. Fourth, we did not include a group of age-matched patients without PCOS to act as control group. Finally, our study was carried out at a tertiary care centre, which may limit generalizability of our findings.
CONCLUSION
In conclusion, NAFLD diagnosed by TE with CAP is a frequent comorbidity in young South Asian women with PCOS without known liver disease. Obesity and hyperandrogenism seem the main associated factors. NAFLD can also progress to significant liver fibrosis, pointing towards the coexistence of NASH. Considering the young age of this population, these data suggest that monitoring for liver disease should be proposed in South Asian women with PCOS in case of obesity, elevated ALT, or hyperandrogenism. Early diagnosis of NAFLDvianon-invasive screening tools may help prompt initiation of interventions, including life-style modification, hepatology specialized care and cardiovascular risk stratification. Future longitudinal studies should assess the effect of early diagnosis and interventions on long-term outcomes.
ARTICLE HIGHLIGHTS

ACKNOWLEDGEMENTS
Part of this work has been presented at the Liver Meeting of the American Association for the Study of Liver Diseases 2019 (Boston, United States). Giada Sebastiani is supported by a Junior 1 and 2 Salary Award fromFonds de la Recherche en Santé du Québec(n 27127 and 267806).
猜你喜欢
进出口经理人(2020年11期)2020-11-24
进出口经理人(2020年10期)2020-11-17
北京航空航天大学学报(2019年9期)2019-10-26
福建基础教育研究(2019年7期)2019-05-28
数学学习与研究(2018年15期)2018-11-12
上海师范大学学报·自然科学版(2018年3期)2018-05-14
人力资源(2016年10期)2016-11-30
数学大王·中高年级(2016年7期)2016-09-03
都市丽人(2015年4期)2015-03-20
汽车零部件(2014年1期)2014-09-21
 World Journal of Gastroenterology2020年44期
World Journal of Gastroenterology2020年44期
- World Journal of Gastroenterology的其它文章
- Prognostic value of changes in serum carcinoembryonic antigen levels for preoperative chemoradiotherapy response in locally advanced rectal cancer
- Development and validation of a three-long noncoding RNA signature for predicting prognosis of patients with gastric cancer
- Use of the alkaline phosphatase to prealbumin ratio as an independent predictive factor for the prognosis of gastric cancer
- Active tuberculosis in inflammatory bowel disease patients under treatment from an endemic area in Latin America
- Associations between serum uric acid and hepatobiliary-pancreatic cancer: A cohort study
- COVID-19 in a liver transplant recipient: Could iatrogenic immunosuppression have prevented severe pneumonia? A case report