
Kasai手术对胆道闭锁儿童行活体肝移植术的影响
2016-07-30 06:19李姗霓王凯马楠孟醒初张威孙超董冲吴斌韩潮覃红高伟
天津医药 2016年7期
李姗霓,王凯,马楠,孟醒初,张威,孙超,董冲,吴斌,韩潮,覃红,高伟
Kasai手术对胆道闭锁儿童行活体肝移植术的影响
李姗霓*,王凯*,马楠,孟醒初,张威,孙超,董冲,吴斌,韩潮,覃红,高伟△
摘要:目的评价肝门-空肠吻合术(Kasai手术)对胆道闭锁儿童行活体肝移植术治疗效果及预后的影响。方法对2006年9月—2014年9月实施的150例活体肝移植患者资料进行回顾性分析,其中90例受者先行Kasai手术,后接受活体肝移植(Kasai组);60例受者直接接受活体肝移植(非Kasai组)。比较2组受者的一般资料、术后并发症和累积生存率的差异。结果受者年龄为4.9~87.0个月。Kasai组受者在移植时的移植月龄、体质量、身高均高于非Kasai组,而儿童终末期肝病(PELD)评分、术前胆红素水平则低于非Kasai组(均P<0.05)。2组移植物质量与受者体质量比(GRWR)、手术时间、术中失血量比较差异无统计学意义(均P>0.05)。2组受者的肺感染、急性排斥反应、门静脉吻合口狭窄、门脉血栓、肝动脉闭塞、胆漏、胆肠吻合口狭窄等发生率差异无统计学意义(均P> 0.05)。Kasai组肝移植术后总体并发症发生率为61.1%,高于非Kasai组的43.3%(χ2=4.580,P=0.032)。全部患者中死亡7例(4.7%),其中Kasai组6例(4.0%),5例为多器官功能衰竭,1例严重的肺感染;非Kasai组1例(0.7%),因术前消化道出血急诊手术死于多器官功能衰竭。供者均无严重并发症及死亡。全部受者术后1个月、1年、3年和5年累积生存率分别为98.6%、96.6%、94.9%,92.7%。其中,Kasai组分别为98.9%、96.5%、93.8%、91.3%;非Kasai组分别为98.3%、96.6%、96.4%、95.5%,2组比较差异无统计学意义(χ2=1.490,P=0.222)。结论胆道闭锁患者在Kasai术后行活体肝移植术可获得满意的临床效果,不会增加移植术后主要并发症的发生率及死亡比例,长期生存率与未接受Kasai手术的患者相当。且Kasai手术可推迟行肝移植的时间、利于儿童生长发育、减轻移植术前黄疸。
关键词:胆道闭锁;肝移植;Kasai手术;儿童
基金项目:国家自然科学基金资助项目(81570592)
作者单位:天津市第一中心医院小儿肝移植科,东方器官移植中心(邮编300192)
*并列第一作者;作者简介:李姗霓(1977),女,博士,副主任医师,主要从事儿童肝移植术后管理及随访工作;王凯(1978),男,博士,副主任医师,主要从事成人及儿童肝移植与移植免疫相关研究
△
通讯作者E-mail:gao-wei@medmail.com.cn
胆道闭锁(biliary atresia,BA)是新生儿胆道进行性炎性梗阻性疾病[1],以肝外胆管的完全性梗阻或同时伴有肝内胆道梗阻为特征,如不能及时有效治疗可导致肝功能衰竭,是儿童肝移植最常见的适应证之一[2-3]。目前,治疗BA最有效的方法是肝门-空肠吻合术(Kasai手术)和肝脏移植。Kasai手术于1959年首次实施,可明显延长BA患儿的存活率,文献报告Kasai术后患者自体肝20年存活率为21%~44%[4-6]。但长期存活的患者在疾病的后期仍需行肝移植手术。Kasai手术失败后再行肝移植手术,是目前多数学者推荐的BA的治疗方案。然而早期的Kasai手术是否会影响后期的肝移植手术效果,目前鲜有报道。本文通过回顾性分析我院150例活体肝移植治疗BA患儿的临床资料,探讨既往Kasai手术史对患者活体肝移植手术效果及预后的影响。
1 资料与方法
1.1供者和受者的选择收集2006年9月—2014年9月于天津市第一中心医院初次行活体肝移植手术的BA患儿150例,其中男91例,女59例,月龄4.9~87.0个月,体质量4.5~27.5 kg。所有供者均是患儿三代以内的直系亲属,均为自愿捐肝,均符合医学供者标准并通过了天津市第一中心医院伦理委员会审批。根据肝移植前是否接受Kasai手术,分为Kasai组90例和非Kasai组60例。
1.2手术方法
1.2.1术前准备及手术流程完善术前常规血液学与影像学评估。手术当日禁食水,麻醉后取肋缘下弧形切口入腹(既往行Kasai手术者原则上在原有瘢痕基础上延伸切口)。所有移植物均使用供者的左外侧叶肝脏(Ⅱ、Ⅲ段),手术方式采用背驮式肝移植术。胆道重建采用Roux-en-Y肝空肠吻合术。术者均为同一肝移植治疗组。
1.2.2血管重建方法门静脉长度足够时,行门静脉主干对端吻合。如供、受体门静脉直径差别较大,可用受体门静脉左右分支分叉部静脉片与供体门静脉进行吻合。如供体门静脉足够长,可用受体脾静脉和肠系膜上静脉汇合部与供体门静脉进行吻合。如供体门静脉较短,供、受体门静脉直接吻合张力过大或长度不够,可用间置血管搭桥。如受体门静脉直径较细或有血栓,可将门静脉纵行剖开,用静脉补片扩大门静脉直径。间置血管或静脉补片来源可以为尸体髂静脉或供体脐静脉。动脉采用显微外科技术重建肝动脉。
1.2.3术后管理术后免疫抑制方案为二联免疫抑制,即他克莫司联合甲基氢化泼尼松。他克莫司的初始剂量为0.10~0.15 mg/(kg·d),术后第1个月将浓度维持在7~9 mg/L,以后维持在5~8 mg/L。甲基氢化泼尼松的初始剂量为4 mg/(kg·d),随后逐渐减量,术后3个月或半年逐渐停止使用。术后常规华法林抗凝治疗,国际标准化比值(international normalized ratio,INR)维持在1.5~2.0。术后于重症监护室(ICU)观察3~5 d,约3周后出院。术后3个月内隔周复查,3个月至半年每月复查1次,半年后复查间期延长至3个月1次,以后视情况3~6个月复查1次。监测指标主要为血常规、肝功能、凝血、他克莫司血药浓度,移植超声监测移植肝血流情况。
1.3统计学方法采用SPSS 18.0软件进行统计学分析。正态分布的计量资料以均数±标准差(±s)表示,组间比较采用t检验;偏态分布的计量资料以M(P25,P75)表示,组间比较采用Mann-Whitney U检验;率的比较采用χ2检验;Kaplan-Meier用于统计受者生存率,Log-rankχ2检验用于比较累积生存率。P<0.05为差异有统计学意义。
2 结果
2.1受者一般资料全部患儿进行手术时的月龄为4.9~84.0个月,中位数8.40(6.80,12.33)个月。Kasai组患儿接受肝移植时的月龄、体质量、身高高于非Kasai组,术前儿童终末期肝病(pediatric end stage of liver disease,PELD)评分、胆红素水平低于非Kasai组(P<0.05)。2组受者移植物质量与受者体质量比(graft to recipient body weight ratio,GRWR)、手术时间、术中失血量等差异无统计学意义(P>0.05),见表1。
2.2供者一般资料150例供者中,男60例,女90例,年龄24~47岁,平均(28.7±5.6)岁。供肝脂肪肝12例(8%),脂肪变性比例均<25%,肝功能正常。其中2例(1.3%)术后发生胆漏,1例手术处理,1例穿刺引流均痊愈。1例(0.7%)发生肝脏血肿,外科处理后痊愈出院。截至随访结束,所有供者均无严重并发症出现,均健康存活。
2.3受者肝移植术后并发症情况Kasai组主要并发症为肺感染。非Kasai组以肝动脉闭塞发生率最高。所有患儿均未在围手术期内出现胆道并发症。2组受者的肺感染、急性排斥反应、门静脉吻合口狭窄,门脉血栓、肝动脉闭塞、胆漏、胆肠吻合口狭窄等发生率比较,差异无统计学意义(均P>0.05),见表2。Kasai组肝移植术后总体并发症发生率为61.1%(55/90),高于非Kasai组的43.3%(26/60),差异有统计学意义(χ2=4.580,P=0.032)。

Tab.1 Comparison of general data between two groups 表1 2组受者一般资料比较
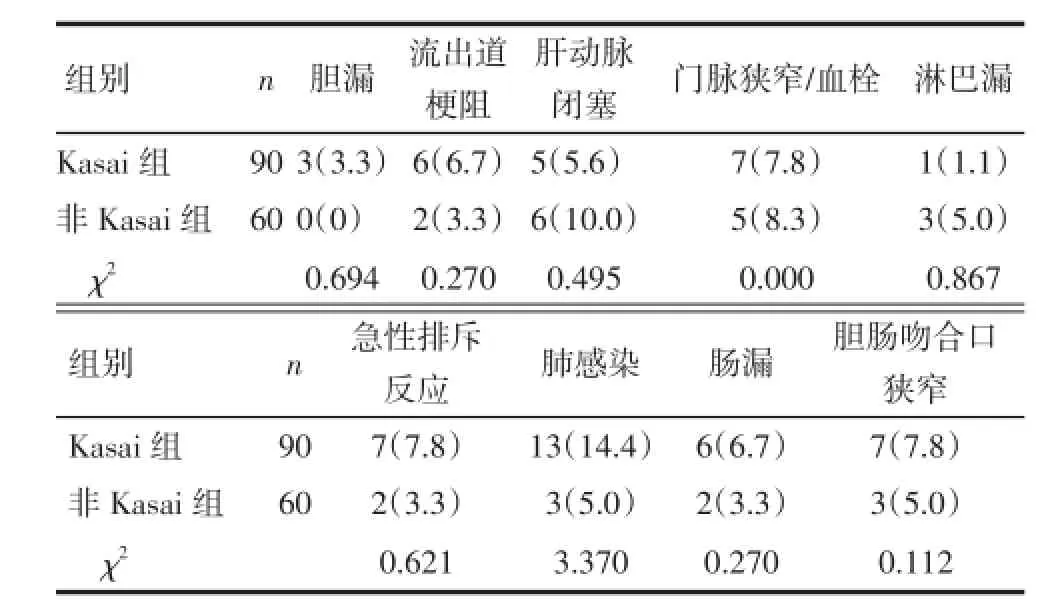
Tab.2 Comparison of complications in patients between two groups表2 2组患儿肝移植术后并发症情况比较 例(%)
2.42组受者生存率比较在随访期间,150例受者死亡7例(4.7%),其中Kasai组6例(4.0%),5例死于多器官功能衰竭,1例死于严重的肺感染;非Kasai组1例(1.7%)因术前消化道出血急诊手术死于多器官功能衰竭。全部受者术后1个月、1年、3年和 5年累积生存率分别为98.6%(149/150)、96.6%(140/145)、94.9%(129/136)、92.7%(115/ 124)。Kasai组术后不同时间累积生存率分别为98.9%(89/90)、96.5%(83/86)、93.8%(76/81)、91.3% (73/80);非Kasai组分别为98.3%(59/60)、96.6% (57/59)、96.4%(53/55)、95.5%(42/44),2组生存率比较差异无统计学意义(Log-rank χ2=1.490,P= 0.222)。
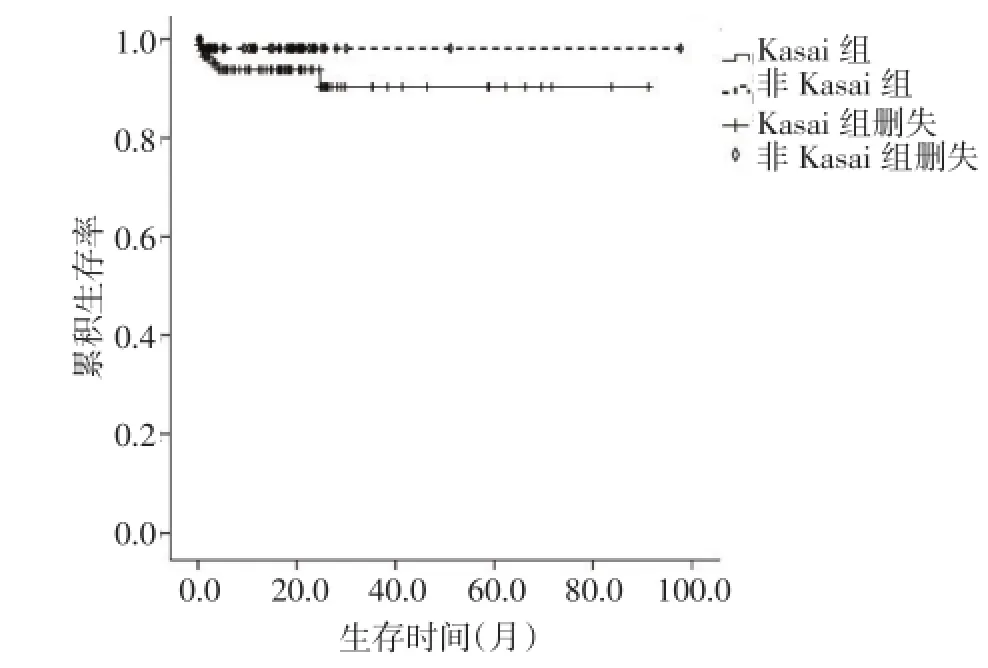
Fig.1 Survival curves of patients图1 2组患儿生存曲线
3 讨论
BA以胆道系统进行性炎症和纤维性梗阻为特征,继发黄疸、胆汁性肝硬化,其发病率约1/10 000~ 1/8 000,约占儿童肝移植的50%[3,7]。Kasai手术的出现虽然在一定程度上提高了BA患者的生存率,大多数患者最终仍需要接受肝移植。因此,在肝移植时代,对于BA患者,Kasai手术的价值与意义尚存争议。
除肝移植术外,Kasai手术是治疗儿童BA最有效的方式。有研究认为Kasai术后黄疸清除率可达45.6%,1年和2年的自体肝生存率分别为53.7%和46.7%[8]。肝移植术前先期接受Kasai手术的优势在于部分儿童在Kasai术后恢复生长发育,体质量增加,有利于提高肝移植的成功率,甚至部分患儿可长期生存,从而避免了行肝移植术。
虽然Kasai术后会不可避免出现腹腔粘连,增加手术时间和出血风险,但其并不会增加手术并发症的发生率及影响远期存活。本组全部受者中无论是Kasai组还是非Kasai组的患者,术后1年、3年和5年的累积生存率均在90%以上,这说明Kasai手术并不影响患者的近期及远期生存率。有研究认为,相比于无手术史的患者,在移植术前接受Kasai手术的患者肝移植围手术期并发症、二次手术发生率没有差异[9-10]。而Kasai术后1年后行移植手术的患者中,其总体并发症发生率要低于未行Kasai手术的患儿[11]。Wang等[10]在对28例患儿分析中认为,行Kasai手术与直接行活体肝移植的患儿在手术时间、出血量等方面的差异无统计学意义。
本研究中,全部患者均未在围手术期内出现胆道并发症。2组受者在门静脉吻合口狭窄、门脉血栓、肝动脉闭塞、胆道并发症、肺部感染、急性排斥反应等发生率均相似。作为儿童肝移植并发症中较为常见的肝动脉血栓形成,大部分患者的肝功能因再通或侧枝循环的建立而肝功能逐渐恢复,未出现死亡病例。同时,由于我中心采用显微镜下动脉吻合技术,手术精准,使得肝动脉血栓形成的发生率明显低于其他中心。需要特别指出的是,Kasai术后胆管炎是影响预后的一个重要因素。在肝移植术前,反流性胆管炎发生次数越多,肝纤维化程度越重,进而会出现门脉高压,甚至出现消化道出血。此外,早期的胆管炎还可能引起肝门部胆管梗阻,加重淤胆。
本研究还发现,接受过Kasai手术的患者在肝移植时的月龄要大于非Kasai患者,且身体的生长发育更充分,而术前的胆红素水平也低于非Kasai患者。这与Superina等[8]的研究结果一致,充分说明了Kasai手术对于肝移植的积极作用,可改善受者的术前状态,在某种程度上必然会降低肝移植的手术风险,减少外科并发症的发生概率。
总之,尽管Kasai手术会因可能发生腹腔粘连而增加肝移植术的手术难度,但其有助于改善BA患儿术前状态,促进生长发育,对于肝移植具有一定的积极意义。在目前我国的实际国情下,先期行Kasai手术,在出现终末期肝硬化失代偿期后再行肝移植术,这种“序贯”治疗,有助于BA患儿的长期生存。
参考文献
[1]Pintér AB,Farkas A,Par A,et al.A long-term follow-up of five patients with atresia of the common bile duct[J].J Pediatr Surg,2004,39(7): 1050-1054.
[2]Chiu CY,Chen PH,Chan CF,et al.Biliary atresia in preterm infants inTaiwan:a nationwide survey[J].J Pediatr,2013,163(1):100-103. doi:10.1016/j.jpeds.2012.12.085.
[3]Jimenez-Rivera C,Jolin-Dahel KS,Fortinsky KJ,et al.International incidence and outcomes of biliary atresia[J].J Pediatr Gastroenterol Nutr,2013,56(4):344-354. doi:10.1097/ MPG.0b013e318282a913.
[4]Lykavieris P,Chardot C,Sokhn M,et al.Outcome in adulthood of biliary atresia:a study of 63 patients who survived for over 20 years with their native liver[J].Hepatology,2005,41(2):366-371.
[5]de Vries W,Homan-Van der Veen J,Hulscher JB,et al.Twentyyear transplant-free survival rate among patients with biliary atresia [J].Clin Gastroenterol Hepatol,2011,9(12):1086-1091.doi: 10.1016/j.cgh.2011.07.024.
[6]Shinkai M,Ohhama Y,Take H,et al.Long-term outcome of children with biliary atresia who were not transplanted after the Kasai operation:>20-year experience at a children’s hospital[J].J Pediatr Gastroenterol Nutr,2009,48(4):443-450.
[7]Devictor D,Tissieres P,Bicêtre Hospital Pediatric Transplant Group.Pediatric liver transplantation:where do we stand?Where we are going to?[J].Expert Rev Gastroenterol Hepatol,2013,7(7):629-641.doi:10.1586/17474124.2013.832486.
[8]Superina R,Magee JC,Brandt ML,et al.The anatomic pattem of biliary atresia identified at time of Kasai hepatoportoentrostomy and early postoperative clearance of jaundice are significant predictors of transplant-free survival[J].Ann Surg,2011,254(4):577-585.doi:10.1097/SLA.0b013e3182300950.
[9]Shneider BL,Brown MB,Haber B,et al.A multicenter study of the outcome of biliary atresia in the United States,1997 to 2000[J].J Pediatr,2006,148(4):467-474.
[10]Wang Q,Yan LN,Zhang MM,et al.The pre-Kasai procedure in living donor liver transplantation for children with biliary atresia [J].Hepatobiliary Pancreat Dis Int,2013,12(1):47-54.
[11]Alexopoulos SP,Merrill M,Kin C,et al.The impact of hepatic portoenterostomy on liver transplantation for the treatment of biliary atresia:early failure adversely affects outcome[J].Pediatr Transplant,2012,16(4):373-378.doi:10.1111/j.1399-3046.2012.01677.x.
(2016-04-05收稿2016-06-07修回)
(本文编辑李鹏)
中图分类号:R617
文献标志码:A
DOI:10.11958/20160239
Effects of Kasai surgery on living donor liver transplantation in the treatment of children biliary atresia
LI Shanni*,WANG Kai*,MA Nan,MENG Xingchu,ZHANG Wei,SUN Chao,DONG Chong,
WU Bin,HAN Chao,QIN Hong,GAO Wei△
Department of Pediatric Transplant of Tianjin First Center Hospital,Oriental Organ Transplant Center,Tianjin 300192,China
△Corresponding AuthorE-mail:gao-wei@medmail.com.cn
Abstract:ObjectiveTo evaluate the effects of portoenterostomy(Kasai surgery)on living donor liver transplantation (LDLT)for children with biliary atresia(BA).MethodsA total of 150 children with BA,who were treated with LDLT in our center from September 2006 to September 2014,were retrospectively analysed.The children were categorized into Kasai group(90 cases,60%)and non-Kasai(60 cases,40%)group,based on whether they had previously undergone Kasai procedure pre-LDLT.Clinical data,incidence of complications and accumulated survival rates were compared between two groups.ResultsThe ages of pediatric patients were 4.9-87.0 months.The patient age and height were significantly higher in Kasai group than those of non-Kasai group(P<0.05).The serum bilirubin level was lower before surgery in Kasai group than that of non-Kasai group(P<0.05).There were no significant differences in body weight,pediatric end stage of liver disease(PELD)score,graft to recipient body weight ratio(GRWR),operation time and blood loss between two groups(P> 0.05).Similarly,there were no significant differences in pulmonary infection,acute rejection,portal vein thrombosis,hepatic artery occlusion and biliary complications between the two groups(P>0.05).The overall complication rate of post-LDLT was 61.1%in Kasai group,which was higher than that in non-Kasai group(43.3%,χ2=4.580,P=0.032).Totally,there were 7 cases(4.7%)died on post-LDLT,in which there were 6 cases(4.0%)in Kasai group including 5 cases of multiple organfailure and 1 case of severe pulmonary infection,and 1 case(0.7%)in non-Kasai group,who died of multiple organ failure due to preoperative gastrointestinal bleeding for emergency surgery.There were no serious complications and death in donors.The overall cumulative survival rates were 98.6%,96.6%,94.9%and 92.7%in 1 month,1 year,3 years and 5 years after LDLT,respectively.And there were no significant differences in survival rates in 1 month,1 year,3 years and 5 years between two groups(χ2=1.490,P=0.222)with the rates of 98.9%,96.5%,93.8%,91.3%in Kasai group and 98.3%,96.6%, 96.4%,95.5%in non-Kasai group.ConclusionPerforming Kasai procedure can acquire satisfied results to pediatric patients with BA pre-LDLT,without increasing the incidence of major complications and mortality post-LDLT.And the accumulated survival rate is not different in pediatric patients received Kasai surgery compared with that in non-Kasai patient.Besides that,Kasai surgery might postpone the time of receiving LDLT,benefit to the growth of children and reduce the jaundice of pre-LDLT.
Key words:biliary atresia;liver transplantation;Kasai surgical;child
猜你喜欢
少儿美术·书法版(2021年11期)2021-10-20
少儿美术·书法版(2021年8期)2021-10-20
天津医科大学学报(2021年1期)2021-01-26
华人时刊(2020年21期)2021-01-14
杂文选刊(2016年7期)2016-08-02
小天使·一年级语数英综合(2016年6期)2016-05-14
中国药业(2014年19期)2014-05-17
中华移植杂志(电子版)(2012年3期)2012-08-15
中华移植杂志(电子版)(2010年4期)2010-02-09
小学生·新读写(2006年6期)2006-06-14
